







Open Diaphyseal Clavicle Fracture with Butterfly Fragments
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 35-year-old male presented with an open diaphyseal clavicle fracture following a high-energy motorcycle accident. The fracture was classified as a simple diaphyseal pattern with two butterfly fragments, according to the AO/OTA classification system, specifically 15-B2. The patient exhibited significant soft tissue injury but no neurovascular compromise. Initial radiographs confirmed the fracture pattern, and the wound was thoroughly irrigated and debrided in the emergency department.
Preoperative Plan
Planning remarks: The preoperative plan involved direct exposure of the fracture site with anatomic clamp reduction. Interfragmentary compression was planned using lag screws for the butterfly fragments, followed by application of a reconstruction plate on the anterior inferior aspect of the clavicle for neutralization.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with a small sandbag placed between the scapulae to elevate the shoulder girdle, facilitating access to the clavicle.
Anatomical surgical approach: A direct approach to the clavicle was utilized, involving a longitudinal incision overlying the fracture site. Subcutaneous tissues were carefully dissected, and the platysma muscle was incised in line with its fibers. The fracture site was exposed by elevating the periosteum and preserving soft tissue attachments as much as possible.
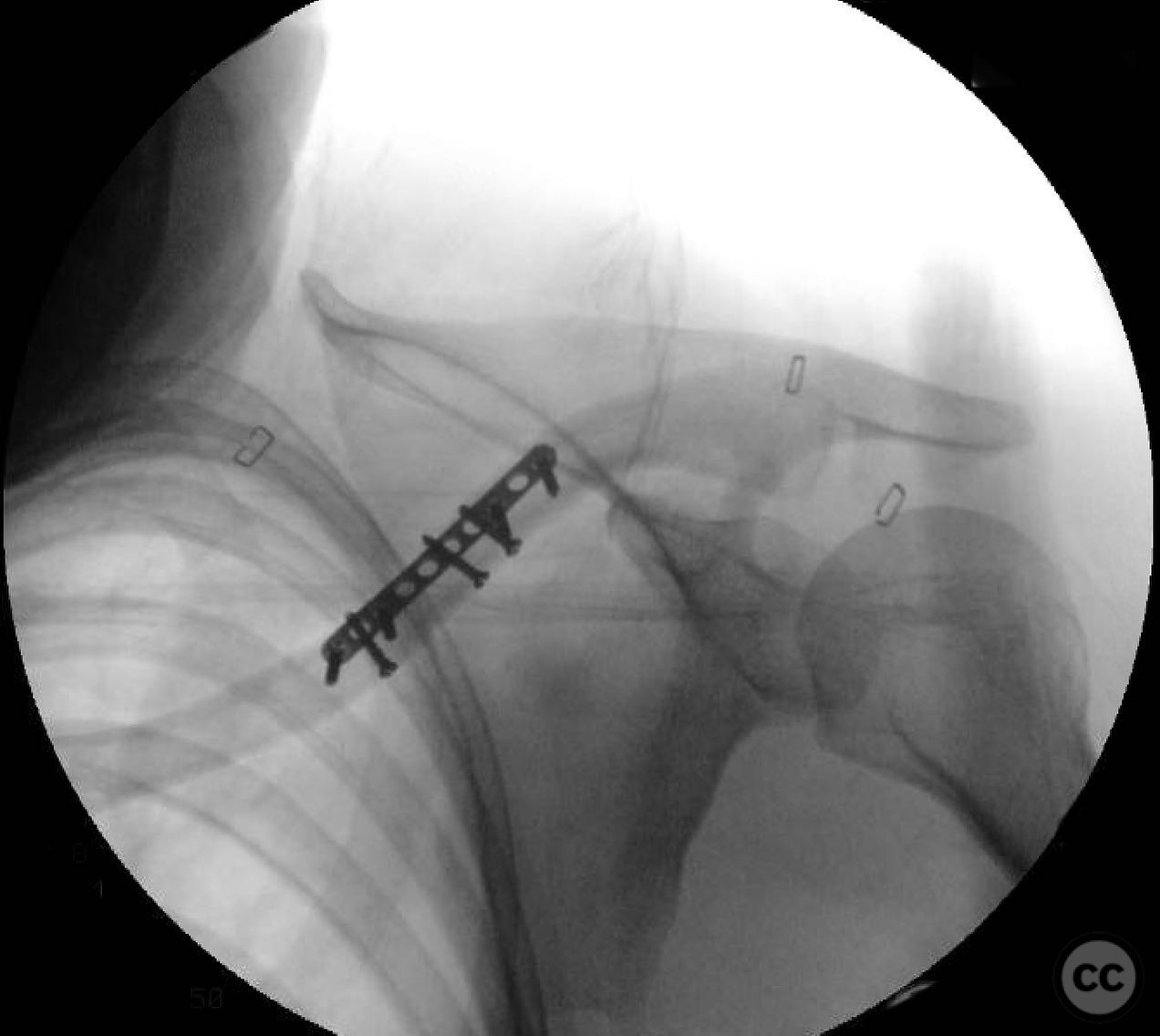
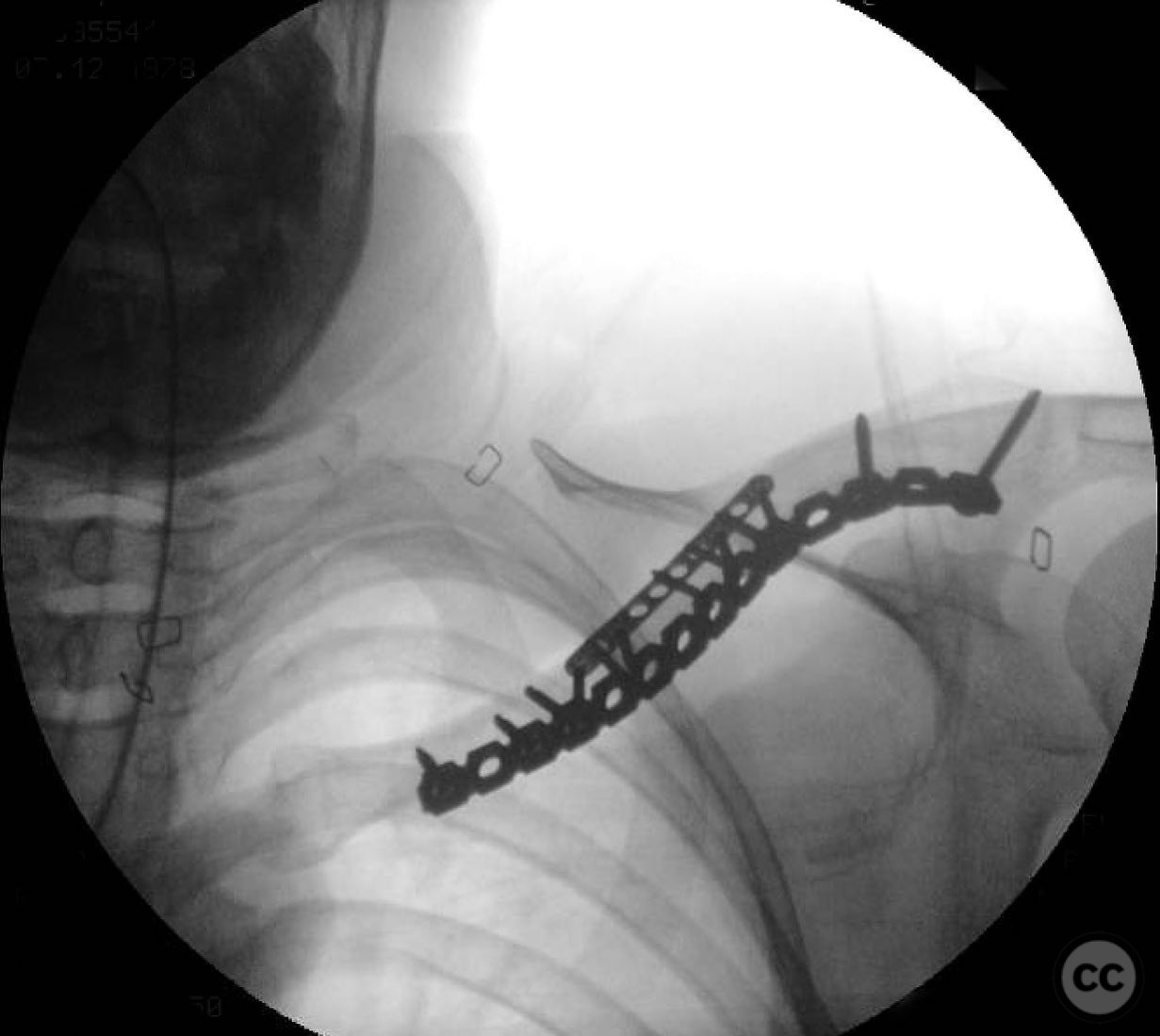
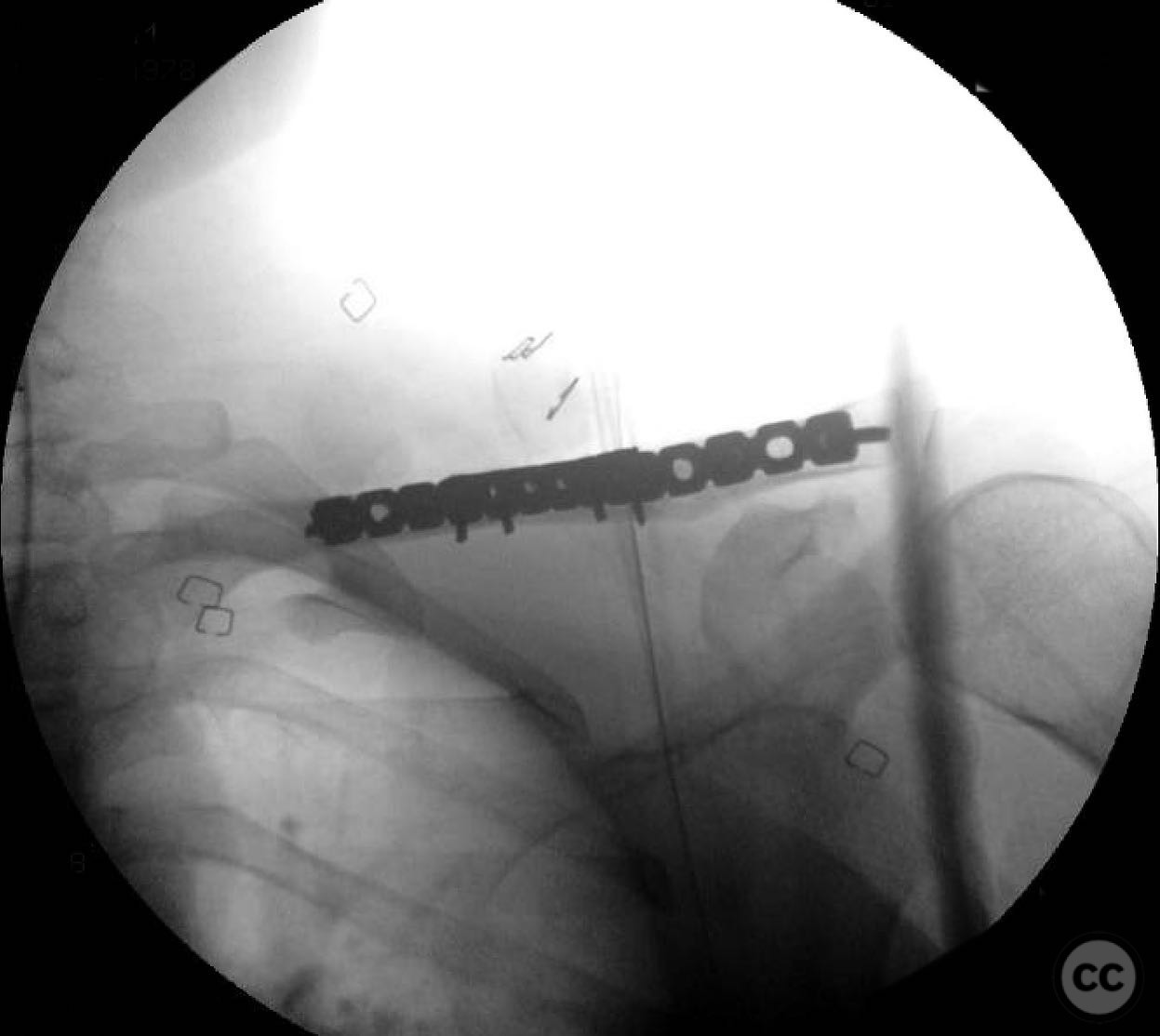
Operative remarks:During the procedure, anatomic reduction of the butterfly fragments was achieved using 2.4mm lag screws for interfragmentary compression. The main segment reduction proved challenging due to instability; hence, a 2.4mm "clamp replacement plate" was temporarily used to maintain reduction. A reconstruction plate was contoured and applied to the anterior inferior clavicle, providing a neutralization construct. Absolute stability was achieved, anticipating primary bone healing.
Postoperative protocol: Postoperatively, the patient was instructed to wear a sling for comfort and protection. Passive range of motion exercises for the shoulder were initiated at two weeks post-surgery, progressing to active-assisted exercises by four weeks. Full active range of motion and strengthening exercises were commenced at six weeks postoperatively.
Follow up: Not specified.
Orthopaedic implants used: 2.4mm lag screws, 2.4mm clamp replacement plate, reconstruction plate.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 331 times
16 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Open Diaphyseal Clavicle Fracture with Butterfly Fragments. Journal of Orthopaedic Surgery and Traumatology. Case Report 8732155 Published Online Jul 16 2025.