






Interprosthetic Femur Fracture with Osteopenic Bone Management
Score and Comment on this Case
Clinical Details
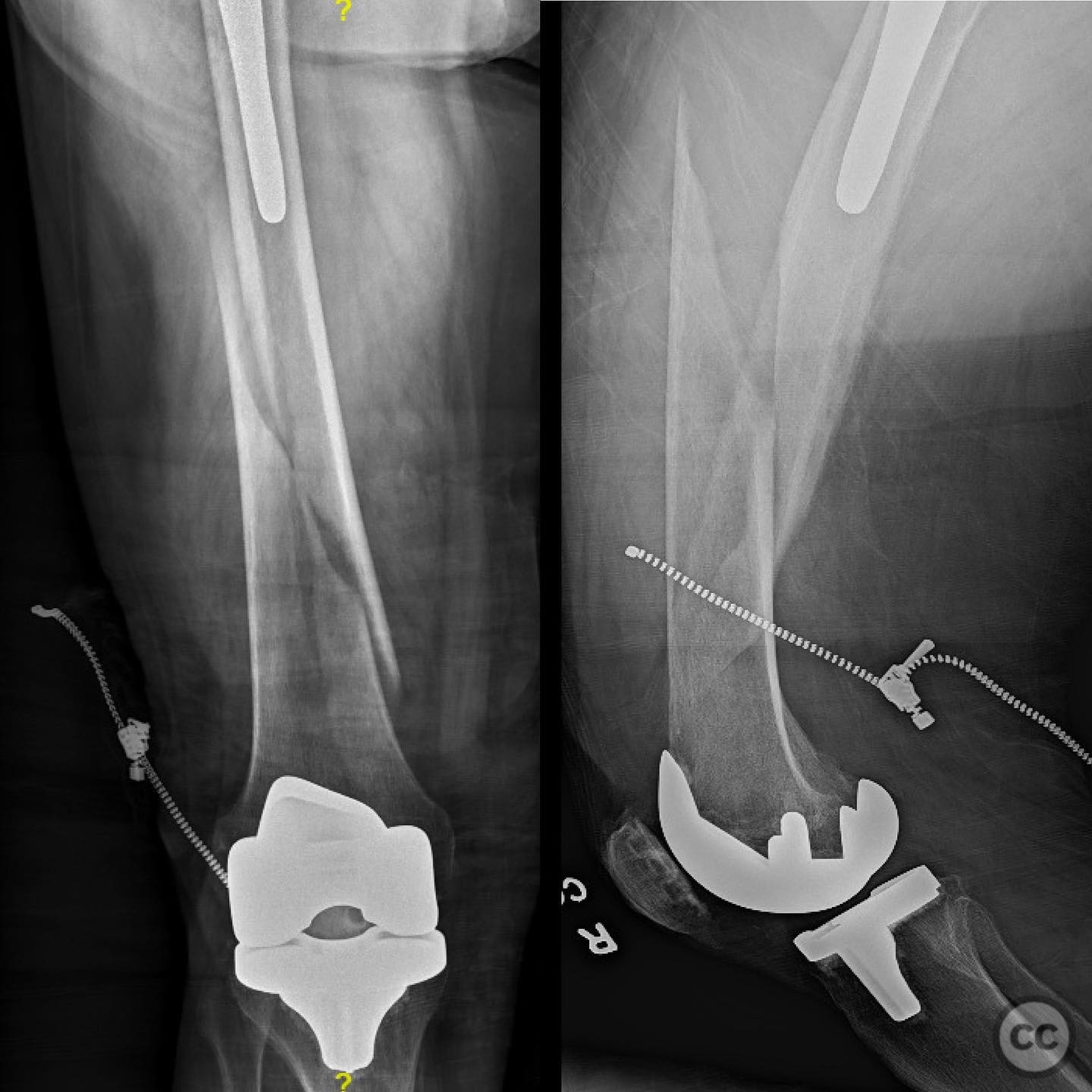
Clinical and radiological findings: A 73-year-old female patient presented following a fall down the stairs, resulting in an interprosthetic femur fracture. The patient has a history of total hip arthroplasty (THA) and total knee arthroplasty (TKA) performed 5 and 8 years ago, respectively, both of which are functioning well. The patient has no major medical comorbidities. Radiographic evaluation confirmed the presence of an interprosthetic fracture between the femoral components of the THA and TKA. The fracture is classified as an AO/OTA 32-C3 fracture, indicating a complex diaphyseal fracture.
Preoperative Plan
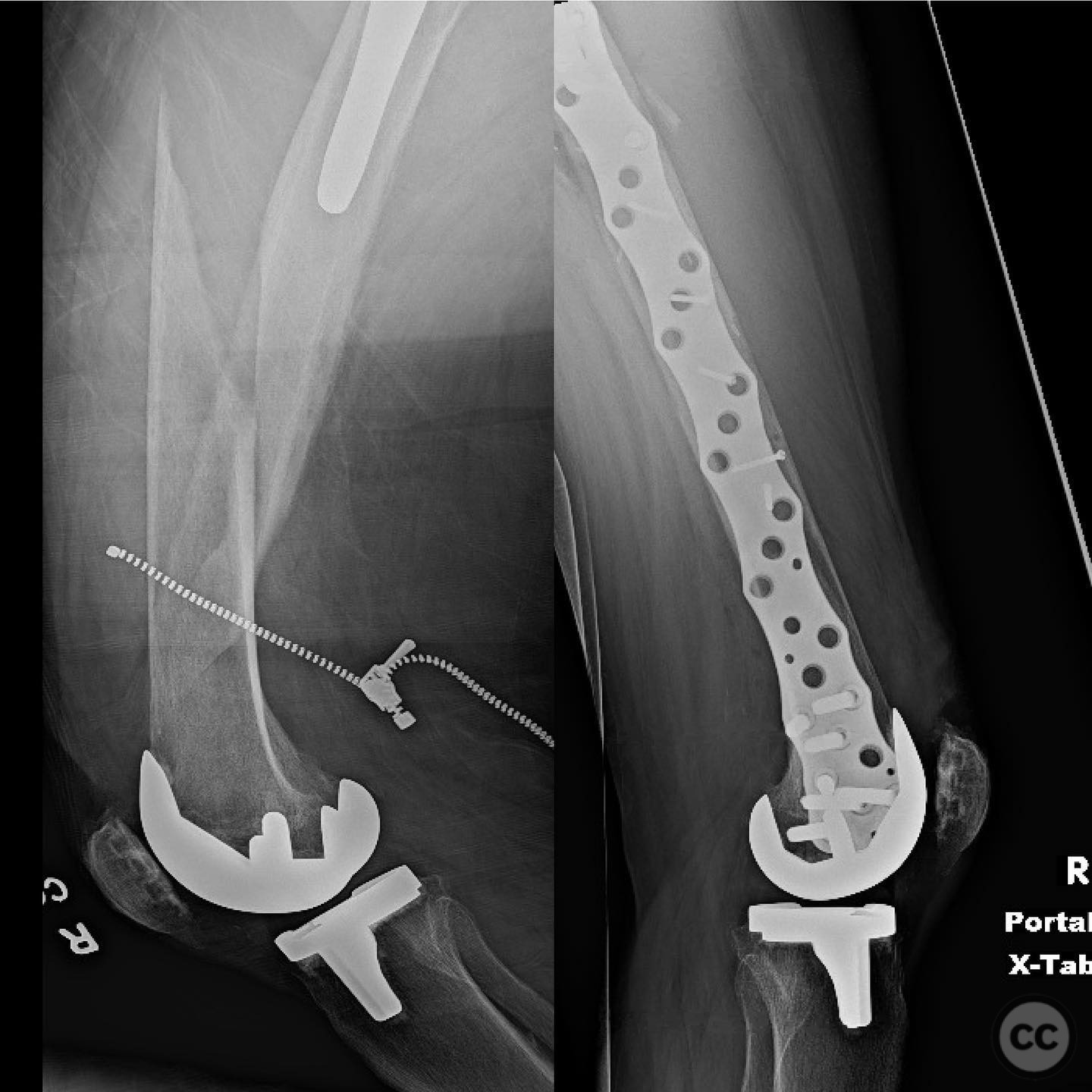
Planning remarks: The preoperative plan involves a lateral approach to the femur, aiming to achieve relative stability through bridge plating. The strategy includes restoring length, alignment, and rotation while preserving the fracture hematoma to facilitate secondary bone healing via endochondral ossification. A stout plate with maximum working length and low screw density is planned to allow early weight bearing.
Surgical Discussion
Patient positioning: The patient is positioned supine on a radiolucent table to facilitate intraoperative imaging and access to the lateral aspect of the femur.
Anatomical surgical approach: A lateral approach to the femur is utilized, involving an incision over the lateral aspect of the thigh. Dissection proceeds through the fascia lata, with careful subperiosteal elevation of the vastus lateralis muscle to expose the femoral shaft. Care is taken to preserve soft tissue attachments and fracture hematoma.
Operative remarks:The surgeon notes that achieving high-quality reduction in terms of length, coronal and sagittal plane alignment, and rotation is critical. The use of a bridge plate with low screw density allows for controlled interfragmentary motion, promoting secondary bone healing. The technique avoids the use of lag screws due to osteopenic bone quality, which would not provide sufficient grip for absolute stability.
Postoperative protocol: Postoperative rehabilitation includes early weight bearing as tolerated, with progression based on clinical and radiographic evidence of healing. Physical therapy focuses on range of motion and strengthening exercises to promote functional recovery.
Follow up: Not specified
Orthopaedic implants used: Stout bridge plate with low screw density
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 283 times
13 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Interprosthetic Femur Fracture with Osteopenic Bone Management. Journal of Orthopaedic Surgery and Traumatology. Case Report 7912662 Published Online Jul 13 2025.