




_1.jpg)
_0.jpg)





_3.jpg)
_2.jpg)

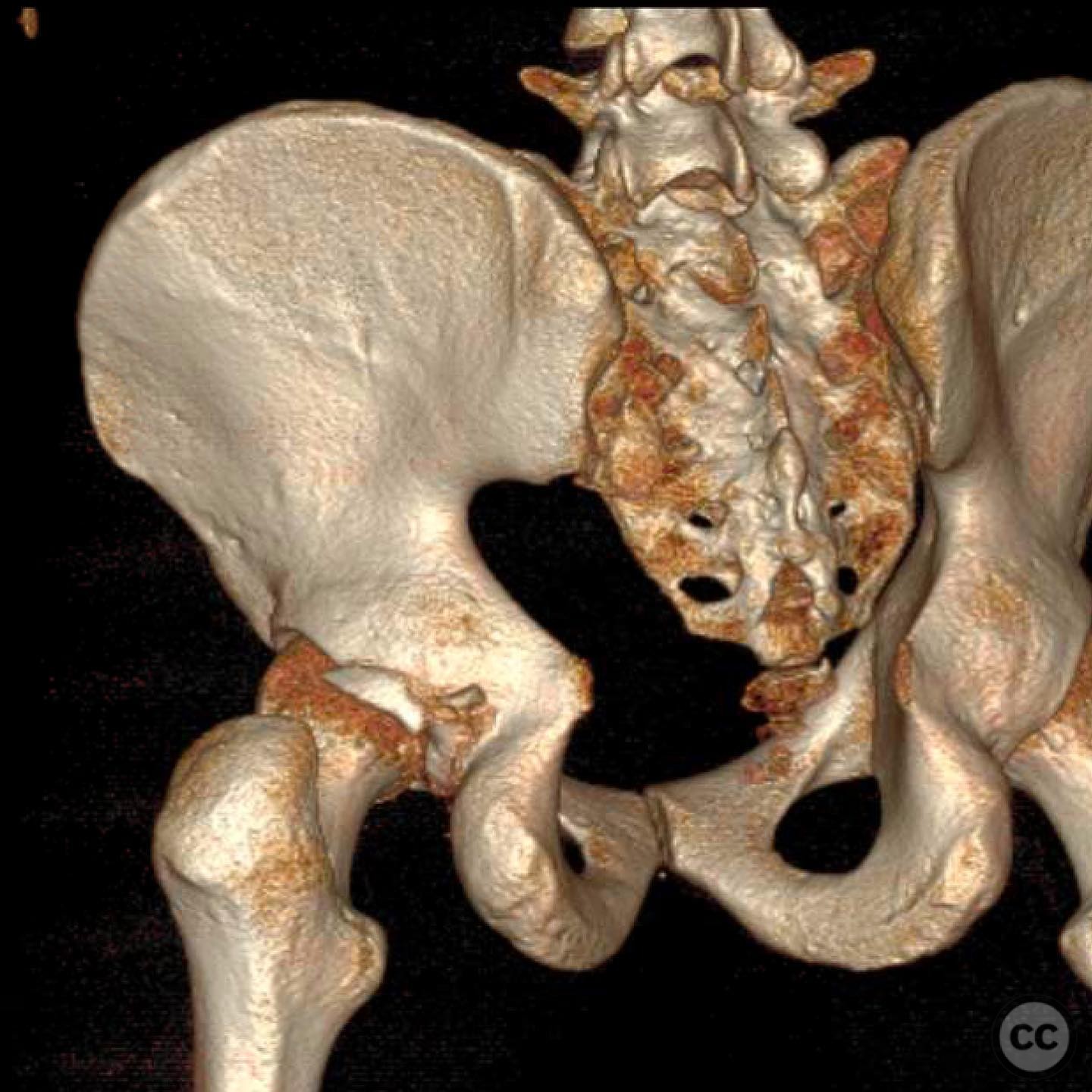
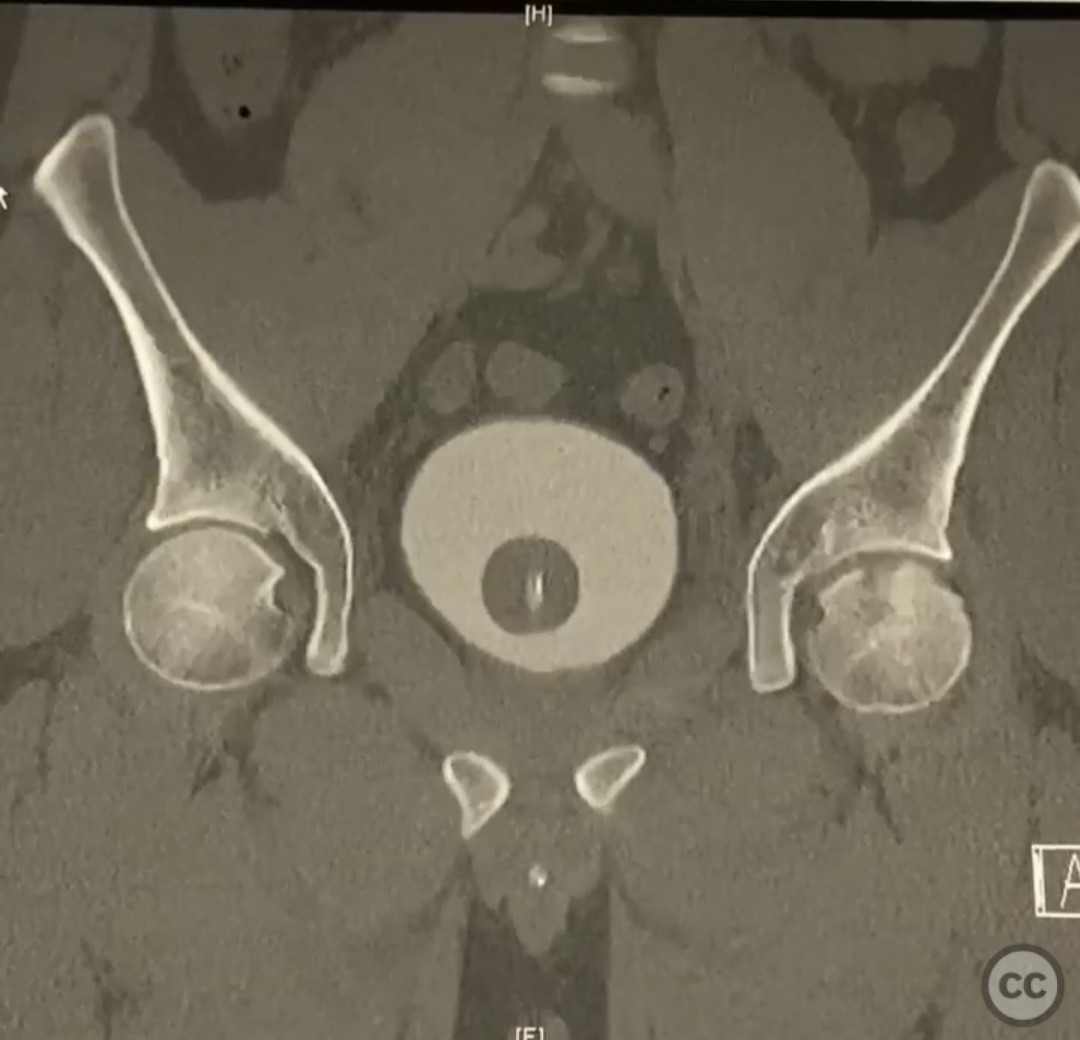
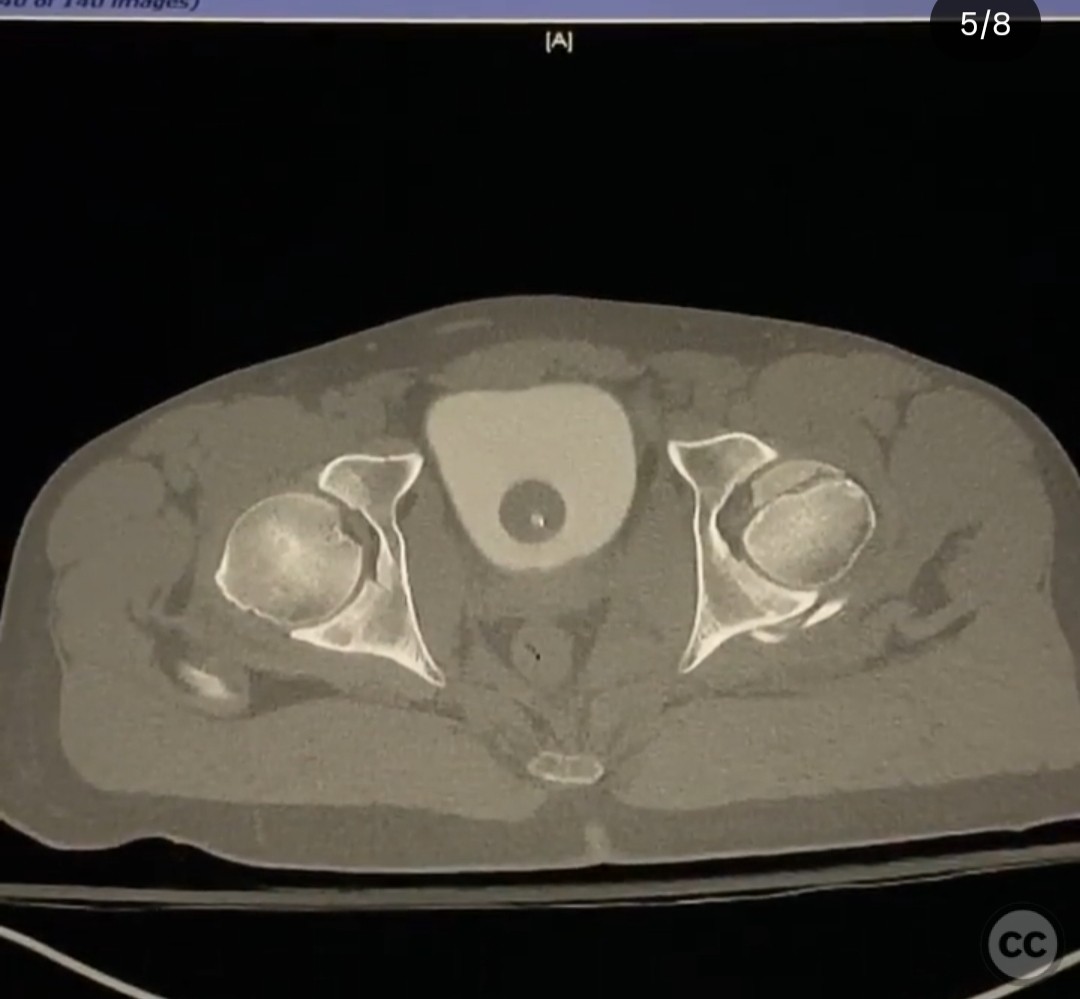
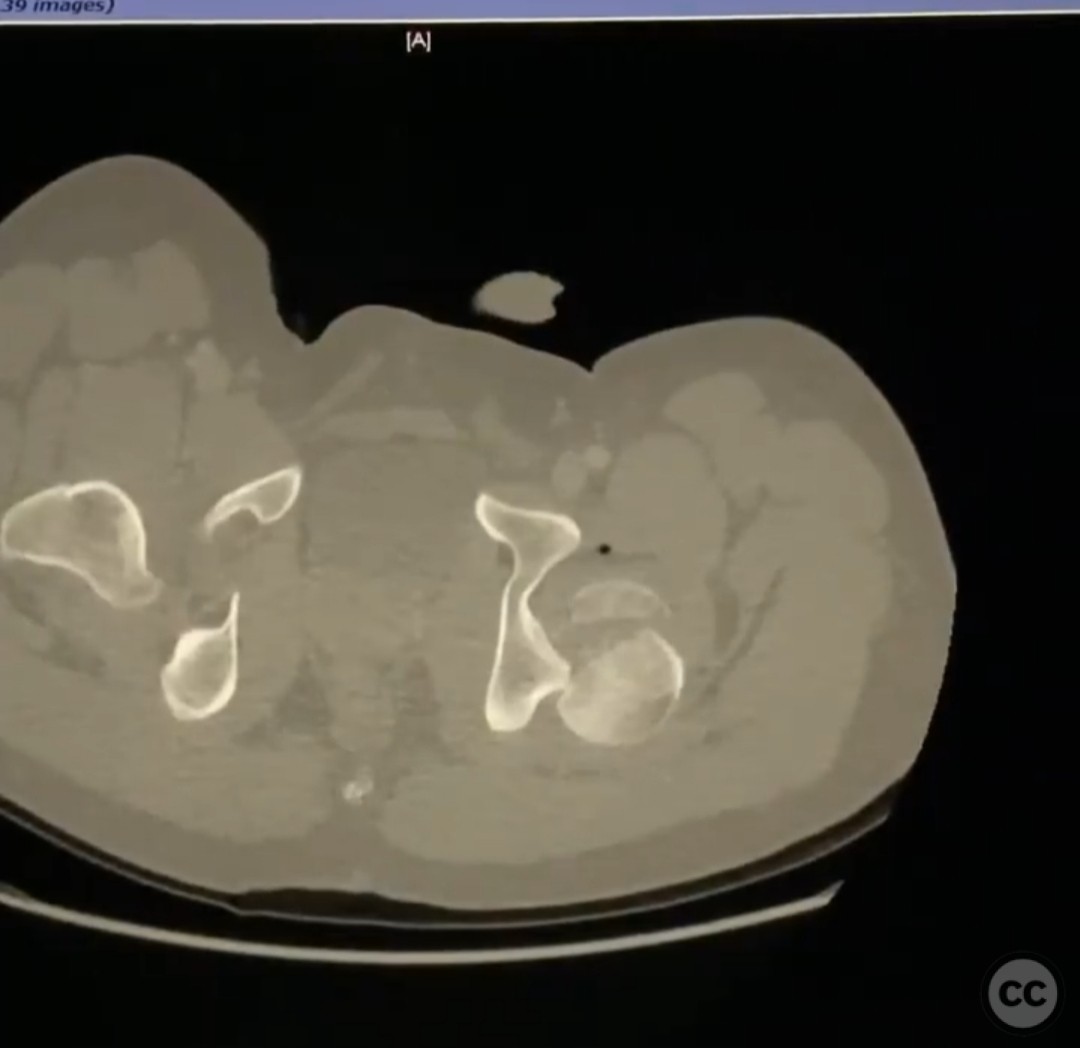
Pipkin IV Femoral Head Fracture Dislocation with Posterior Wall Involvement.
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A young male involved in a high-speed motorcycle accident presented with a Pipkin IV femoral head fracture dislocation. The dislocation pattern was atypical, occurring posteriorly with the leg in abduction and external rotation. This resulted in a fracture pattern through and above the fovea, with significant damage to the cranial weight-bearing surface of the femoral head. Initial management involved a successful closed reduction performed with careful maneuvers under attending supervision.
Preoperative Plan
Planning remarks: The preoperative plan involved addressing the femoral head fracture via an anterior approach, specifically the Heuter approach, to fix the head and assess stability through stress examination. The posterior approach was considered only if instability persisted post-fixation.
Surgical Discussion
Patient positioning: Supine positioning was utilized to facilitate access via the anterior approach, allowing for optimal exposure of the femoral head.
Anatomical surgical approach: An anterior Heuter approach was employed, involving an incision along the interval between the sartorius and tensor fascia latae muscles. Subperiosteal dissection was carried out to expose the hip joint capsule, followed by capsulotomy to access the femoral head for fracture fixation.
Operative remarks:The femoral head was fixed anteriorly, and a stress examination was conducted to assess stability. Despite initial confidence in stability post-fixation, the patient exhibited near dislocation during stress testing, indicating residual instability. Retrospective consideration suggested that a Gibson approach with a trigastric slide might have been more appropriate to address both the head and posterior wall/capsulolabral complex. However, this experience reinforced the current protocol of fixing from the front and addressing posterior instability only if necessary.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with crutches for six weeks, followed by gradual progression to full weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Orthopaedic implants used included screws for fixation of the femoral head fracture.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 353 times
16 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Pipkin IV Femoral Head Fracture Dislocation with Posterior Wall Involvement.. Journal of Orthopaedic Surgery and Traumatology. Case Report 41271650 Published Online Jul 16 2025.