







Pipkin IV Femoral Head Fracture with Posterior Wall Involvement and Femoral Neck Fracture.
Score and Comment on this Case
Clinical Details
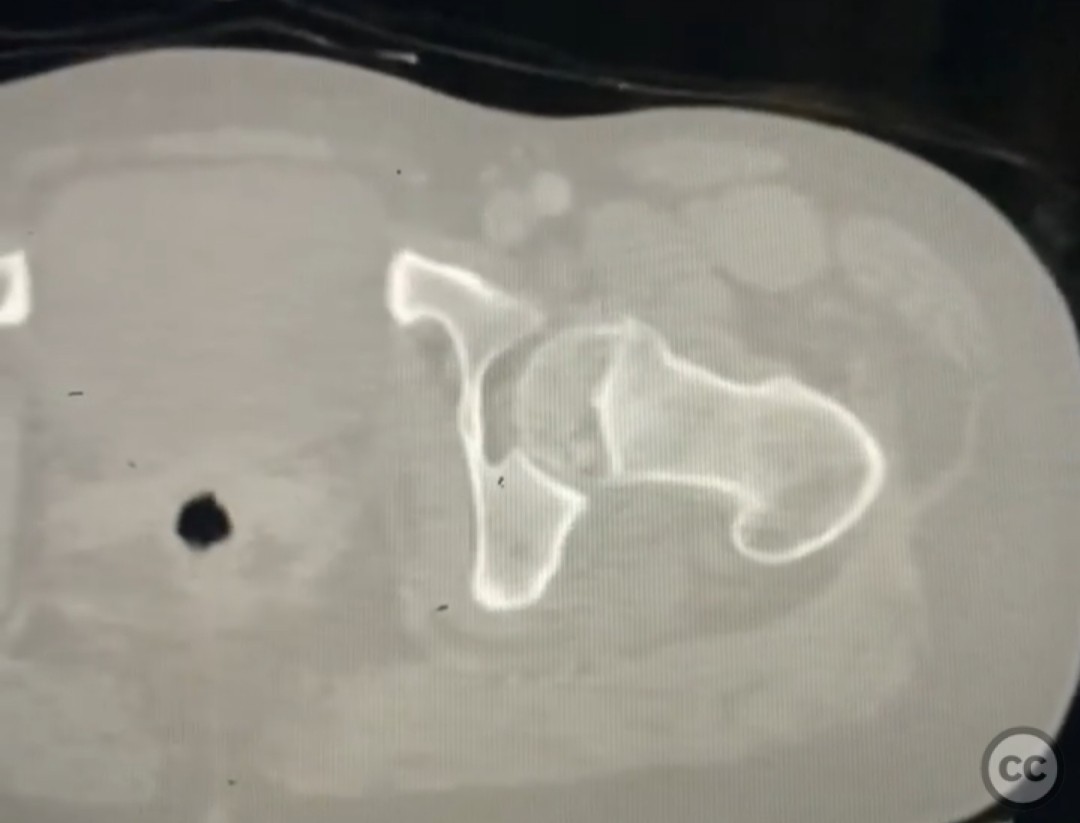
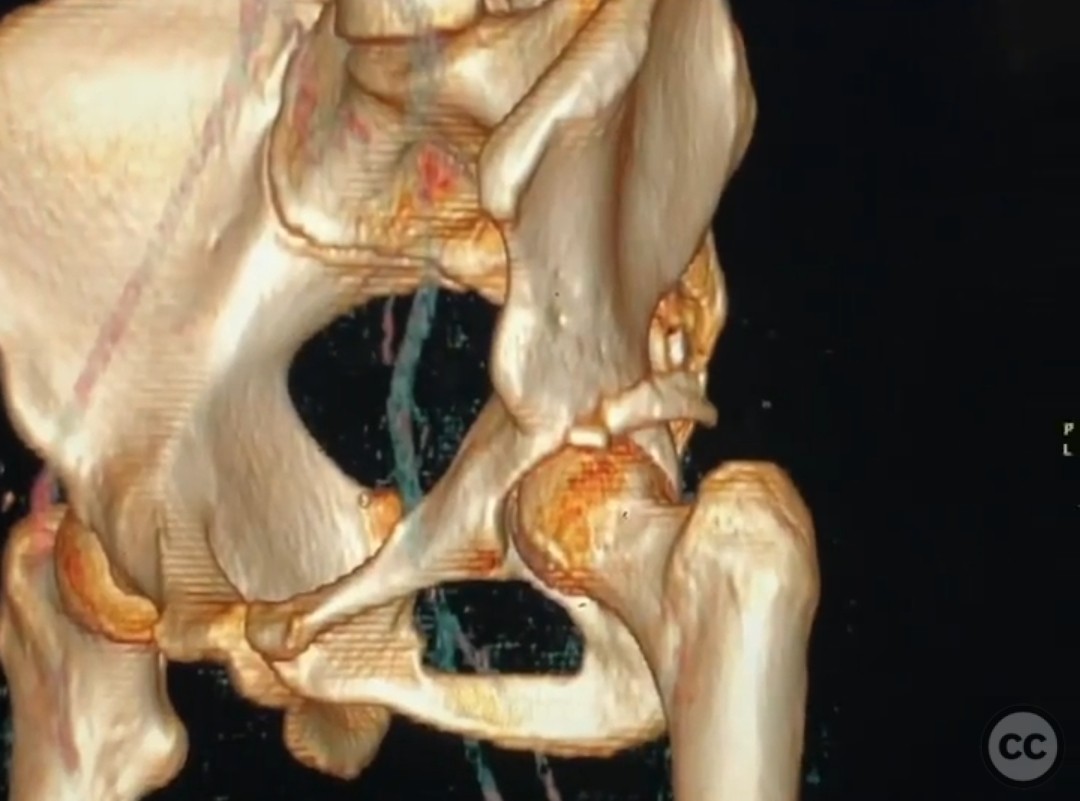
Clinical and radiological findings: A 33-year-old female involved in a motor vehicle collision presented with a posterior hip dislocation accompanied by a comminuted supra-foveal femoral head fracture, a cranial peripheral posterior wall fracture, and a non-displaced femoral neck fracture. The injury is associated with a risk of sciatic nerve palsy and avascular necrosis (AVN).
Preoperative Plan
Planning remarks: The preoperative plan involved a Gibson approach with a trigastric slide osteotomy for anterior dislocation to address the femoral head fracture. The intention was to reconstruct the femoral head using a femoral head allograft due to a 20% pie slice defect. The posterior wall was to be addressed through capsulolabral repair with suture anchors and spring plates.
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position to facilitate the Gibson approach and anterior dislocation of the hip.
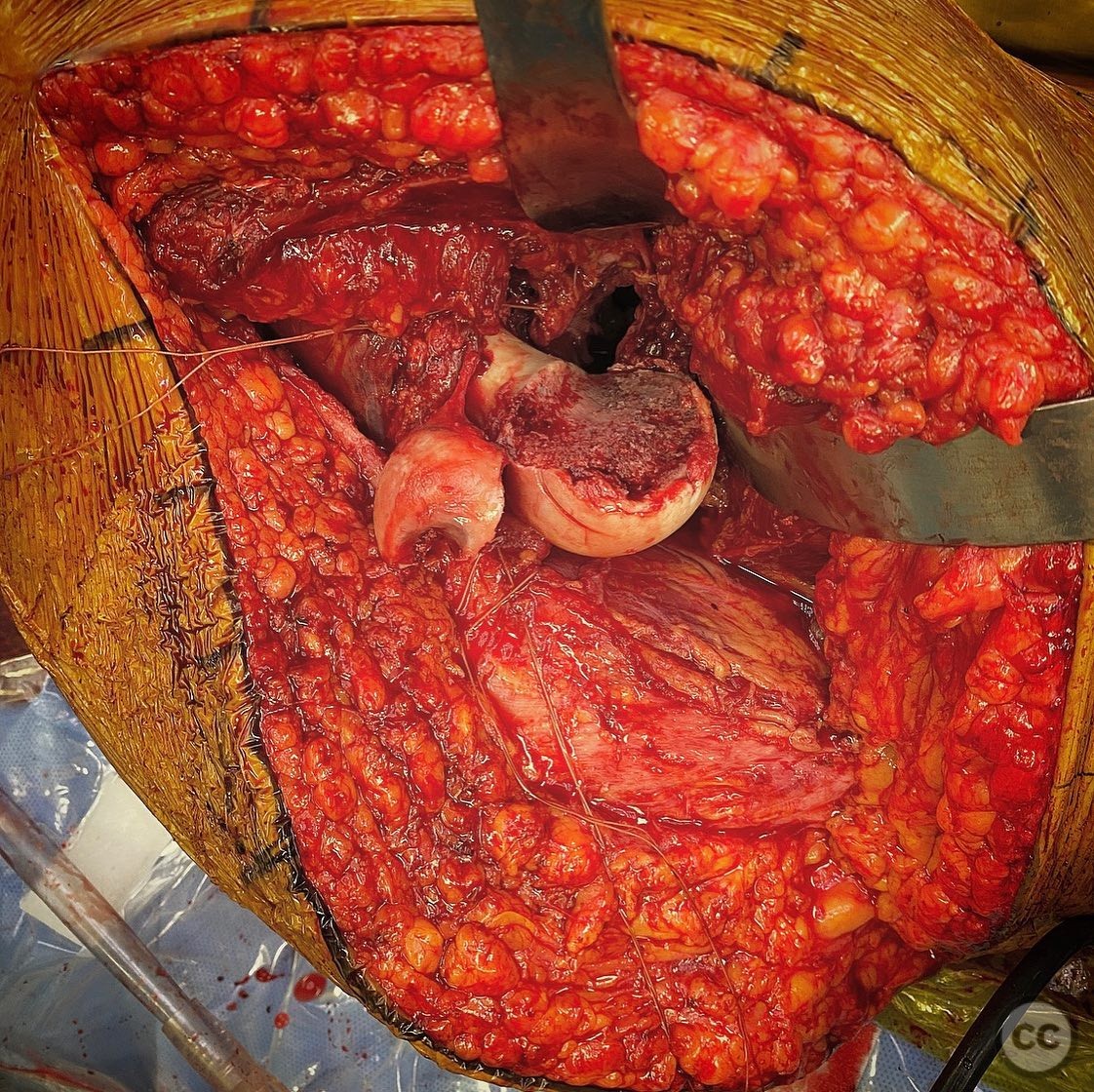
Anatomical surgical approach: A Gibson approach was utilized, involving a trigastric slide osteotomy to achieve anterior dislocation of the hip. This allowed access to the femoral head for reconstruction using an allograft. The posterior wall was accessed for capsulolabral repair.
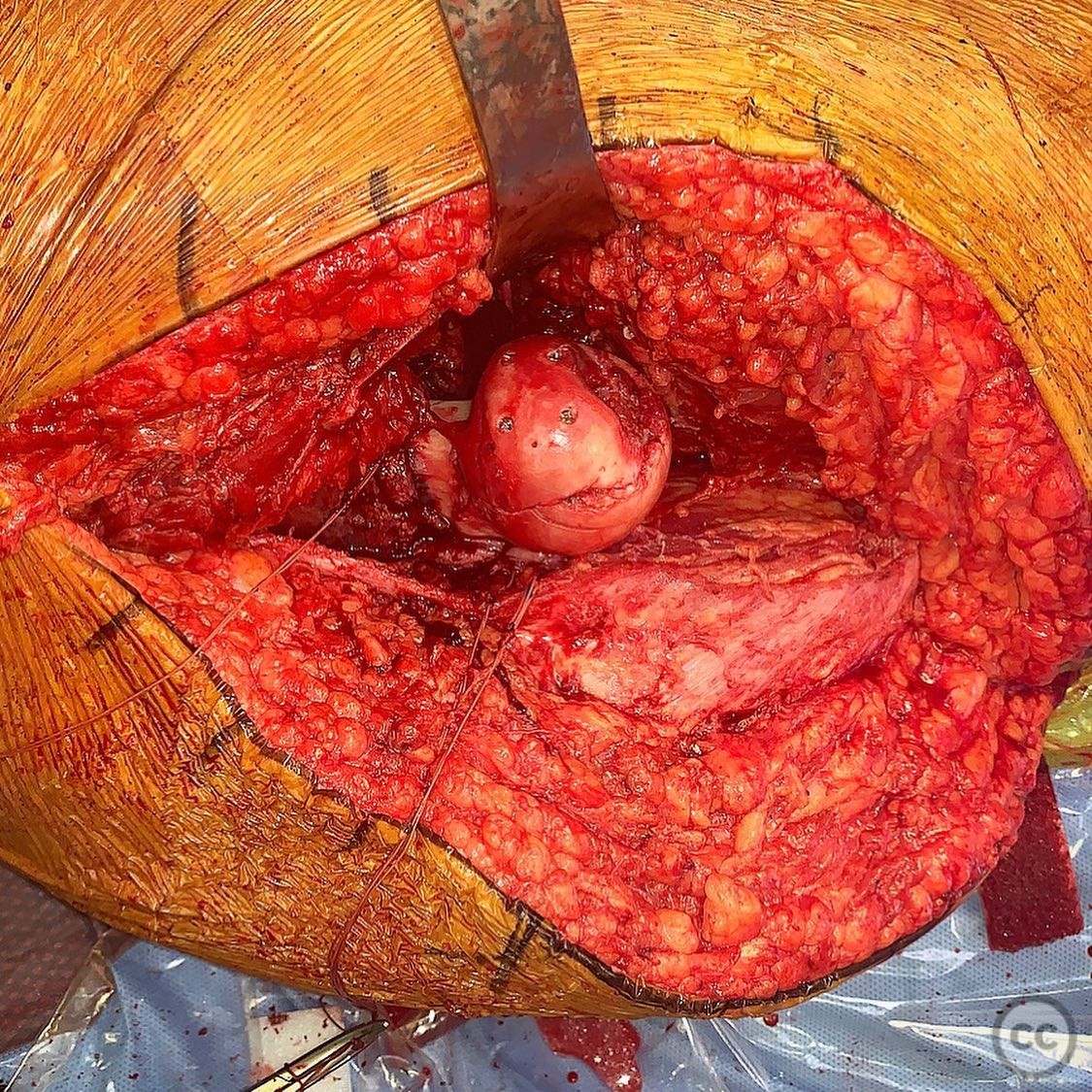
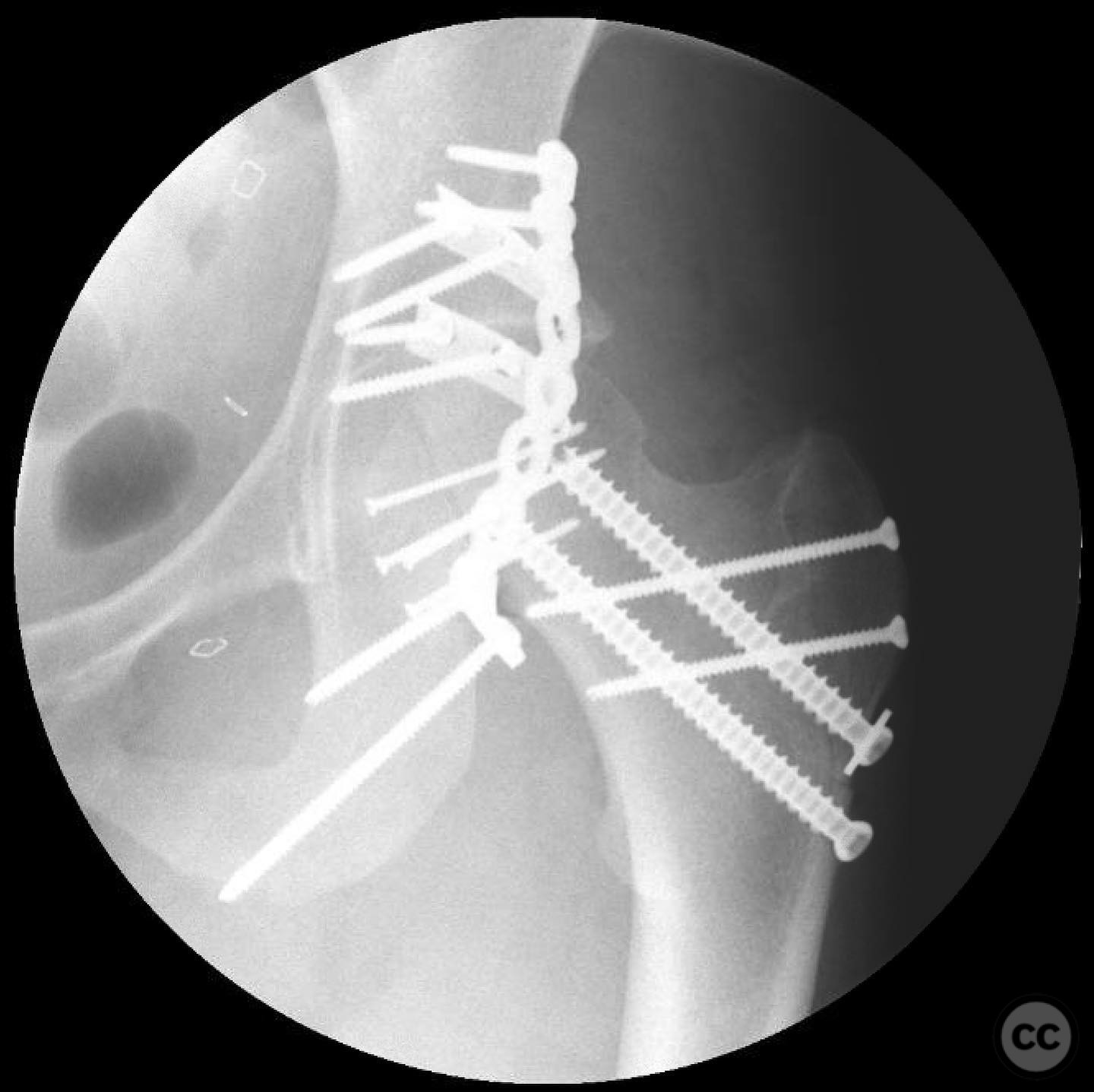
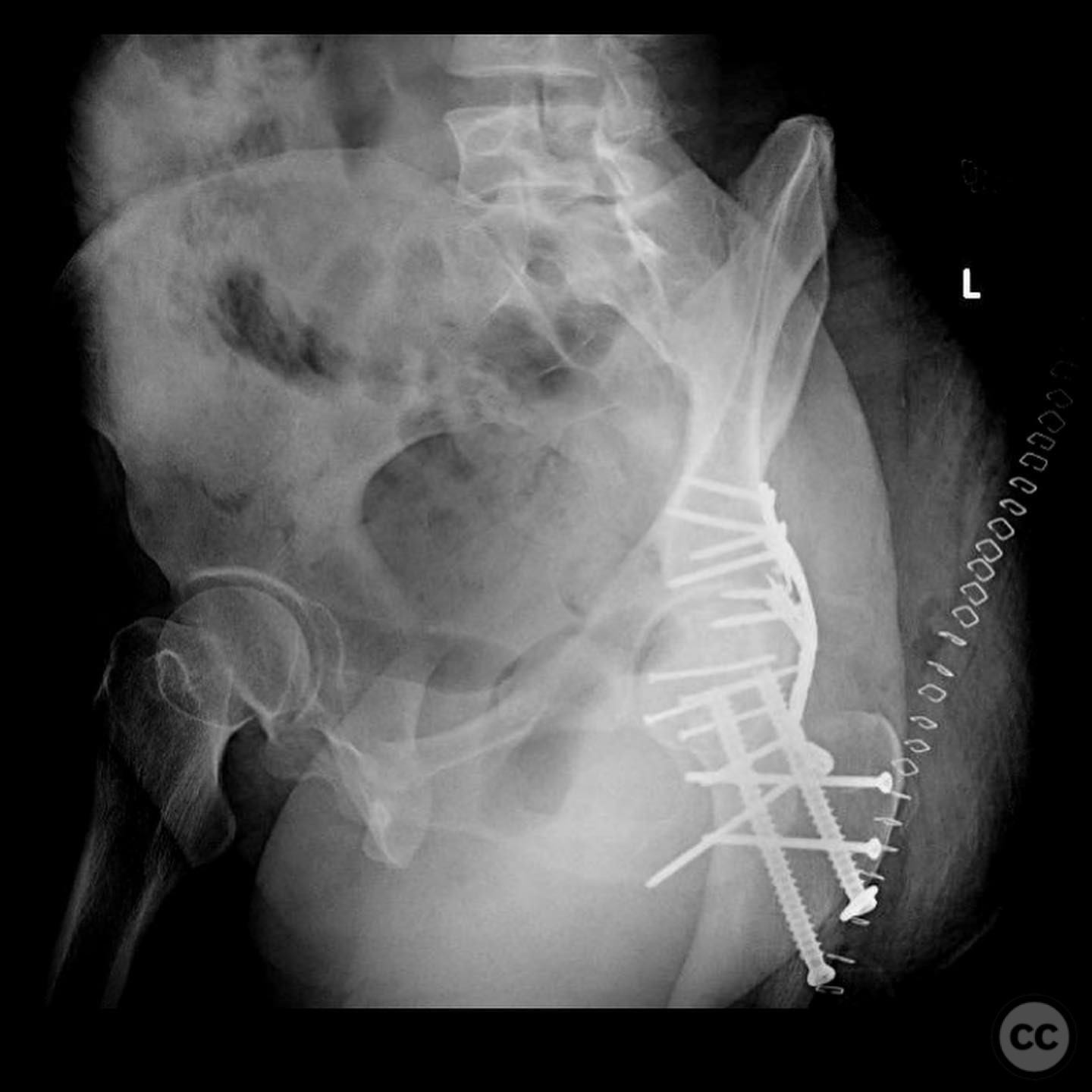
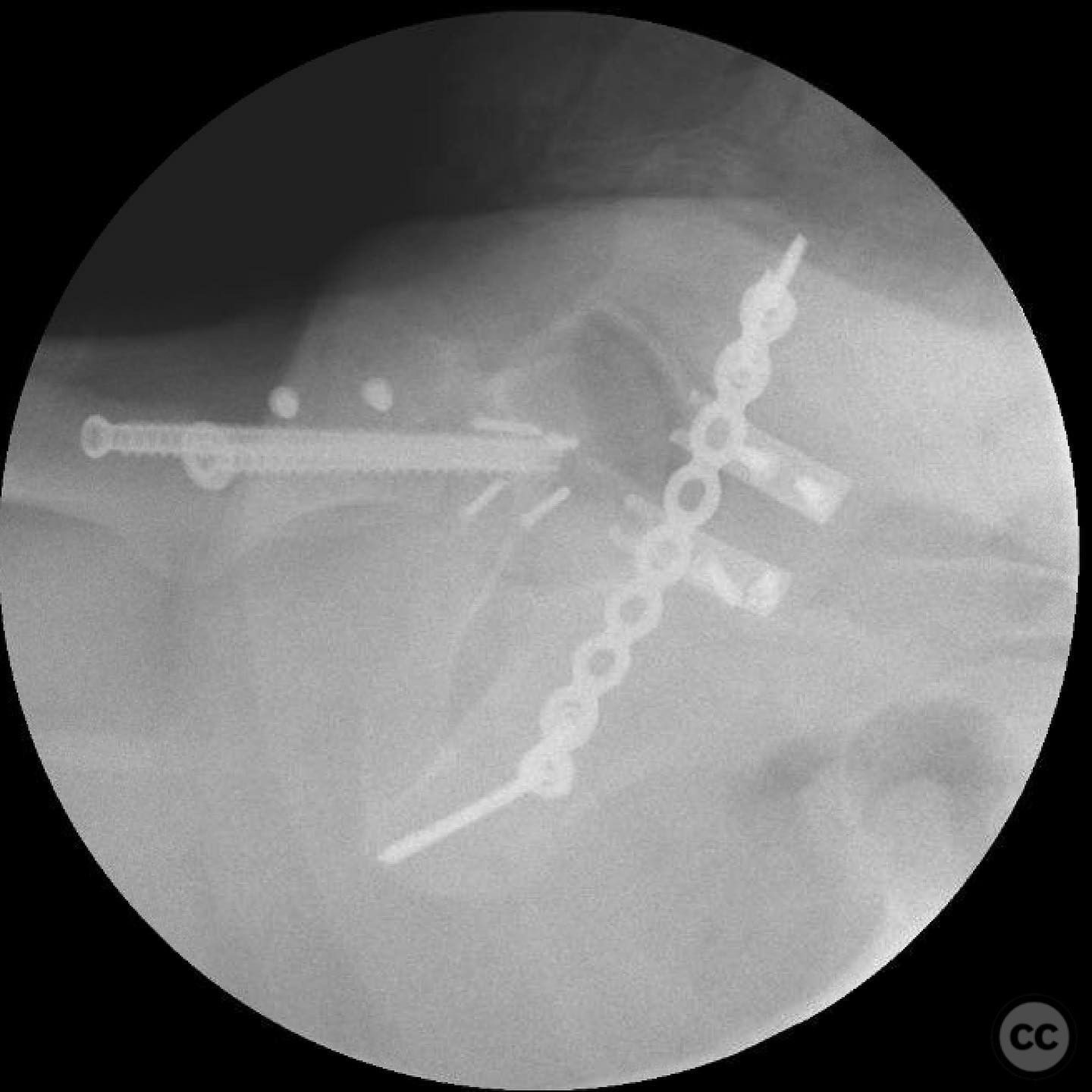
Operative remarks:The femoral head defect required meticulous reconstruction using a femoral head allograft to restore its round shape. The posterior wall instability was addressed with spring plates and three suture anchors to reattach the capsulolabral complex. The reconstruction aimed to achieve a stable and congruent hip joint.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing on the affected limb for 6 weeks, followed by gradual weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Femoral head allograft, spring plates, suture anchors.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 378 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Pipkin IV Femoral Head Fracture with Posterior Wall Involvement and Femoral Neck Fracture.. Journal of Orthopaedic Surgery and Traumatology. Case Report 29232632 Published Online Jul 14 2025.