
Operative Stabilization of Displaced Comminuted Iliac Fracture with Lag Screws and Plate
Score and Comment on this Case
Clinical Details
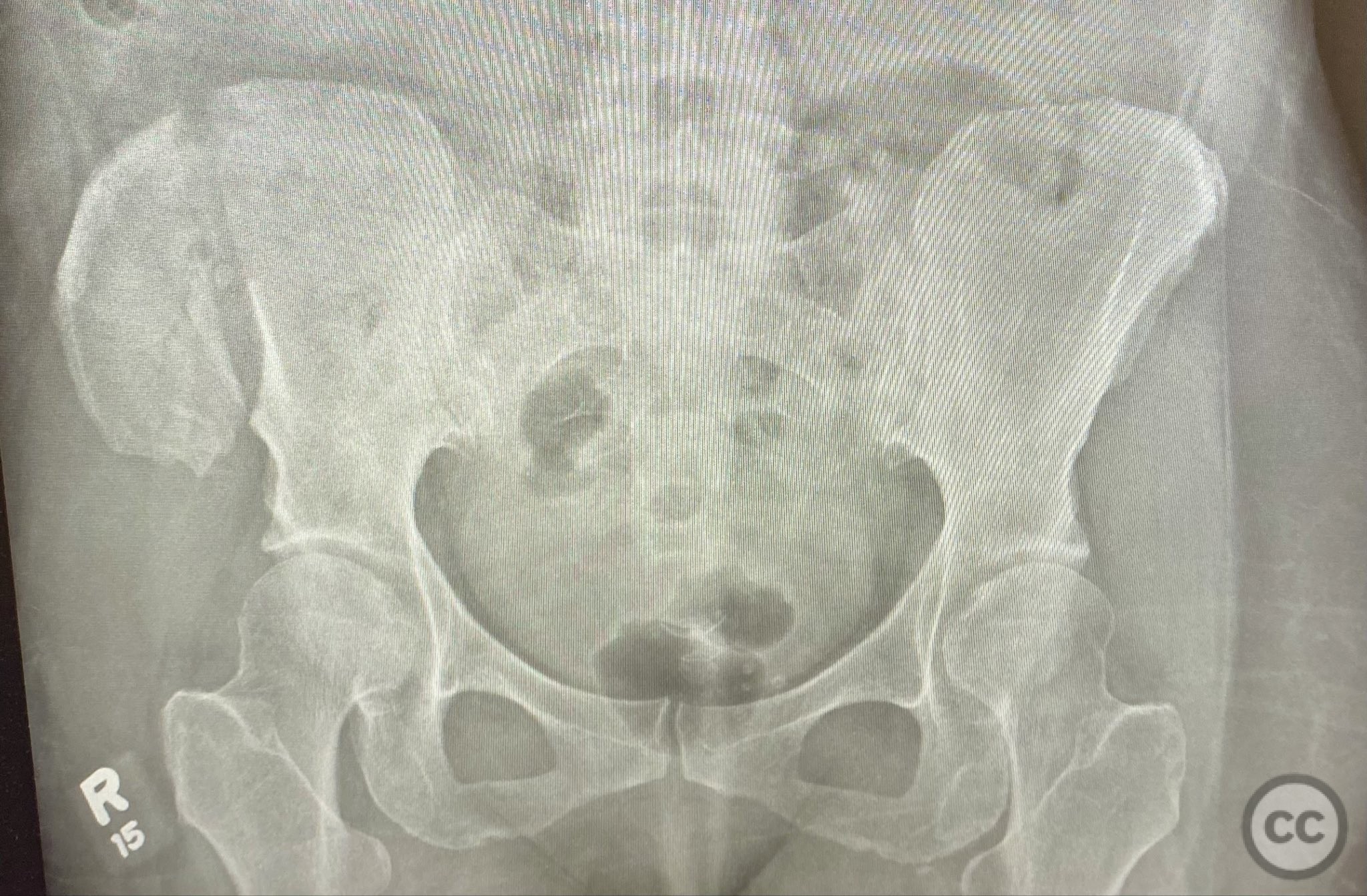
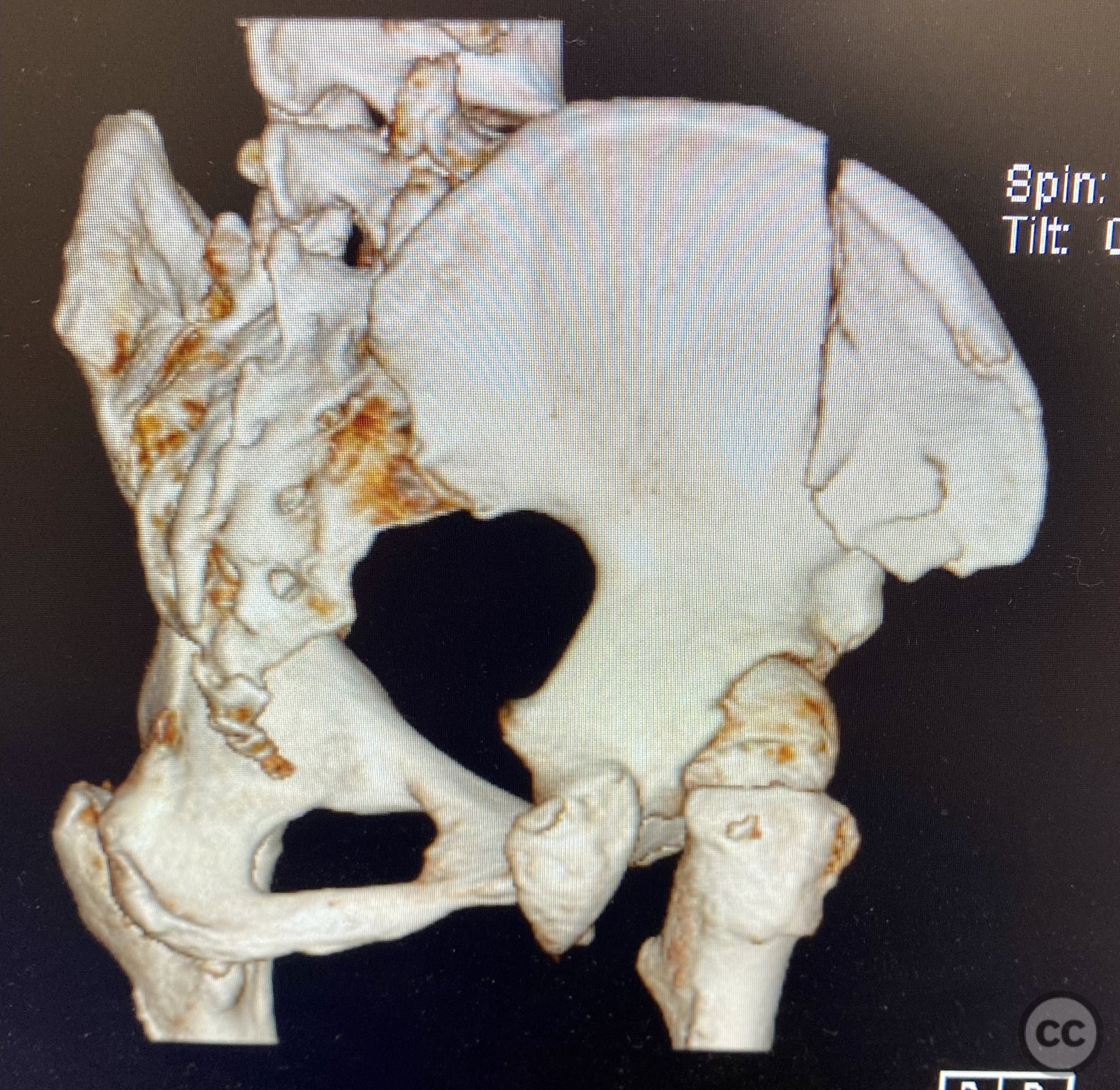
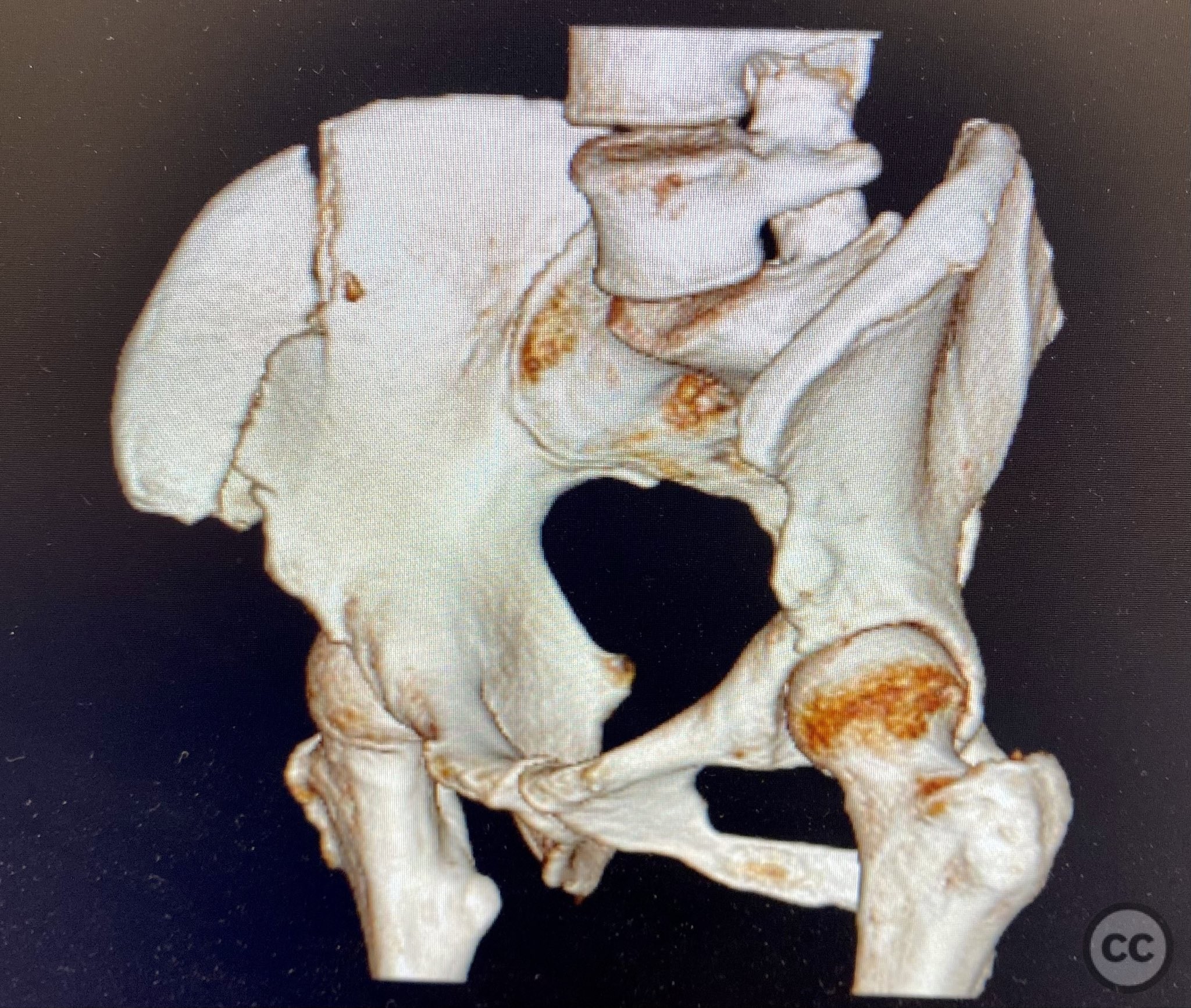
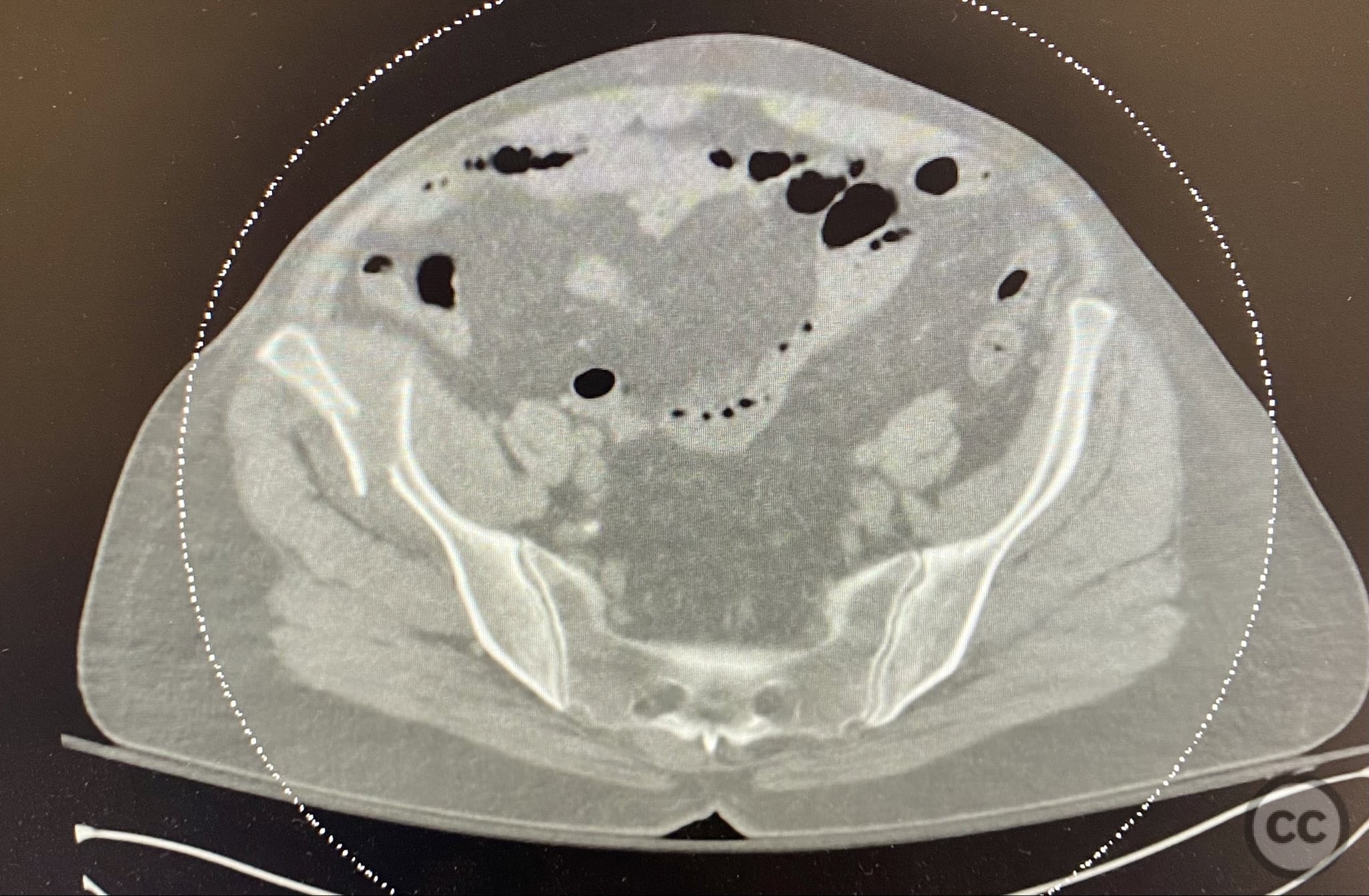
Clinical and radiological findings: A middle-aged patient sustained a closed, displaced, and comminuted fracture of the right os ilium following a fall from height. Initial AP pelvic radiograph and 3D surface rendered imaging demonstrated significant comminution, displacement, and poor bone quality. The patient was unable to mobilize due to pain. No associated neurovascular deficit or additional pelvic ring injury was reported. AO/OTA classification: 61B2.2 (partial articular, comminuted iliac wing fracture).
Preoperative Plan
Planning remarks: The preoperative plan was for open reduction and internal fixation via an iliac approach, with extension medially as required for visualization. Reduction was to be achieved with direct manipulation and clamping, followed by lag screw fixation between the inner and outer iliac tables, and supplemental fixation with a contoured and tensioned plate.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent table, with a bump under the ipsilateral flank to elevate the hemipelvis and facilitate lateral access to the iliac wing.
Anatomical surgical approach: A longitudinal incision was made over the iliac crest, extending from the anterior superior iliac spine (ASIS) posteriorly along the crest. Subperiosteal dissection exposed both the outer and inner tables of the os ilium. The exposure was extended medially to include the lateral half of the inguinal portion of an ilioinguinal approach, providing broad visualization of the fossa iliaca interna for fracture debridement, manipulation, reduction, and application of clamps. Careful preservation of the origins of musculus gluteus medius and minimus laterally, and musculus iliacus medially, was maintained.
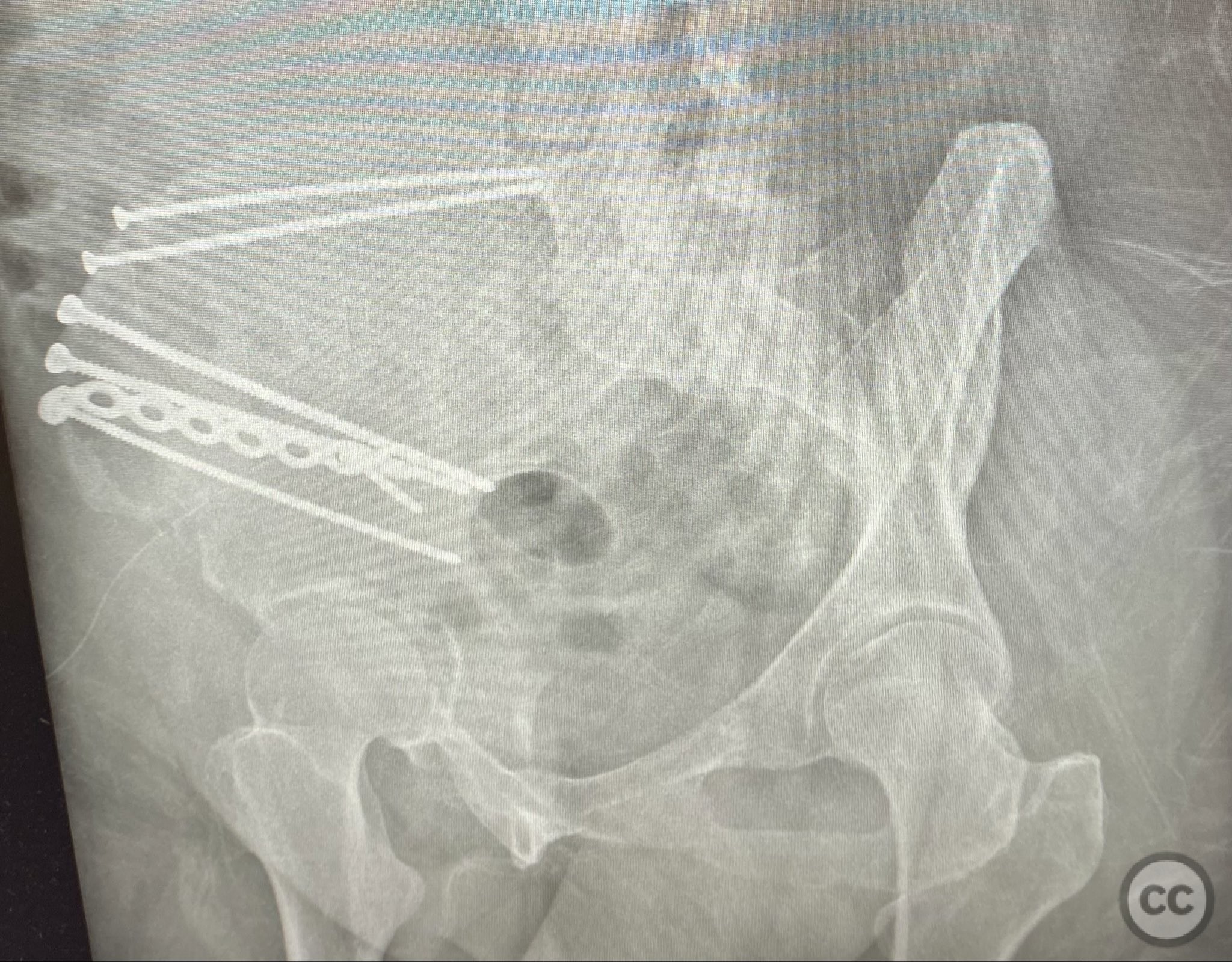
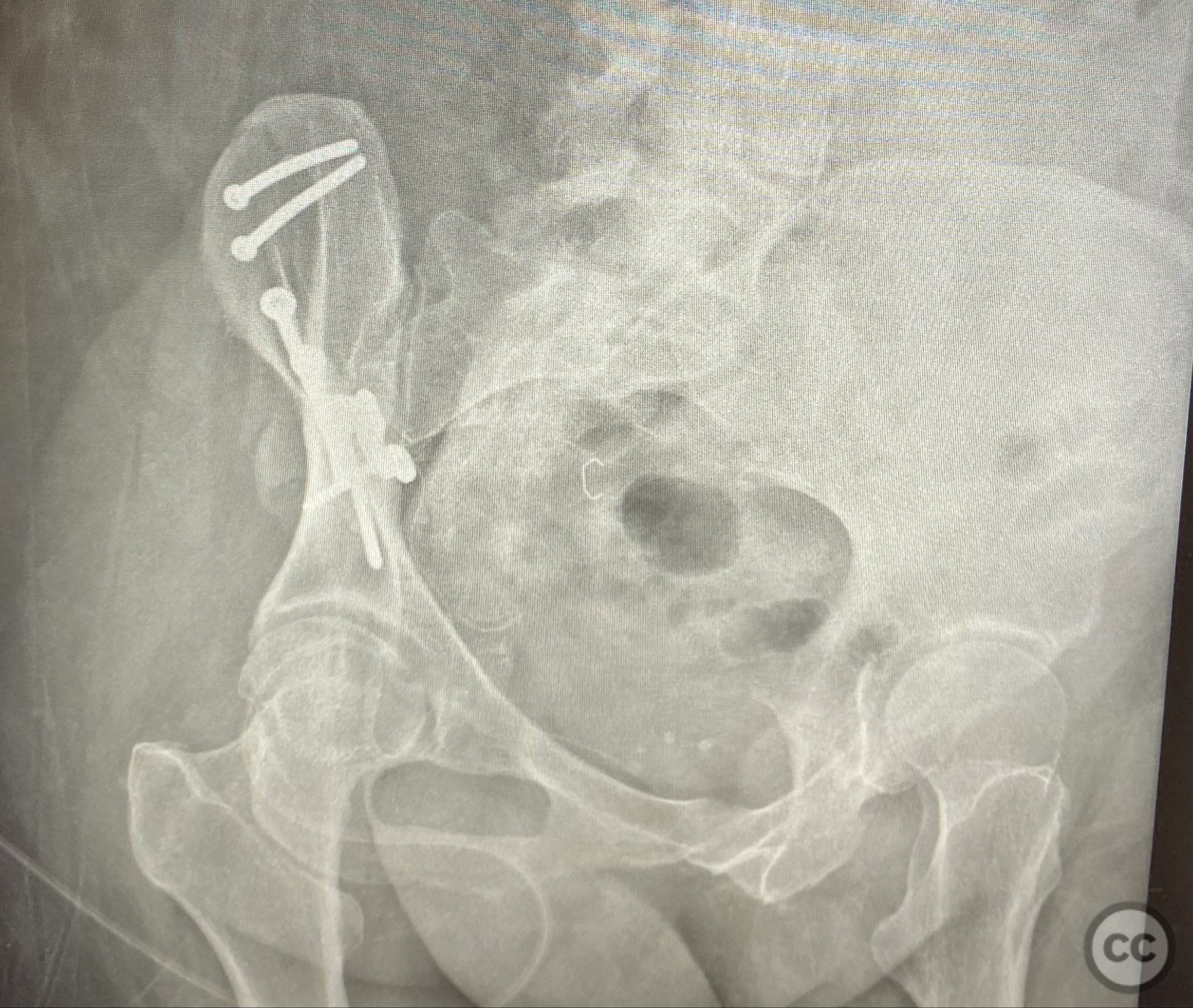
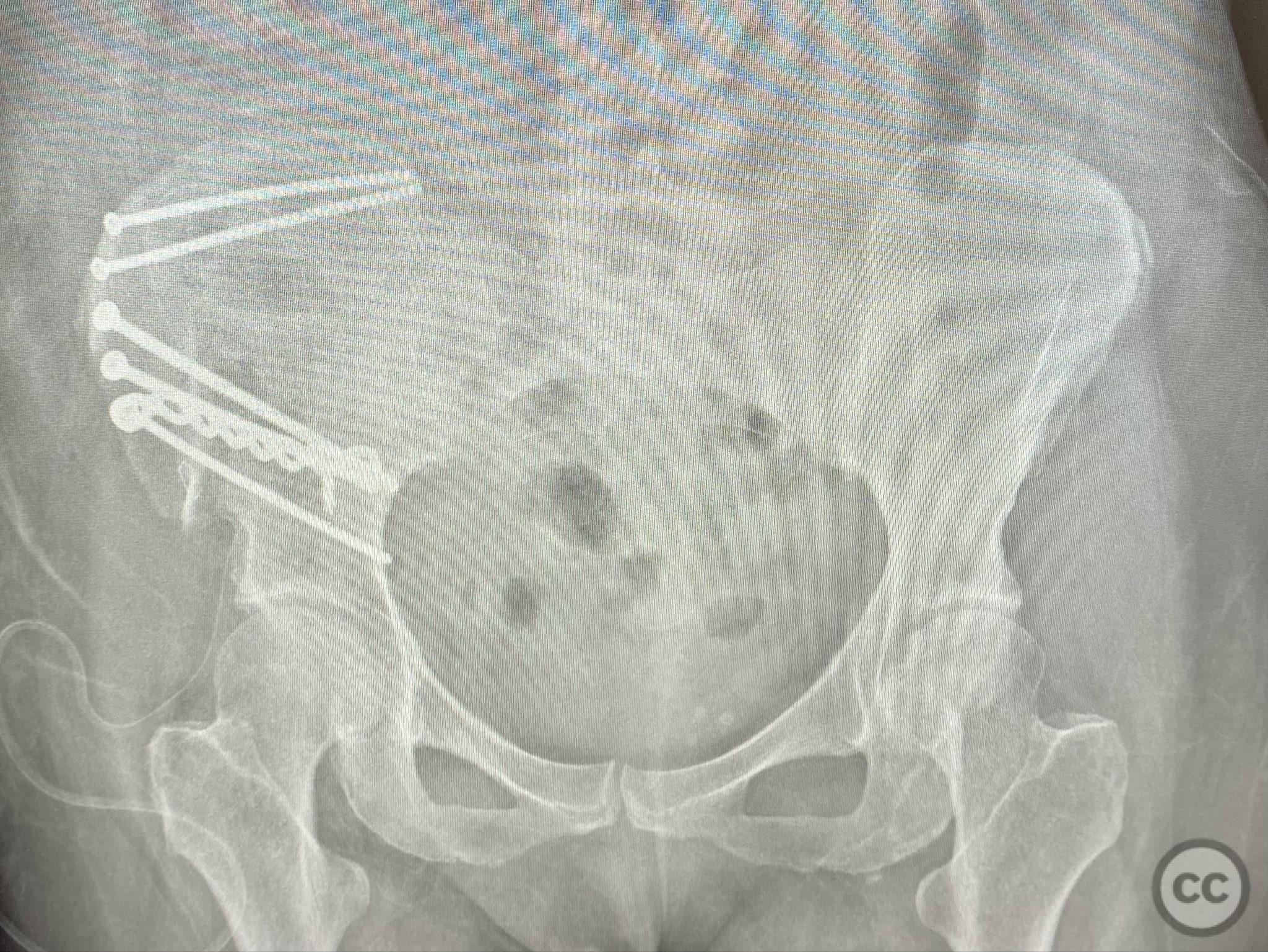
Operative remarks:The comminuted fragments were mobilized and reduced using pointed reduction forceps and ball-spike pushers under direct vision. Lag screws were placed transversely between the inner and outer cortical tables of the ilium to achieve interfragmentary compression across major fracture lines. A pre-contoured reconstruction plate was then applied along the crest and tensioned to supplement the lag screws, providing additional stability across zones of comminution. The expanded exposure facilitated thorough cleaning of hematoma and debris, precise reduction, and secure clamp placement during fixation.
Postoperative protocol: Postoperatively, toe-touch weight bearing with crutches was instituted for 8 weeks. Active-assisted range of motion exercises for hip and knee were commenced immediately. Progressive weight bearing was planned from week 9 onwards, contingent on radiographic evidence of healing.
Follow up: Not specified
Orthopaedic implants used: 3.5mm cortical lag screws; pre-contoured 3.5mm reconstruction plate
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 309 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Operative Stabilization of Displaced Comminuted Iliac Fracture with Lag Screws and Plate. Journal of Orthopaedic Surgery and Traumatology. Case Report 856681 Published Online Sep 12 2025.