





Pipkin Type III Femoral Head and Neck Fracture Dislocation in a Young Adult
Score and Comment on this Case
Clinical Details
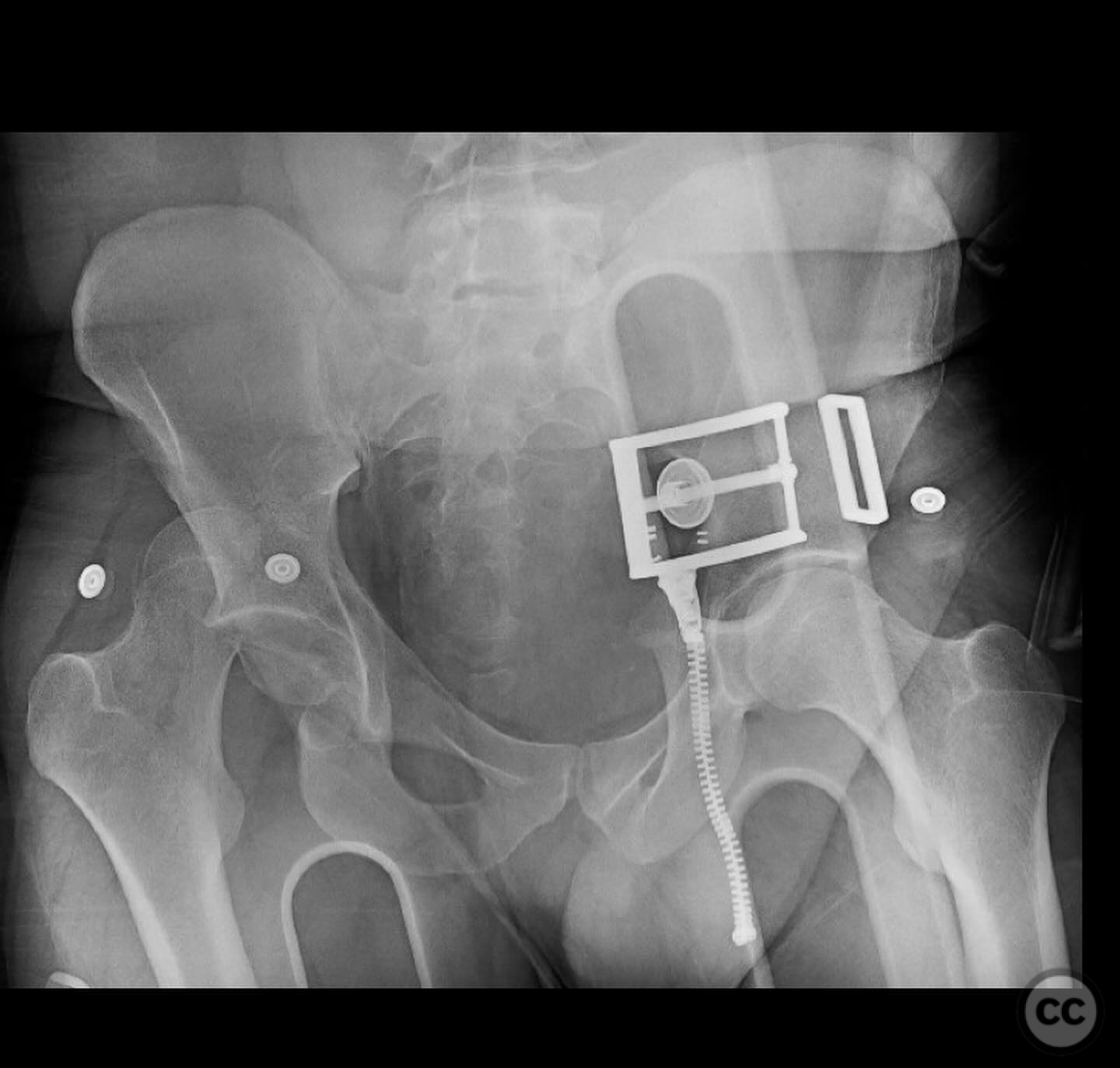
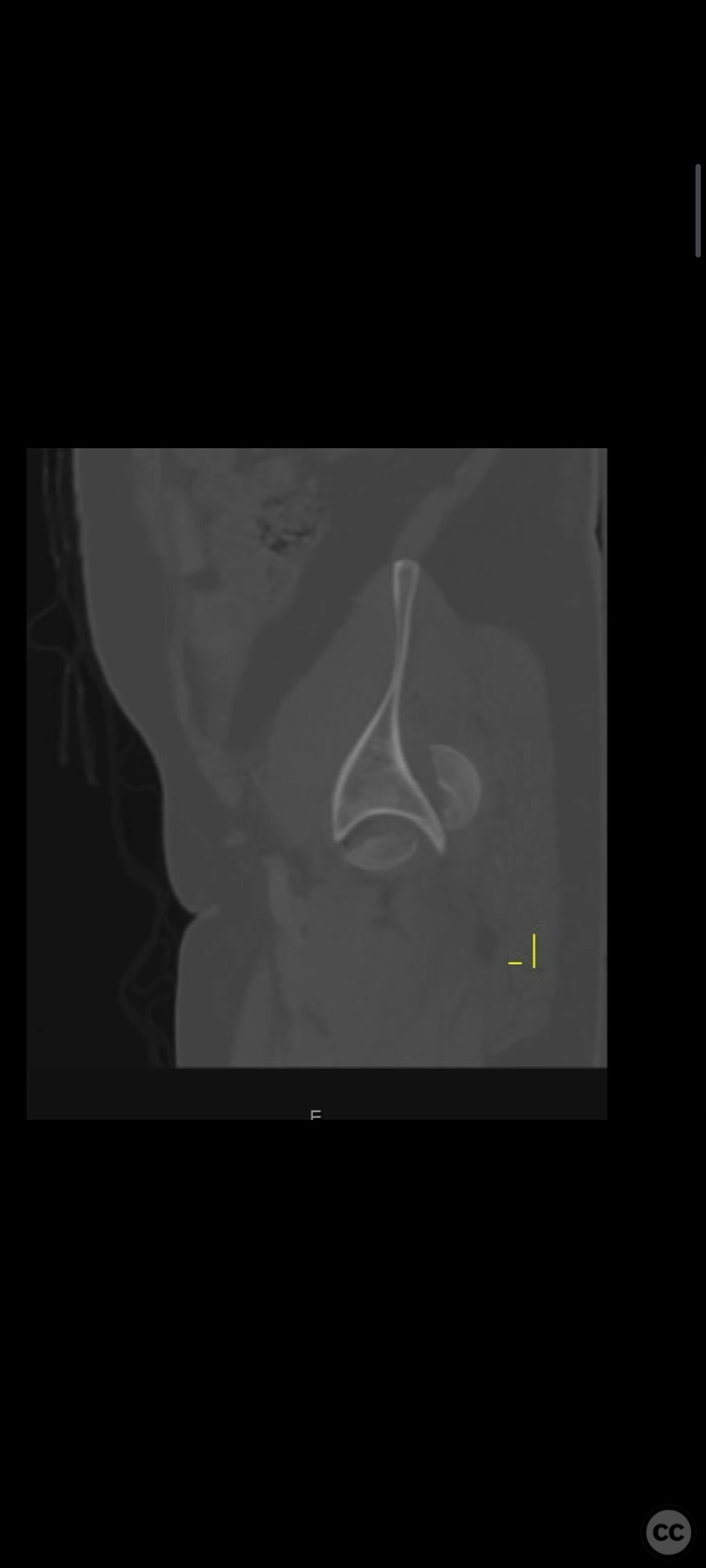
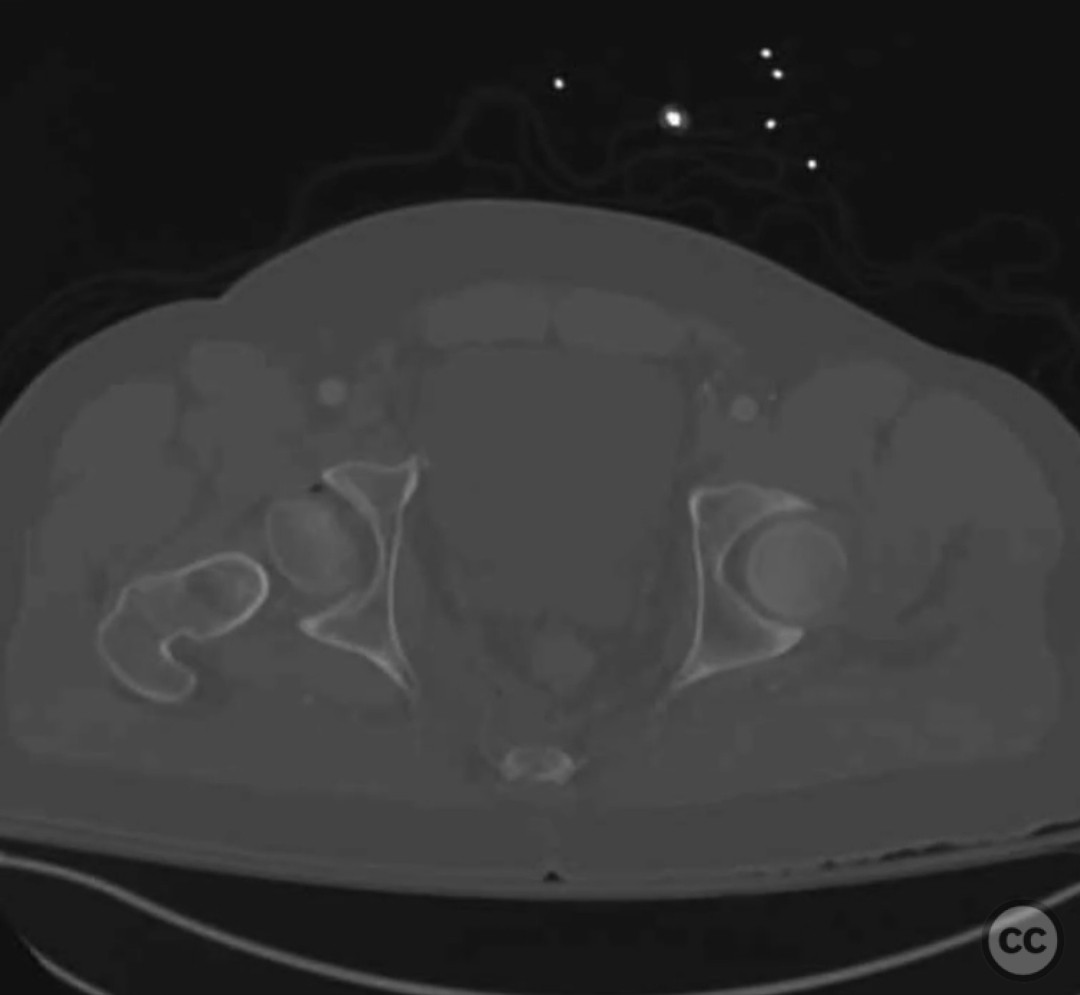
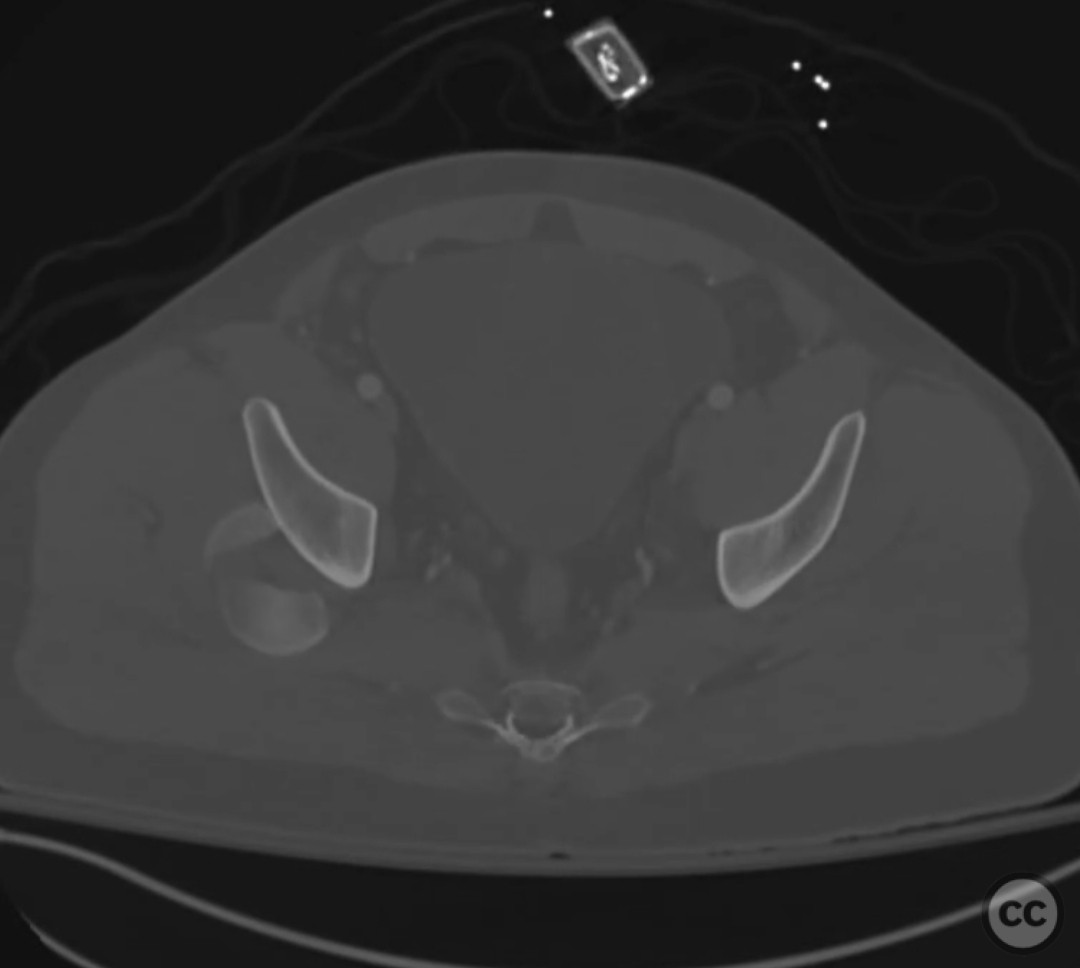
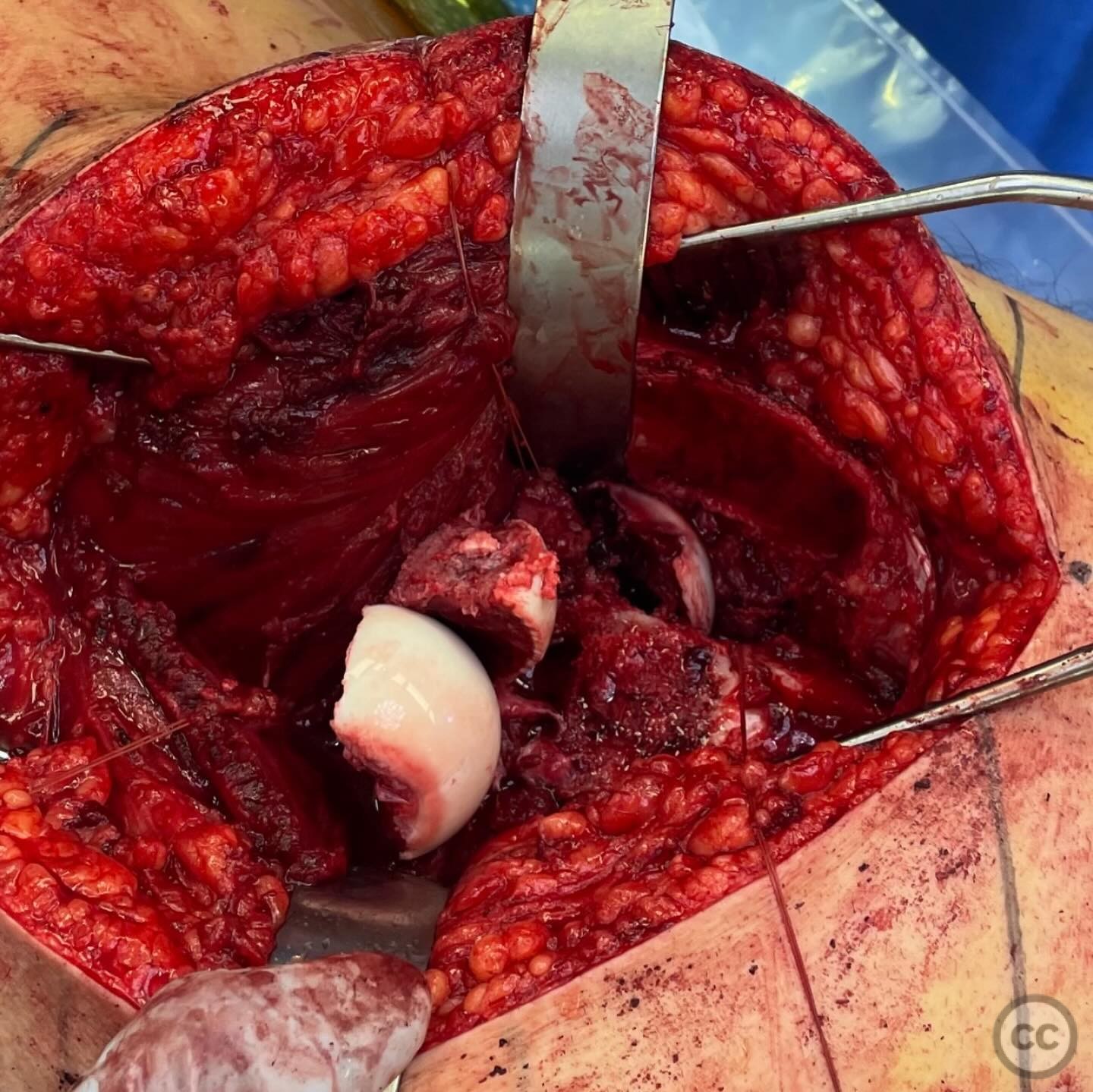
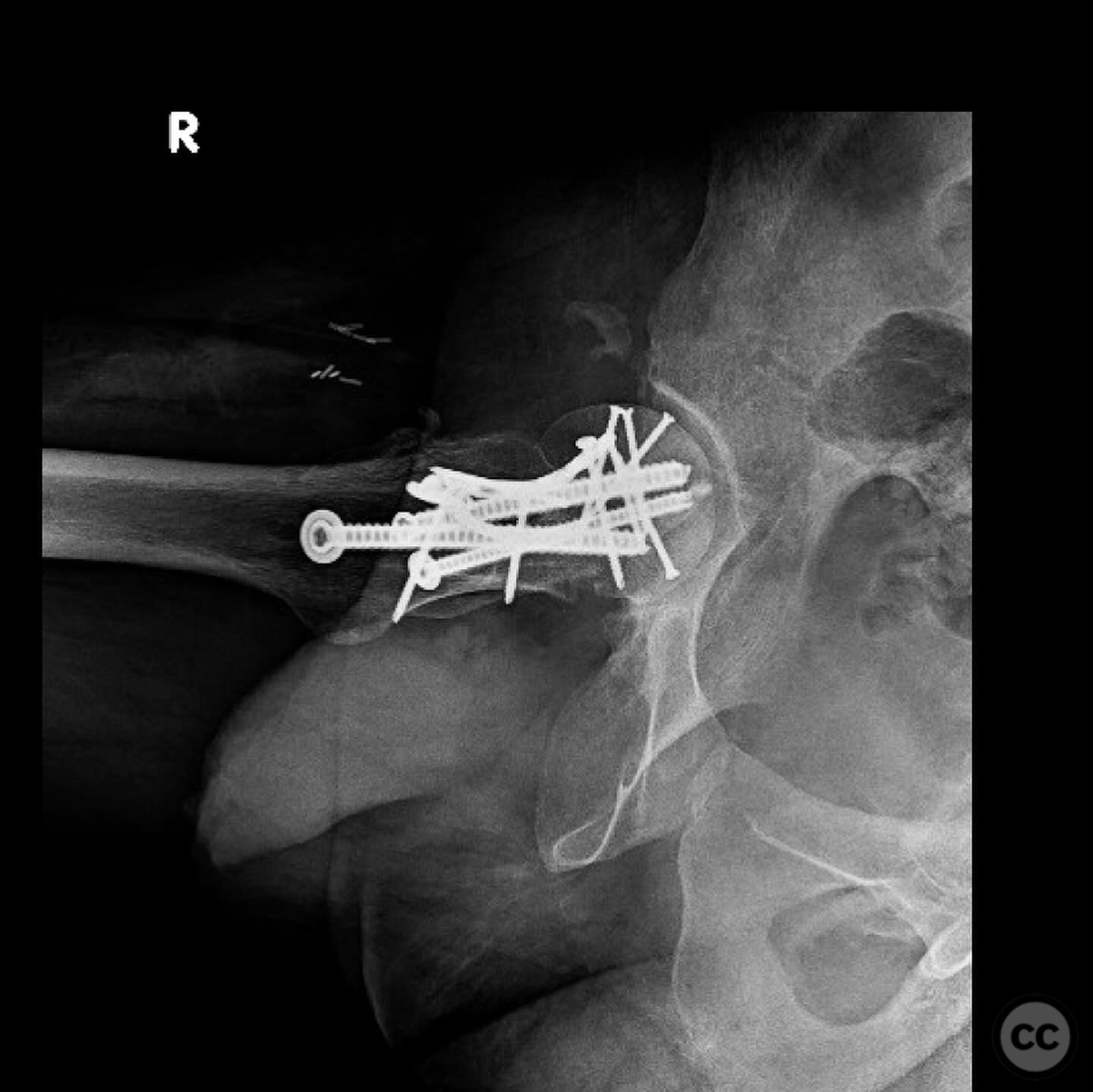
Clinical and radiological findings: A 19-year-old male involved in a motorcycle accident presented with a Pipkin Type III femoral head and neck fracture dislocation. The patient had other extremity injuries but was not in extremis. Radiological evaluation confirmed the complex fracture dislocation, with the femoral head in three pieces, one of which retained significant retinacular tissue.
Preoperative Plan
Planning remarks: The preoperative plan involved a Gibson approach with a surgical hip dislocation to facilitate reduction and fixation. The primary goal was to preserve the patient's native hip joint due to his young age, despite the high risk of complications such as avascular necrosis (AVN) and post-traumatic osteoarthritis (PTOA).
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position to allow optimal access for the Gibson approach and surgical hip dislocation.
Anatomical surgical approach: A Gibson approach was utilized, involving an incision along the posterior aspect of the hip, extending from the posterior superior iliac spine to the greater trochanter. The gluteus maximus was split, and the short external rotators were released to expose the hip joint. A surgical dislocation of the hip was performed to facilitate direct visualization and manipulation of the fracture fragments.
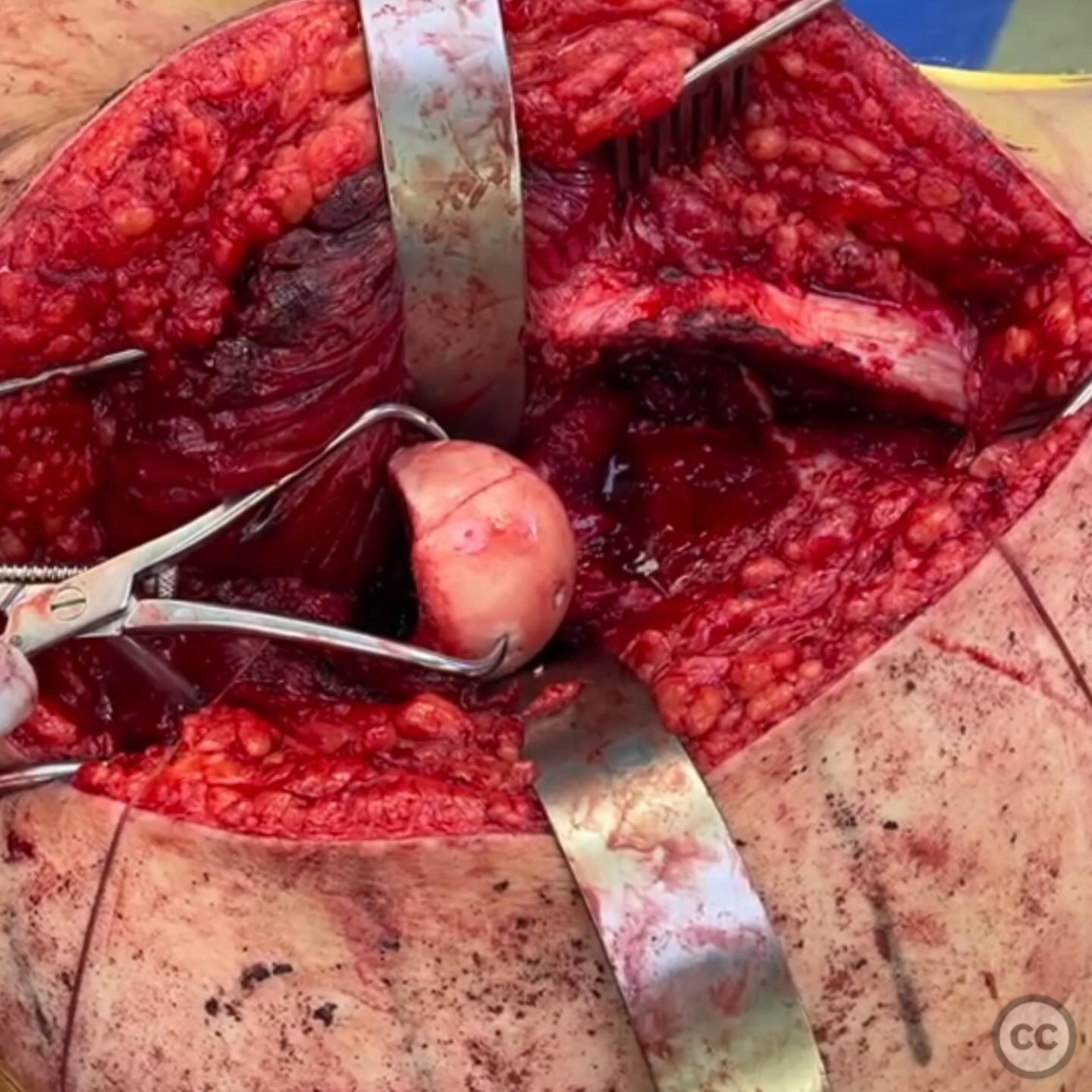
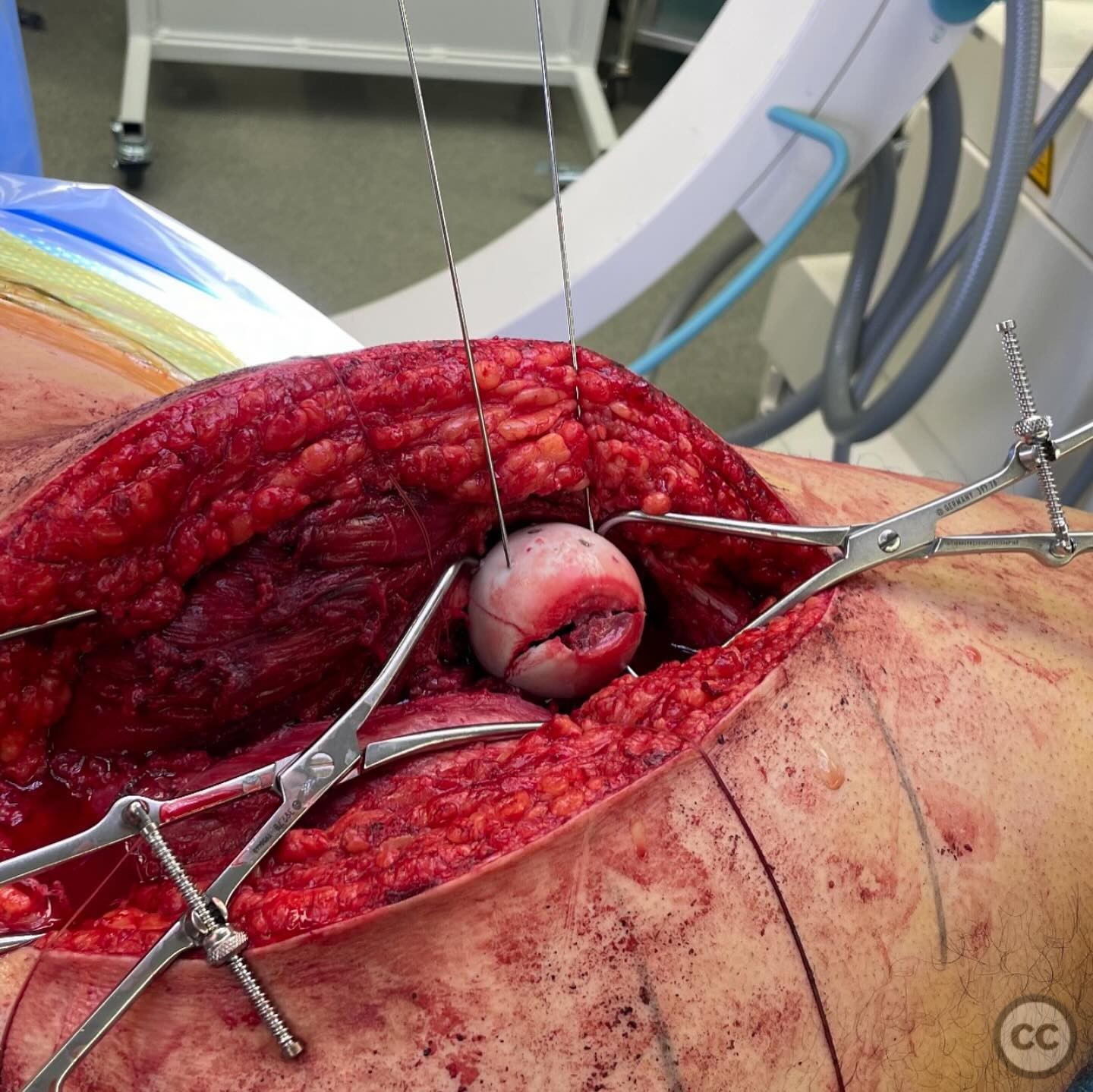
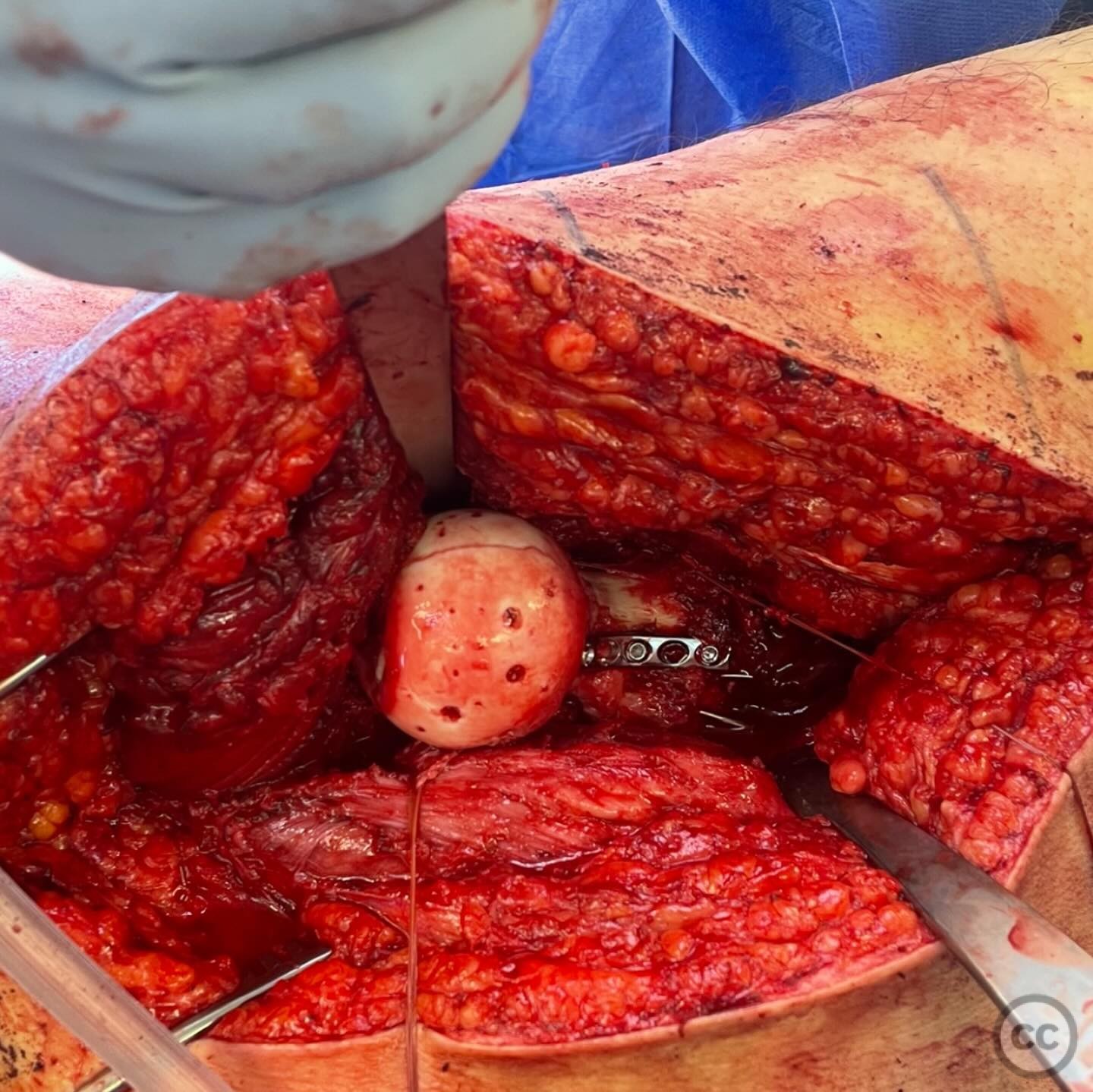
Operative remarks:The reduction of the femoral head was straightforward; however, achieving reduction of the head to the neck was challenging due to the need to preserve retinacular tissues. Antegrade wire fixation was employed initially to stabilize the head fragments, allowing for subsequent reduction of the hip joint without displacing the neck fracture. Definitive fixation involved navigating a "traffic jam" of hardware, utilizing 5.5 mm cannulated screws past 2.4 mm screws in the head.
Postoperative protocol: Postoperatively, the patient was allowed partial weight-bearing with crutches for six weeks, progressing to full weight-bearing as tolerated. Regular follow-up was scheduled to monitor for signs of AVN or other complications.
Follow up: At six months post-surgery, the patient was ambulatory but experienced pain due to prominent lateral screws and a migrated wire. Revision surgery was performed to replace screws with shorter 7.0 mm screws and retrieve the wire through an anterior approach. The patient remained ambulatory without hip pain at this stage, though vigilant monitoring for AVN continues.
Orthopaedic implants used: 5.5 mm cannulated screws, 2.4 mm screws, 7.0 mm screws, antegrade wires.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 343 times
10 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Pipkin Type III Femoral Head and Neck Fracture Dislocation in a Young Adult. Journal of Orthopaedic Surgery and Traumatology. Case Report 13879591 Published Online Jul 10 2025.