



 who sustained a displaced comminuted subcapital femoral neck fracture when he _4.jpg)
 who sustained a displaced comminuted subcapital femoral neck fracture when he _1.jpg)
 who sustained a displaced comminuted subcapital femoral neck fracture when he _2.jpg)
 who sustained a displaced comminuted subcapital femoral neck fracture when he _6.jpg)
 who sustained a displaced comminuted subcapital femoral neck fracture when he _5.jpg)
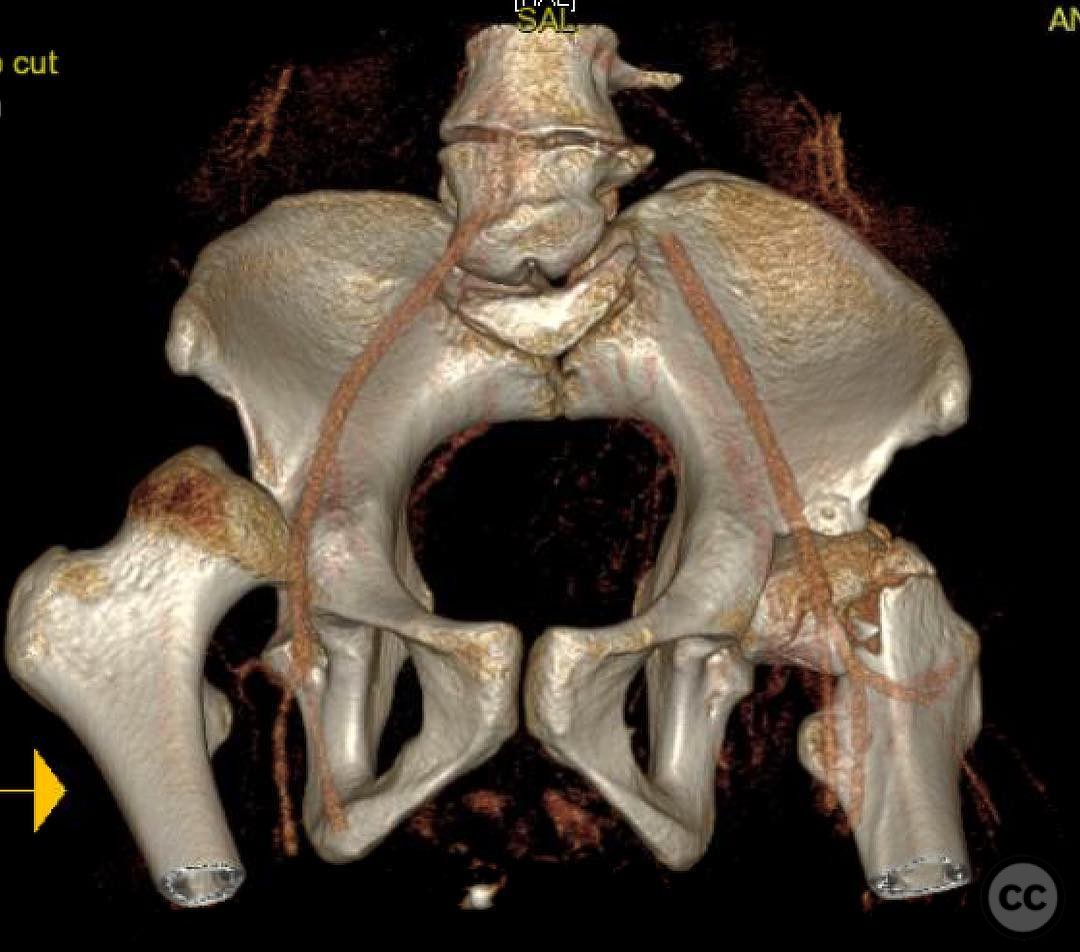
Displaced Comminuted Subcapital Femoral Neck Fracture in Caudal Regression Syndrome
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A young active male with caudal regression syndrome, characterized by sacral agenesis, sustained a displaced comminuted subcapital femoral neck fracture after being struck by a car while riding a scooter. Despite the absence of his sacrum and bilateral congenital hip dysplasia, he ambulates without hip pain. Radiological evaluation revealed a displaced comminuted subcapital fracture of the femoral neck. The patient has a urostomy and colostomy in proximity to the potential surgical site.
Preoperative Plan
Planning remarks: The preoperative plan involved closed reduction due to the presence of anterior neck comminution, which negated the benefits of an open approach, and the proximity of the urostomy and colostomy to the anterior incision site. The fixation strategy involved the use of cannulated screws for optimal fixation into the small subcapital segment.
Surgical Discussion
Patient positioning: Supine position on a fracture table to facilitate closed reduction and percutaneous screw fixation.
Anatomical surgical approach: Percutaneous approach for screw fixation was employed. Guidewires were inserted with precision to avoid multiple perforations of the lateral cortex, ensuring optimal placement of cannulated screws along the calcar and posterior neck.
Operative remarks:The surgeon emphasized the importance of precise guidewire placement to achieve optimal screw positioning without compromising the lateral cortex integrity. The use of screws was preferred over fixed-angle devices due to the very subcapital nature of the fracture, allowing for better fixation in the small segment. The disadvantages noted were the lack of fixed-angle stability and potential for uncontrolled fracture collapse.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with crutches for 6 weeks, followed by gradual progression to full weight-bearing as tolerated.
Follow up: Not specified.
Orthopaedic implants used: Cannulated screws.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 331 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Displaced Comminuted Subcapital Femoral Neck Fracture in Caudal Regression Syndrome. Journal of Orthopaedic Surgery and Traumatology. Case Report 21872741 Published Online Jul 21 2025.