






Monteggia Fracture with Segmental Ulna Shaft Fracture
Score and Comment on this Case
Clinical Details
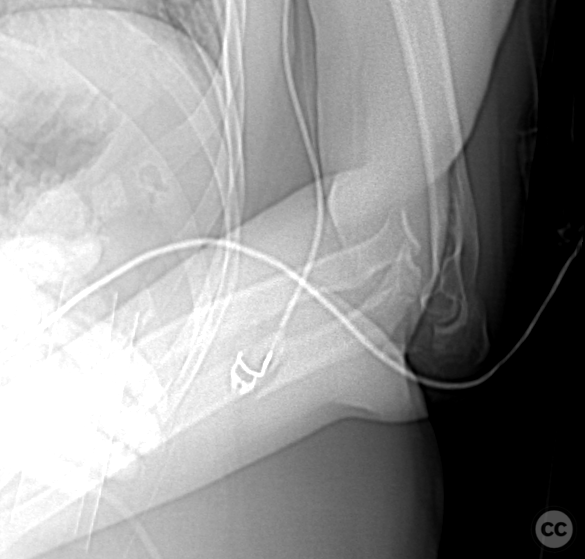
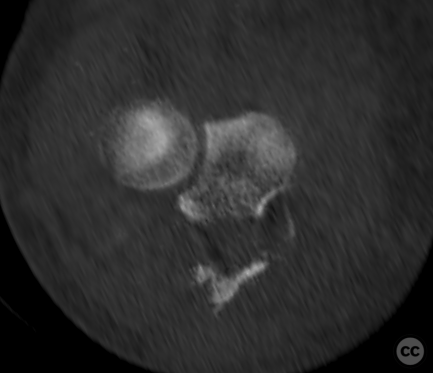
Clinical and radiological findings: A 35-year-old female involved in a motor vehicle accident presented as a polytrauma patient with multiple injuries, including a Monteggia fracture (AO/OTA classification 2U1B3) with a segmental ulna shaft fracture (AO/OTA classification 2U2C3). The injury was closed. Initial management included reduction and immobilization in an external fixator as part of a damage control strategy. Radiographs confirmed the fracture pattern, and CT imaging provided detailed visualization of the fracture fragments.
Preoperative Plan
Planning remarks: The definitive surgical plan involved removal of the external fixator, thorough debridement of pin sites, and internal fixation of the ulna shaft and Monteggia fracture. The planned approach was a dorsal incision along the forearm, curving around the radial aspect of the olecranon to expose the ulna and facilitate reduction and fixation.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table. The left arm was initially placed at the side for removal of the external fixator, followed by repositioning over the patient's chest on an auxiliary arm holder anteriorly, allowing acces
Anatomical surgical approach: A longitudinal dorsal incision was made along the forearm, curving around the radial aspect of the olecranon. Subcutaneous dissection was performed between the flexor carpi ulnaris and extensor carpi ulnaris muscles to expose the dorsal aspect of the ulna. The anconeus muscle was reflected to expose the proximal radial aspect of the ulna. A limited Taylor sham approach was employed to access the medial aspect, reflecting one belly of the flexor carpi ulnaris. An incision on the radial aspect of the capsule allowed visualization of the ulnar humeral joint and radial capitellar joint. The fragmented olecranon was left attached to muscular attachments, focusing on reconstructing major articular fragments and triceps insertion.
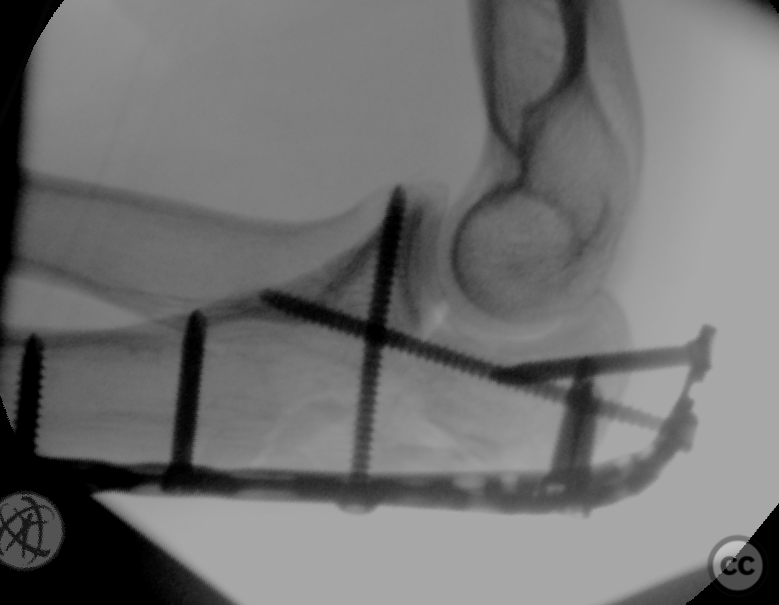
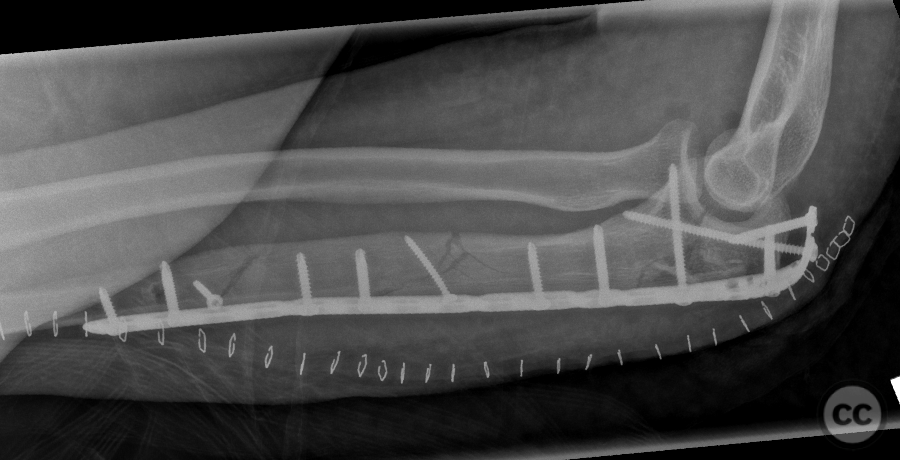
Operative remarks:Dynamic testing demonstrated a congruent reduction with minimal instability. The anterior dislocation of the proximal radial ulnar joint could not be reproduced, and no rupture of the ligamentum annulare could be identified. Segmental fragments distal to the main injury zone were anatomically reduced and secured with two 2.7-mm bicortical lag screws. A 3.5-mm olecranon plate was positioned and fixed with a single bicortical screw for initial adjustment, followed by a crucial screw engaging the coronoid to secure the ulnar humeral articulation. Additional screws engaged triceps insertion and intermediate articular fragments, ensuring stability. Multiplanar fluoroscopy and dynamic assessment confirmed no residual instability, negating further exploration of ligament structures.
Postoperative protocol: Postoperatively, no splinting is anticipated. A full range of non-weight-bearing motion is encouraged immediately.
Follow up: Not specified
Orthopaedic implants used: Orthopaedic implants used: - 2 x 2.7-mm bicortical lag screws - 3.5-mm olecranon plate
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Guest User
Excellent work. i would choose little longer plate to have at least three screws distal to the fracture extent
Could get one :( and didn’t want to bulk it up with overlapping plates. Begrudgingly accepted 2 screws and the interfrag.
Couldn’t