



Circumferentially Comminuted Femoral Neck Fracture Managed with Percutaneous Reduction and Fixed Angle Implantation.
Score and Comment on this Case
Clinical Details
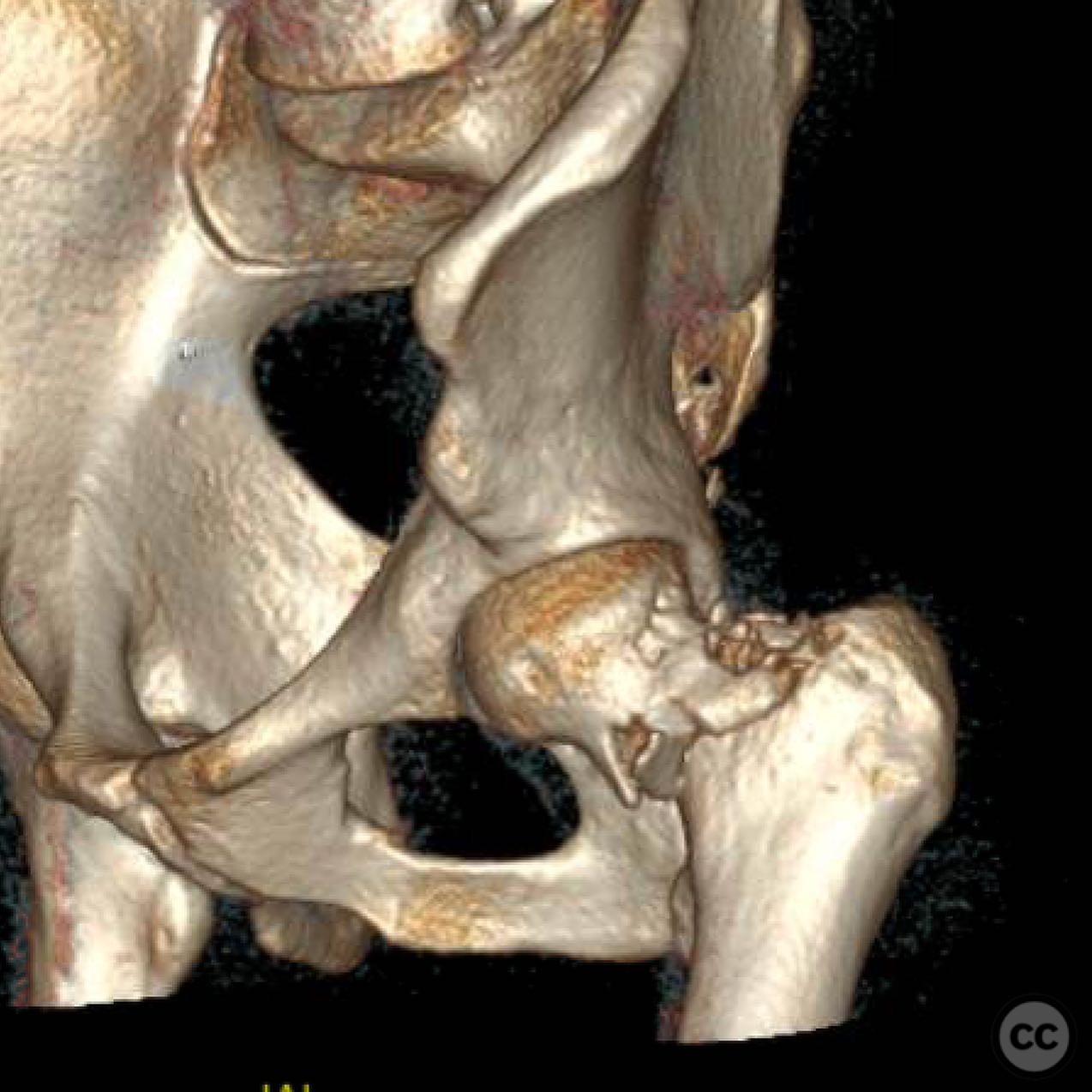
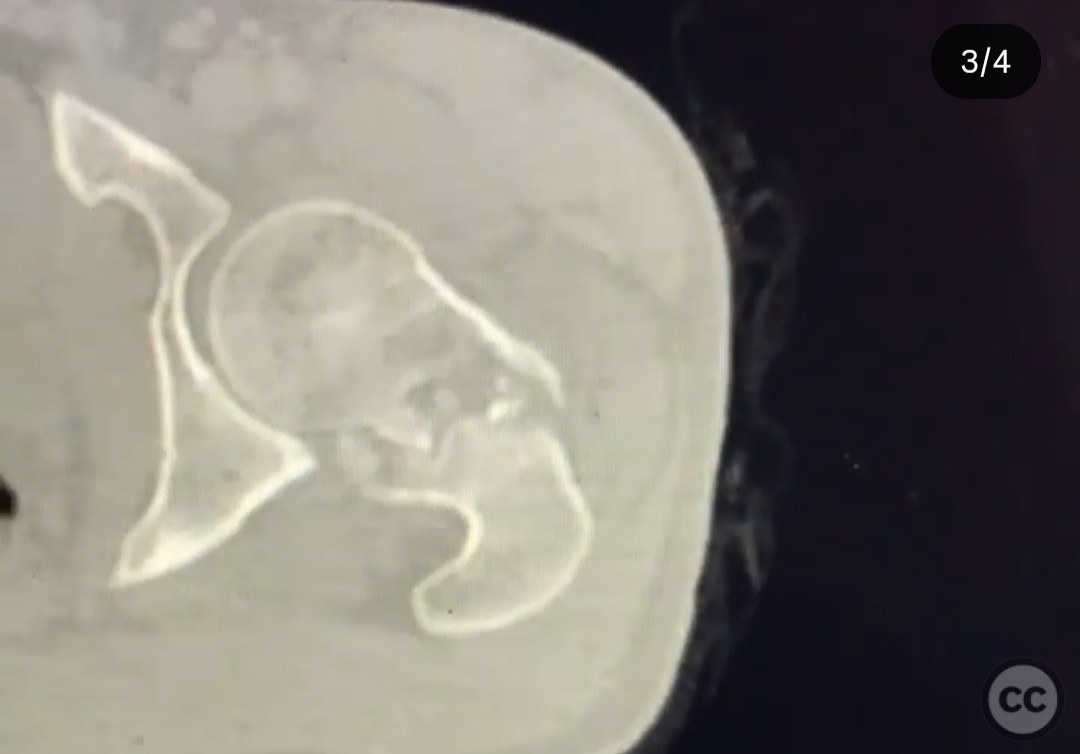
Clinical and radiological findings: A 23-year-old male presented following a motorcycle collision with a parked car, resulting in a circumferentially comminuted femoral neck fracture. The patient was otherwise healthy with no significant comorbidities. Initial radiographs and CT imaging confirmed the complex nature of the fracture, highlighting the comminution around the femoral neck. The neurovascular examination was unremarkable.
Preoperative Plan
Planning remarks: The preoperative plan involved a percutaneous reduction technique due to the circumferential comminution of the femoral neck, which diminished the value of a direct open approach. The goal was to restore proximal femoral morphology using closed or percutaneous manipulation, followed by stabilization with an anti-rotation screw, multiple wires, and a sliding hip screw side plate.
Surgical Discussion
Patient positioning: The patient was positioned supine on a flattop table, allowing for optimal manipulation and imaging access during the percutaneous reduction procedure.
Anatomical surgical approach: A percutaneous approach was utilized, involving small incisions for the insertion of instruments to achieve reduction and fixation. The anti-rotation screw and wires were placed percutaneously to stabilize the fracture fragments, followed by the application of a sliding hip screw side plate.
Operative remarks:The surgeon opted for a percutaneous reduction due to the circumferential comminution of the femoral neck, which made an open reduction less beneficial. The use of a fixed angle implant (sliding hip screw and side plate) was chosen based on emerging evidence suggesting its superiority over non-fixed angle constructs for this fracture type. The procedure was performed on a flattop table, which is the surgeon's preference for such cases.
Postoperative protocol: Postoperatively, the patient was instructed to engage in flat foot weight bearing of the leg only for three months to allow for adequate healing of the fracture.
Follow up: Not specified.
Orthopaedic implants used: Anti-rotation screw, multiple wires, sliding hip screw side plate (fixed angle).
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 315 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Circumferentially Comminuted Femoral Neck Fracture Managed with Percutaneous Reduction and Fixed Angle Implantation.. Journal of Orthopaedic Surgery and Traumatology. Case Report 47613165 Published Online Jul 21 2025.