









Pipkin IV Femoral Head Fracture with Femoral Shaft Fracture in a Polytrauma Patient.
Score and Comment on this Case
Clinical Details
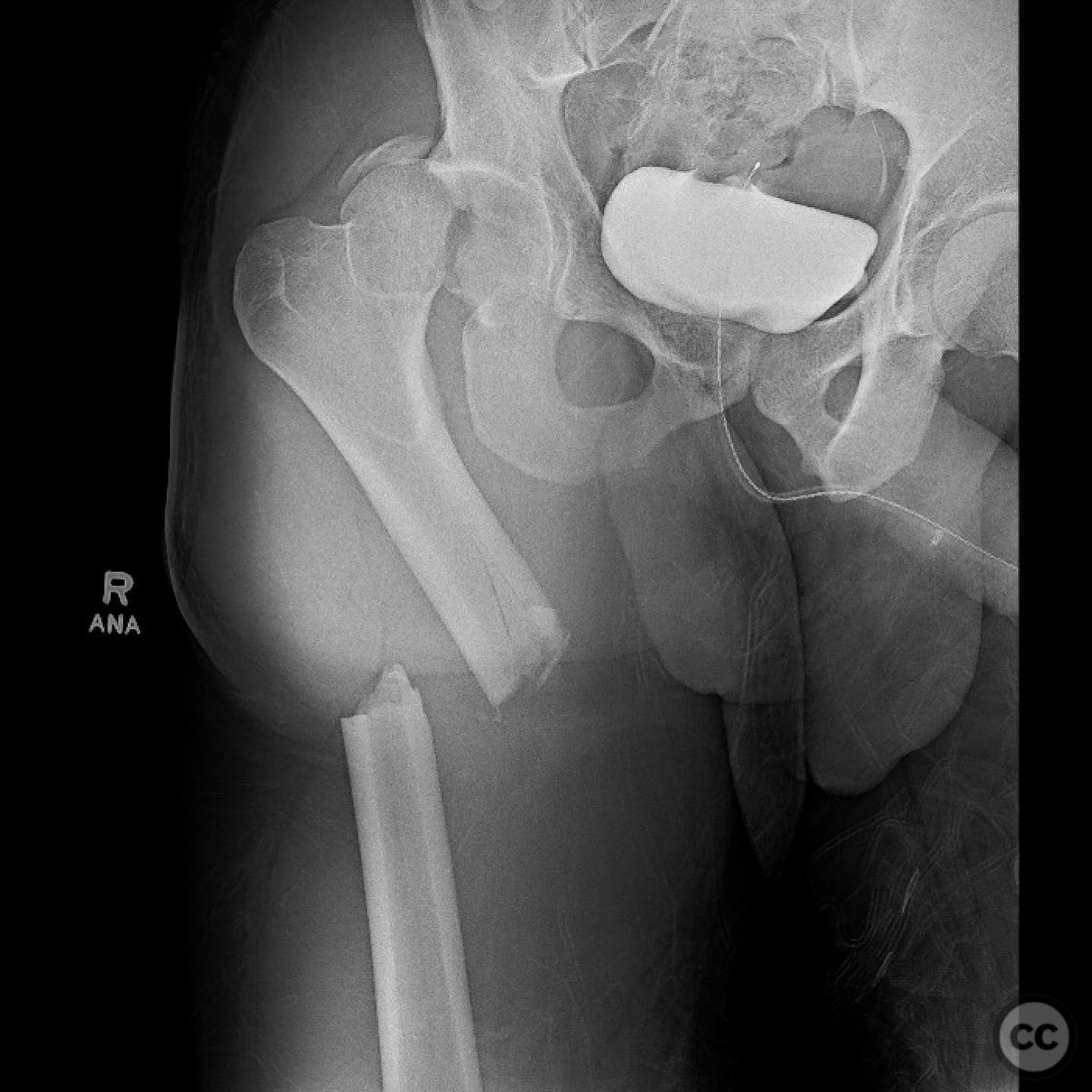
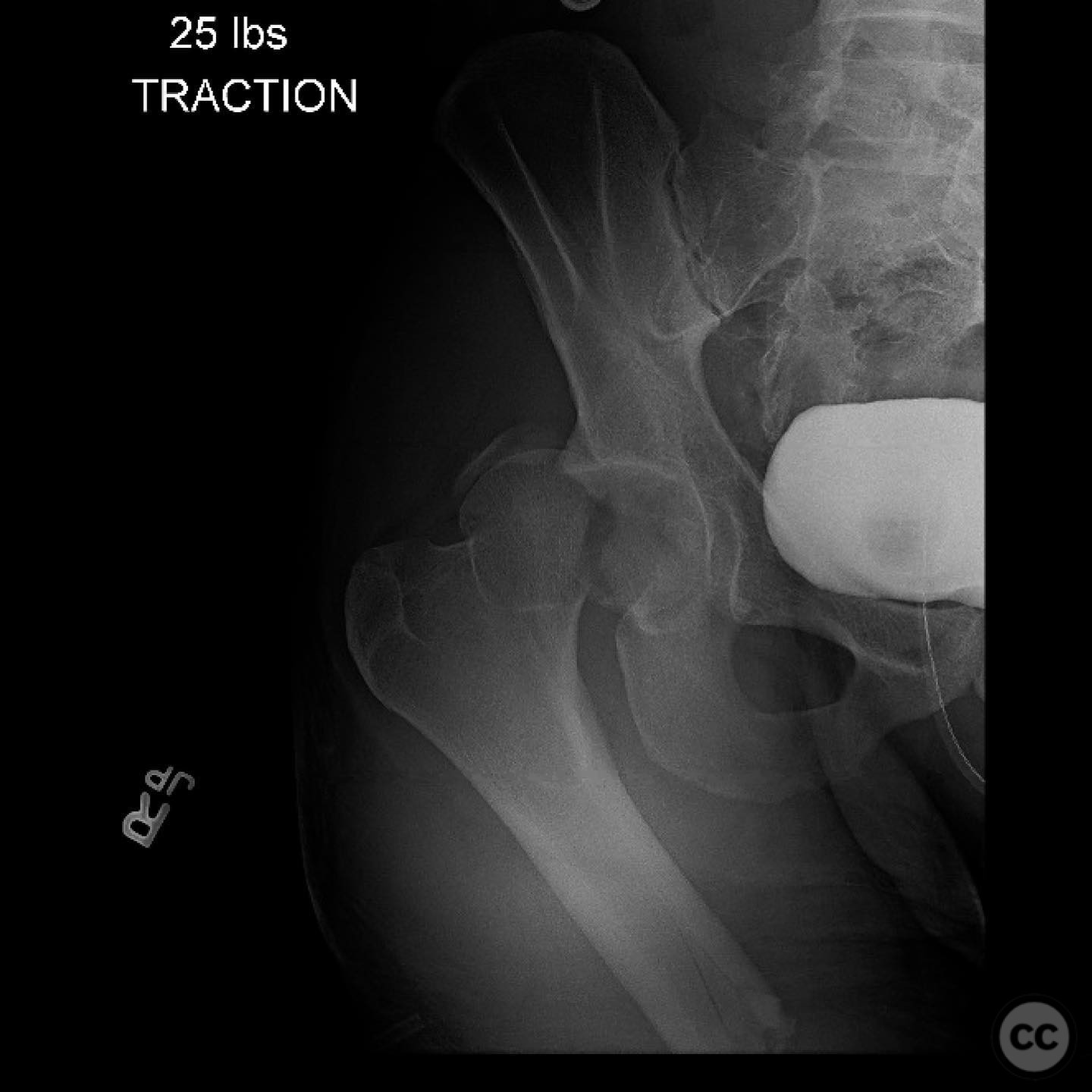
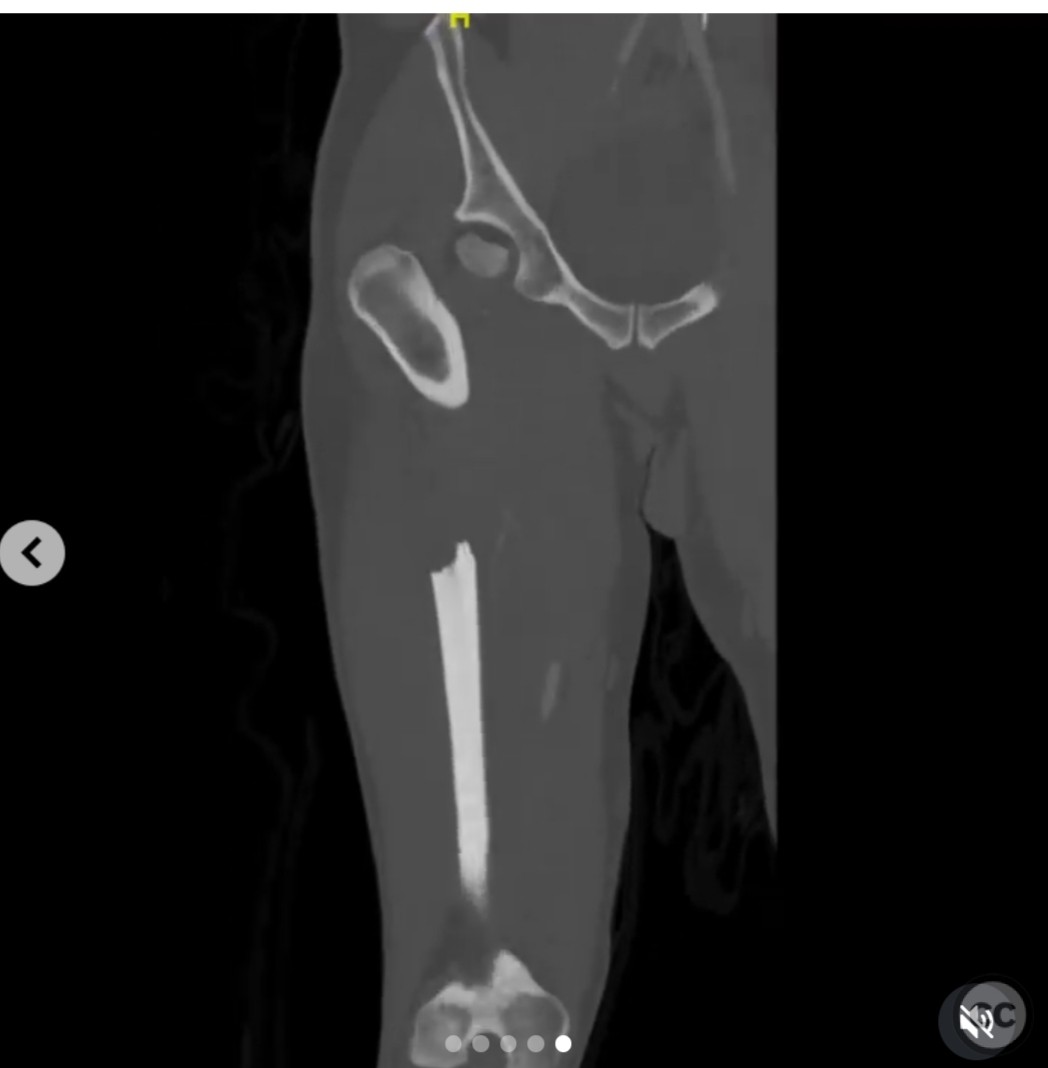
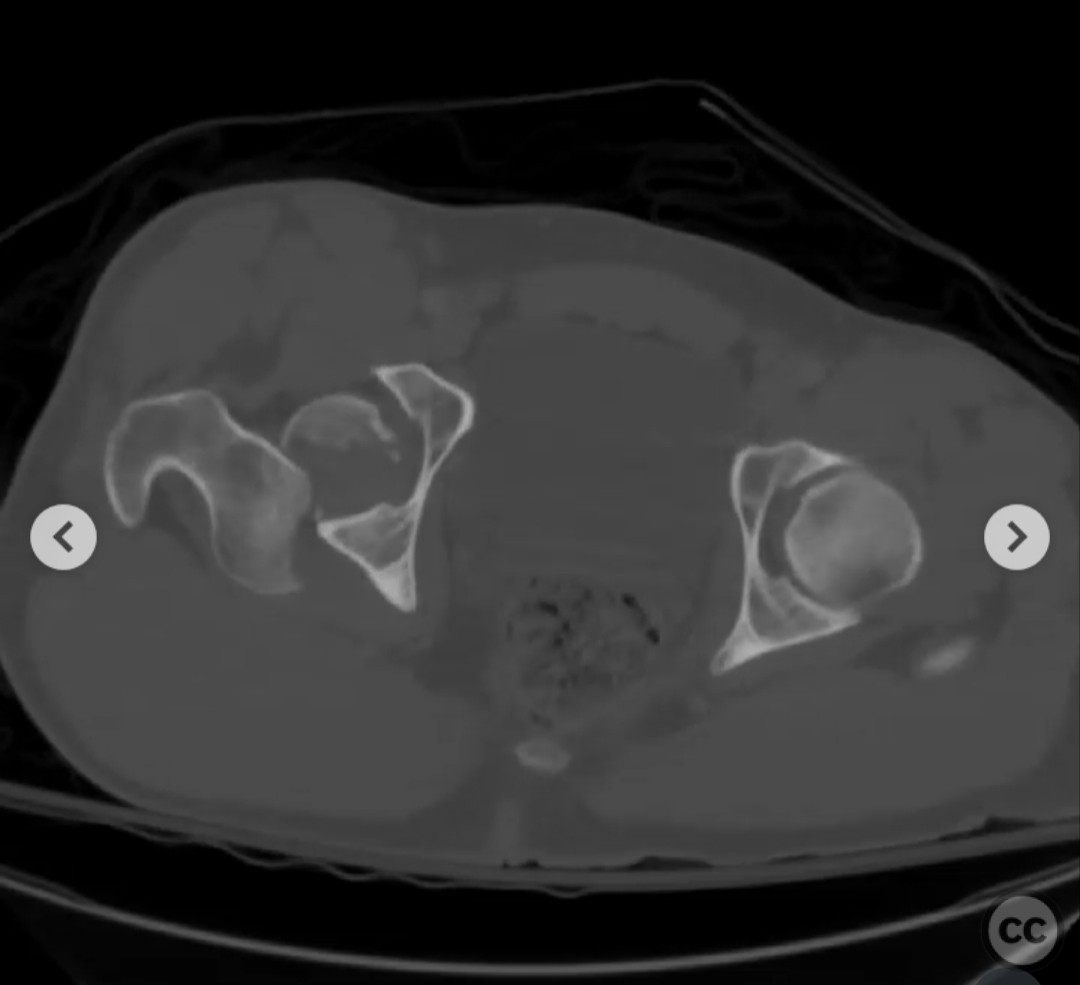
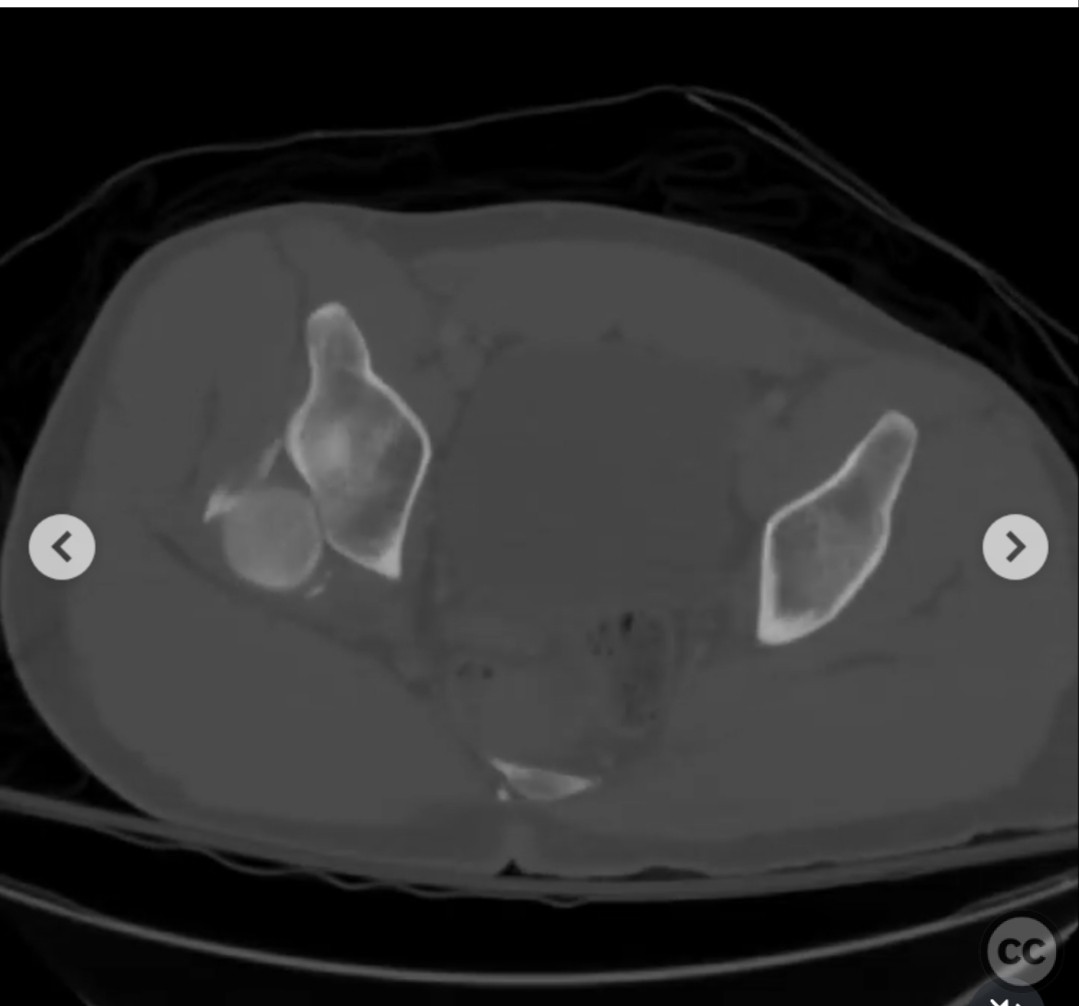
Clinical and radiological findings: A 32-year-old male sustained injuries in a high-speed motorcycle crash, resulting in a Pipkin IV femoral head fracture with an associated femoral shaft fracture. The patient was intubated at the scene due to hemodynamic instability, presenting with a hemopneumothorax, liver laceration, and hemoperitoneum. Initial vital signs included heart rate 90-100 bpm, blood pressure 99/65 mmHg, temperature 36.9°C, hematocrit 38%, platelet count 199 x 10^9/L, and lactate level 5.5 mmol/L. Radiological assessment confirmed the fracture pattern and the presence of a cranial acetabular wall fracture.
Preoperative Plan
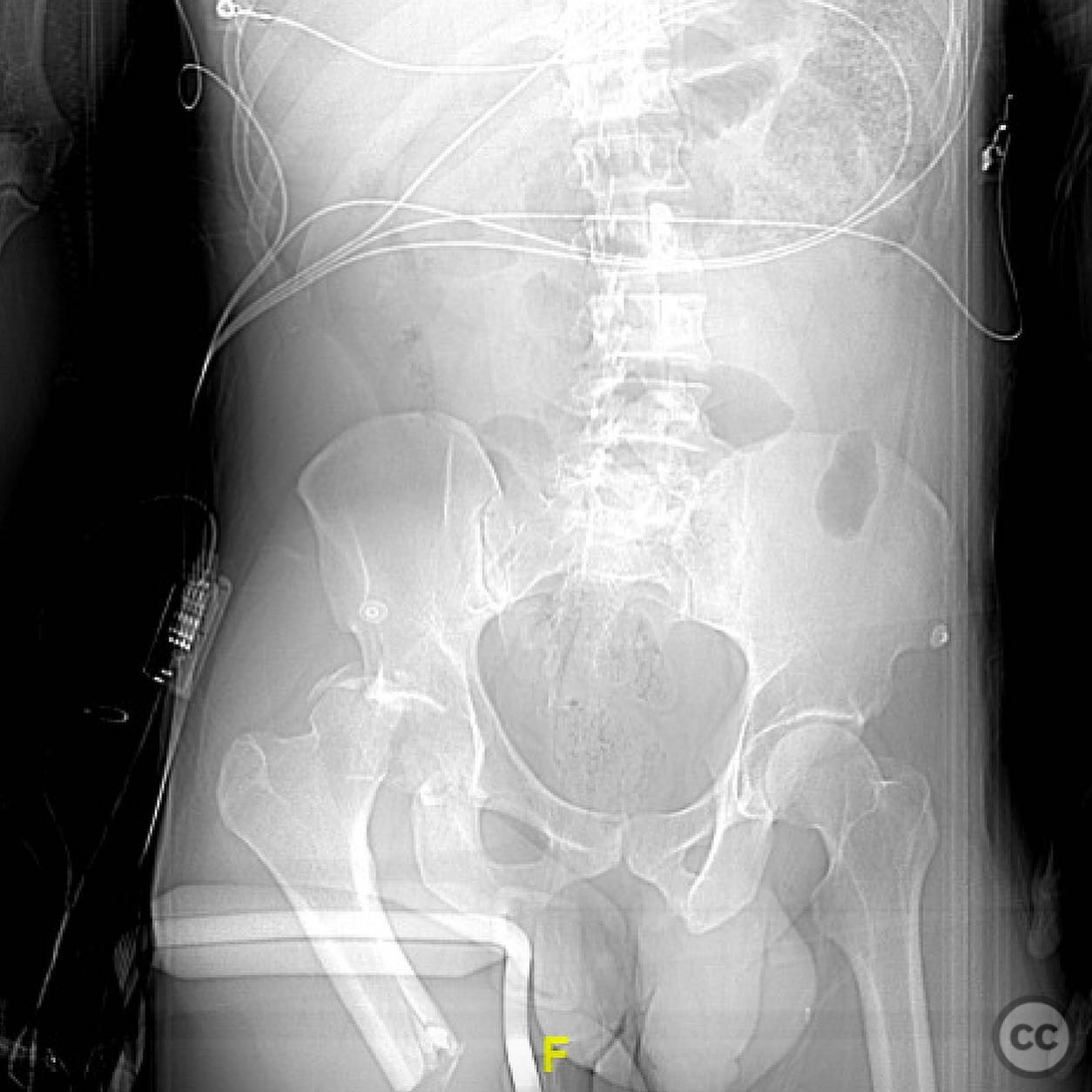
Planning remarks: The preoperative plan involved initial damage control orthopaedics with percutaneous reduction and external fixation of the femur. Definitive management was staged, prioritizing stabilization of the femoral shaft fracture before addressing the Pipkin IV fracture. The femoral shaft was planned to be stabilized first using an intramedullary nail, with consideration for either antegrade or retrograde nailing based on intraoperative findings and future surgical approach requirements.
Surgical Discussion
Patient positioning: The patient was positioned supine for the initial damage control procedure. For definitive fixation of the femoral shaft, the patient remained supine to facilitate intramedullary nailing.
Anatomical surgical approach: A lateral approach to the femur was utilized for intramedullary nailing. For the subsequent management of the Pipkin IV fracture, a Gibson approach was planned, involving a trochanteric osteotomy and surgical hip dislocation to address the femoral head fracture. The patient was repositioned to a lateral decubitus position for this stage.
Operative remarks:The surgical team emphasized the importance of stabilizing the femoral shaft prior to addressing the acetabular and femoral head fractures to prevent intraoperative complications such as hip dislocation. The decision to use a Gibson approach with trochanteric osteotomy allowed for optimal exposure and management of both the femoral head and acetabular wall fractures. The cranial location of the acetabular wall fracture necessitated fixation due to its contribution to hip instability.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing on the affected limb for six weeks, followed by gradual weight-bearing as tolerated. Range of motion exercises were initiated early to prevent joint stiffness, with progression to strengthening exercises as healing permitted.
Follow up: Not specified.
Orthopaedic implants used: External fixator, intramedullary nail, trochanteric osteotomy hardware, screws for ORIF of femoral head and acetabular wall.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 302 times
13 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Pipkin IV Femoral Head Fracture with Femoral Shaft Fracture in a Polytrauma Patient.. Journal of Orthopaedic Surgery and Traumatology. Case Report 20192084 Published Online Jul 13 2025.