












Posterior Medial Dome Impaction in Associated Acetabular Fracture: Direct Access via Ilioinguinal Approach
Score and Comment on this Case
Clinical Details
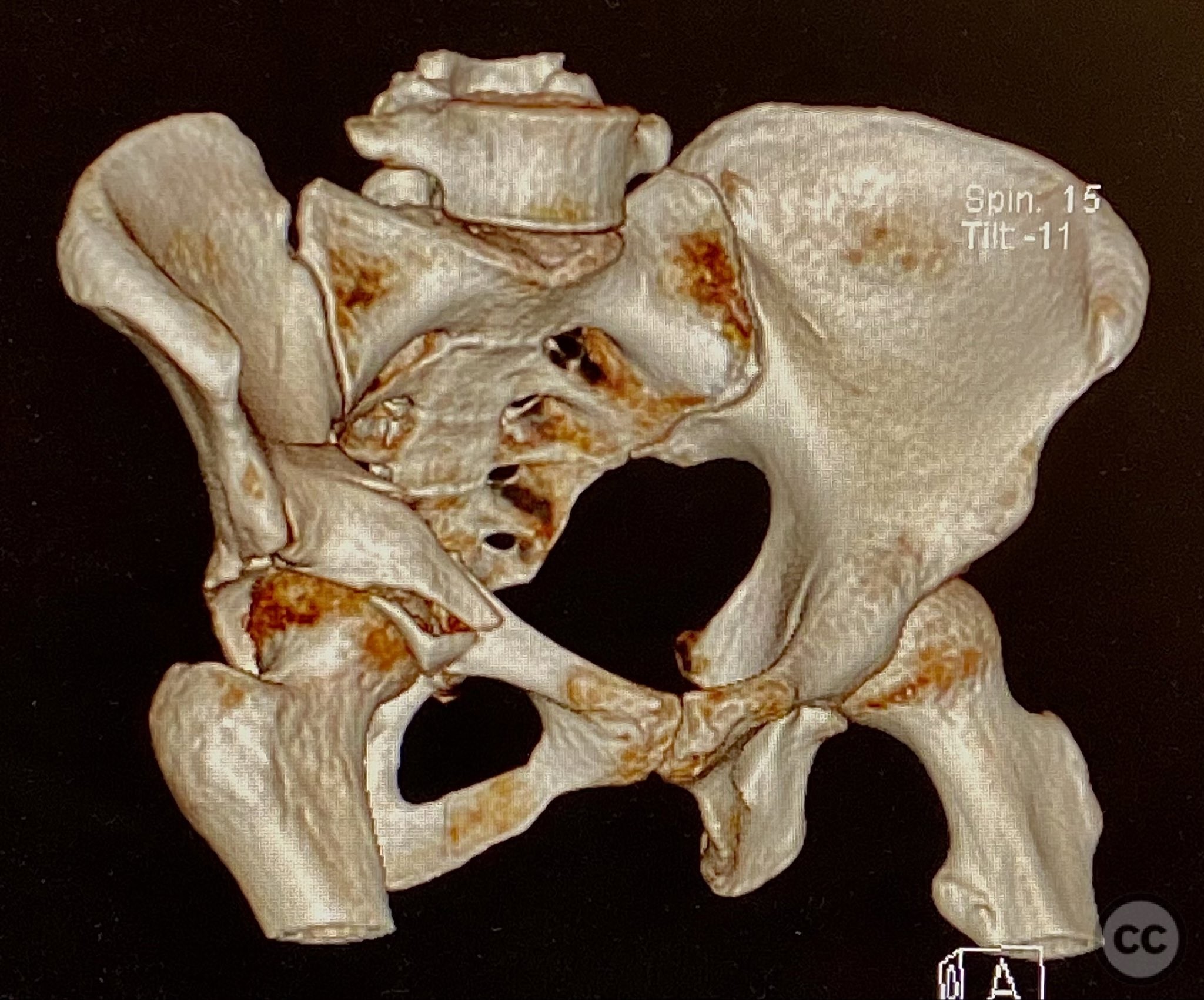
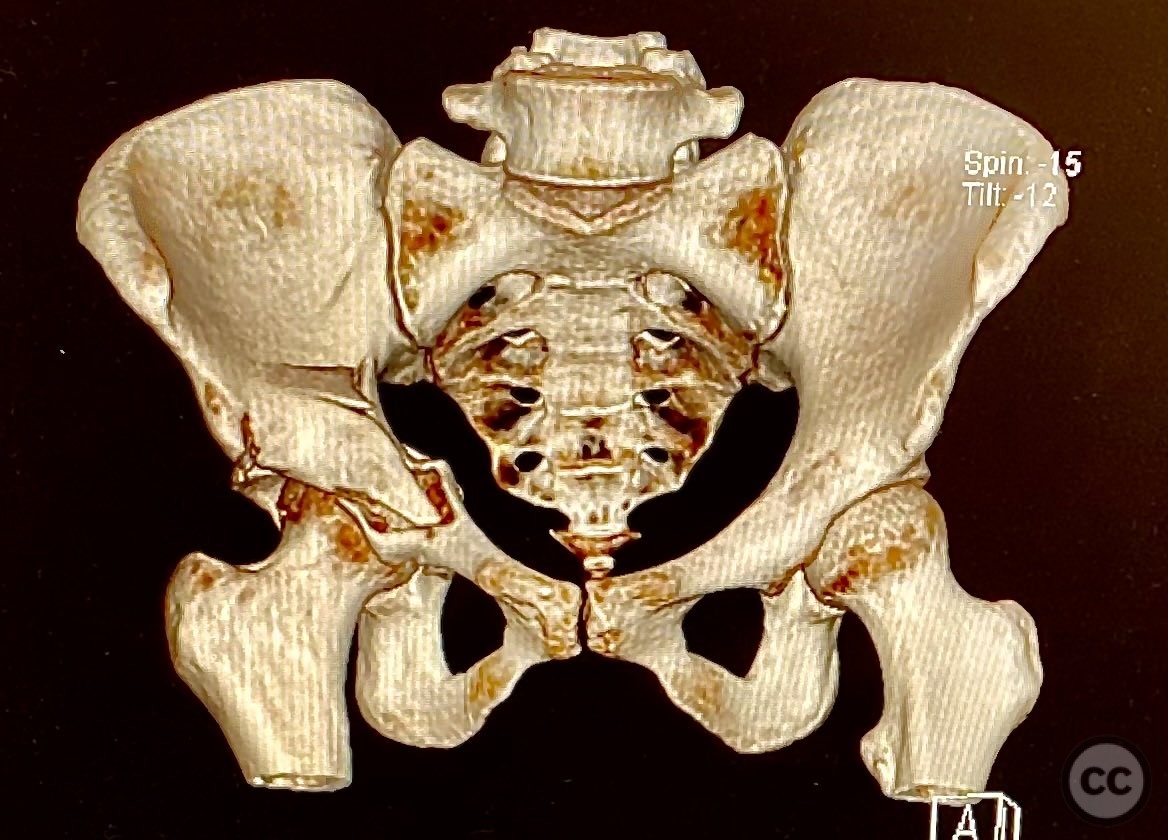
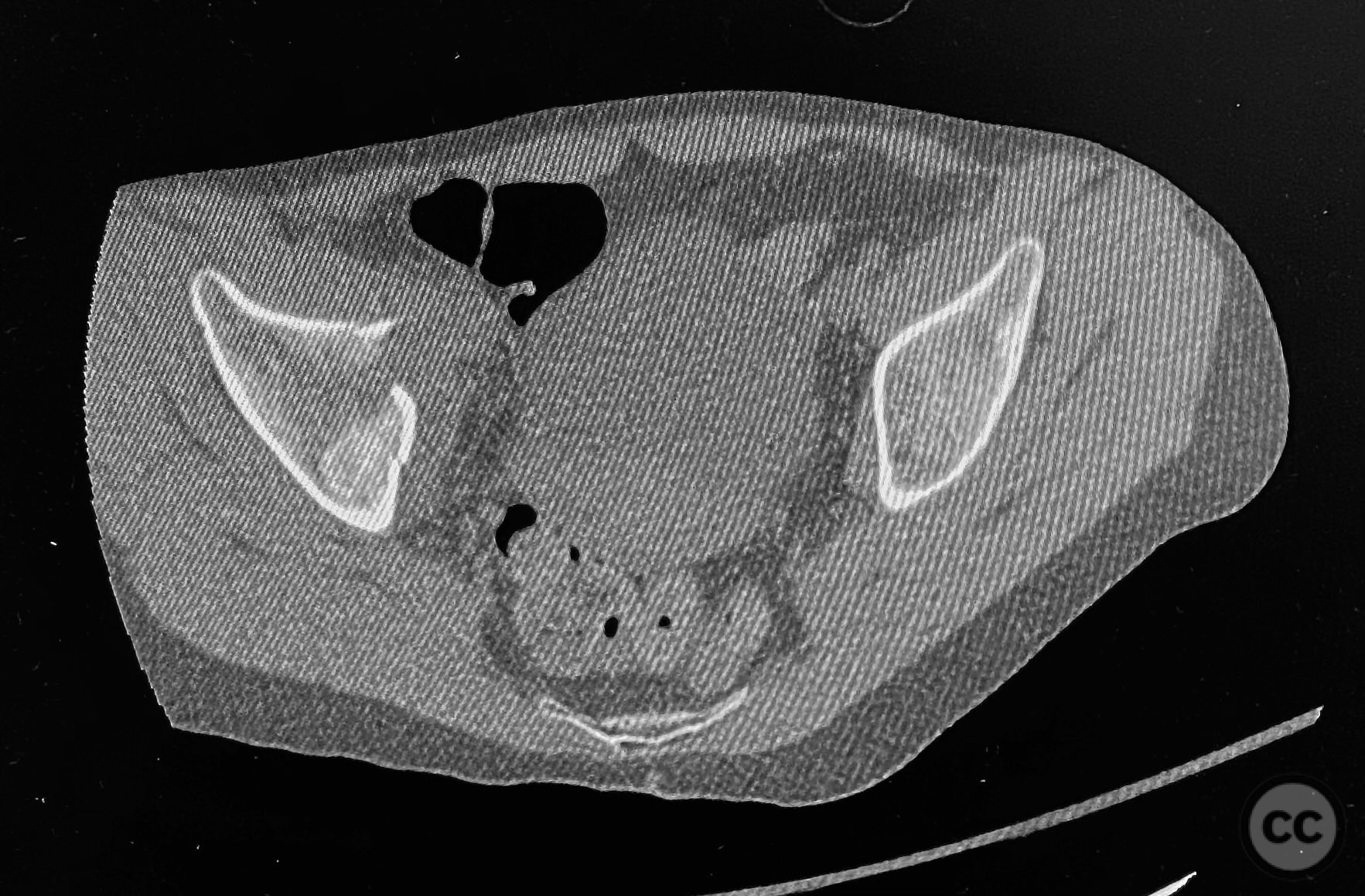
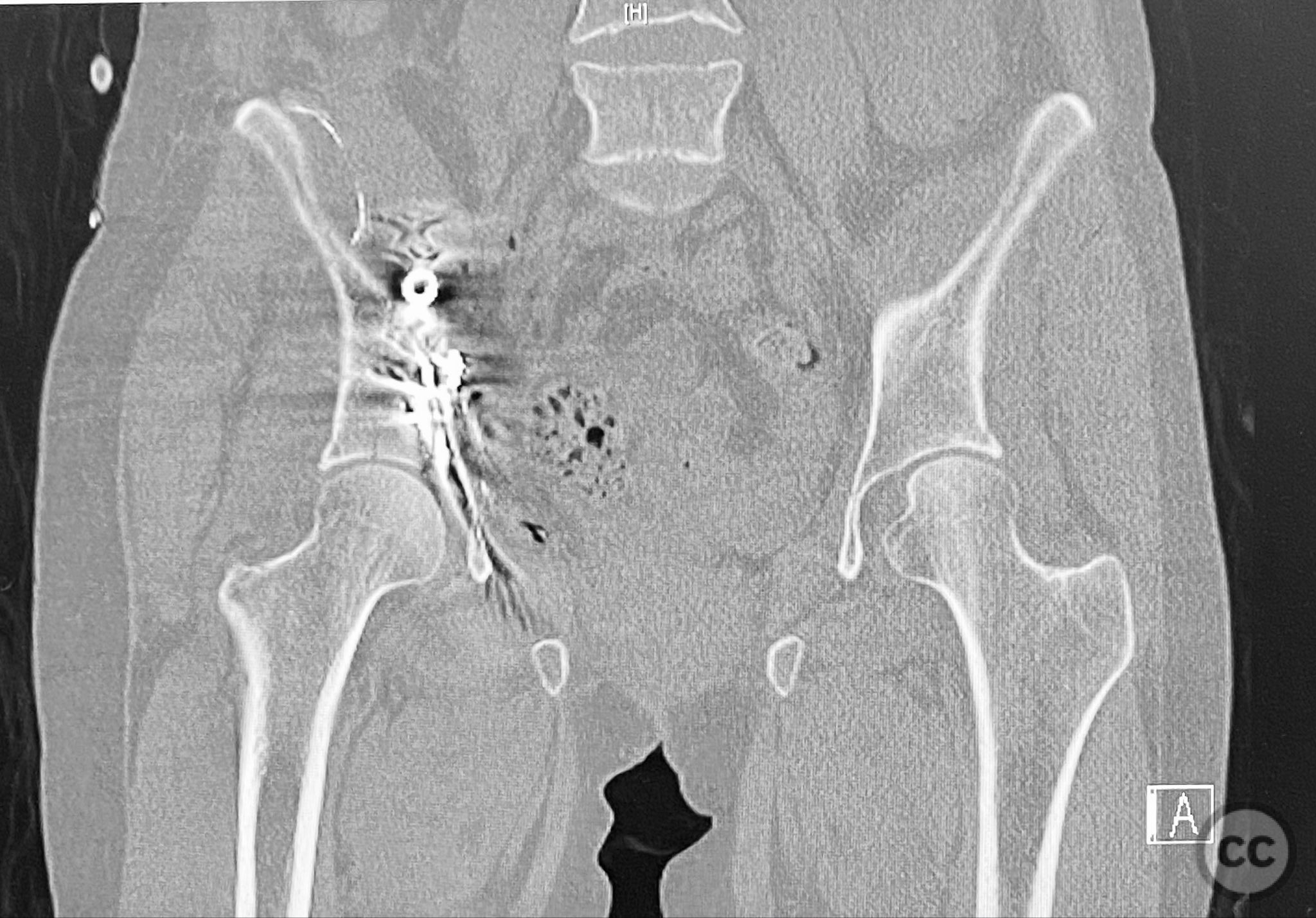
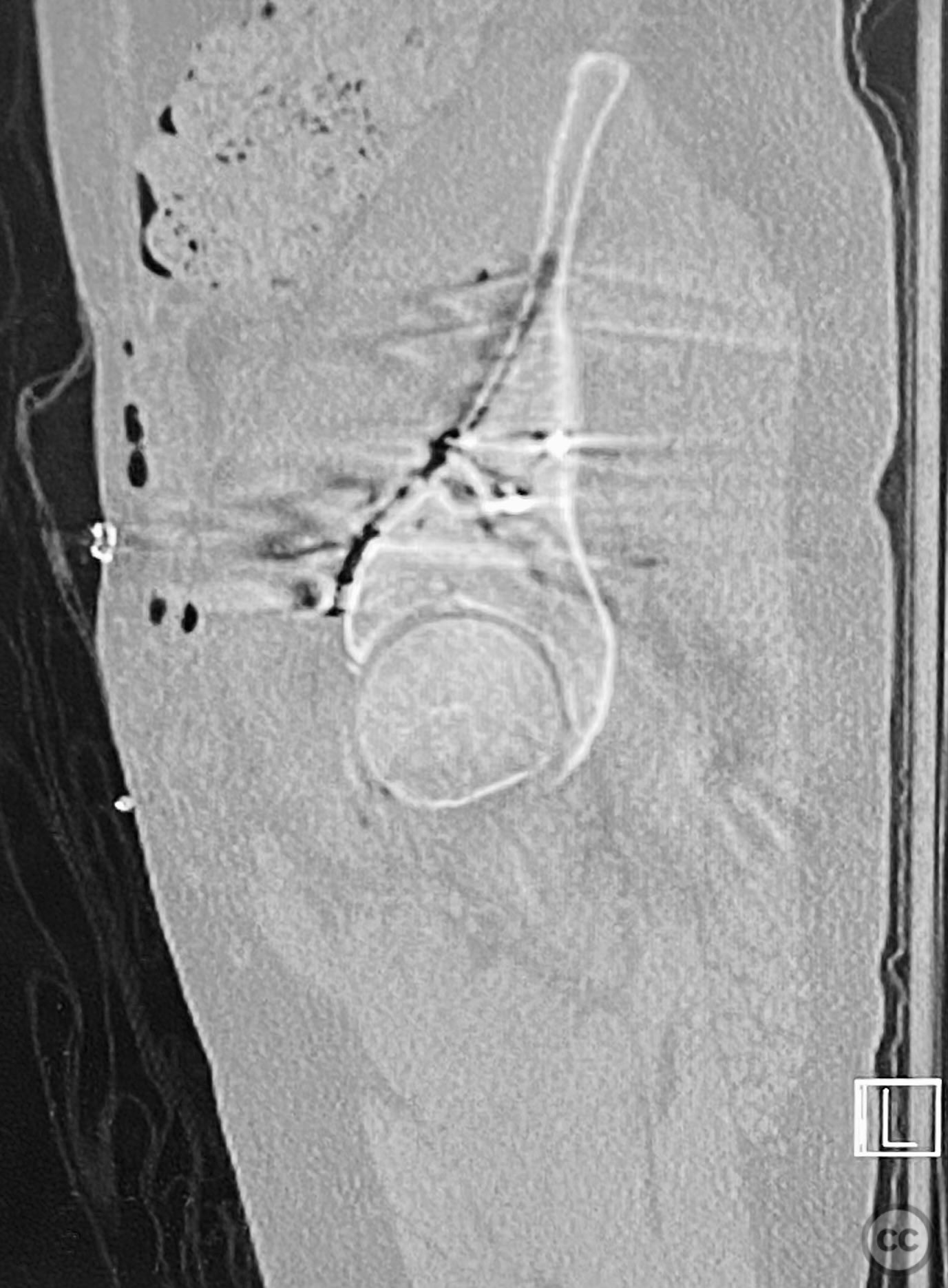
Clinical and radiological findings: The patient sustained an acetabular fracture with a rare posterior medial dome impaction fragment, as demonstrated on AP pelvic radiographs obtained in skeletal traction. Surface renderings and axial CT images revealed multiple incomplete fracture lines, including a rhomboid-shaped cortical fragment adjacent and proximal to the anterior column/wall fragment. Coronal and sagittal reconstructions further delineated the impacted articular fragment and its relationship to the surrounding acetabular dome. The fracture pattern is classified as AO/OTA 62B3 (associated both-column fracture with dome impaction).
Preoperative Plan
Planning remarks: The preoperative plan involved an ilioinguinal approach to the acetabulum, utilizing the intrapelvic interval for initial reduction and stabilization of the posterior column with a contoured intrapelvic plate. Sequential reduction of the anterior column and direct management of the impacted dome fragment were planned, facilitated by temporary removal of the rhomboid cortical fragment.
Surgical Discussion
Patient positioning: The patient was positioned supine on a standard operating table without traction.
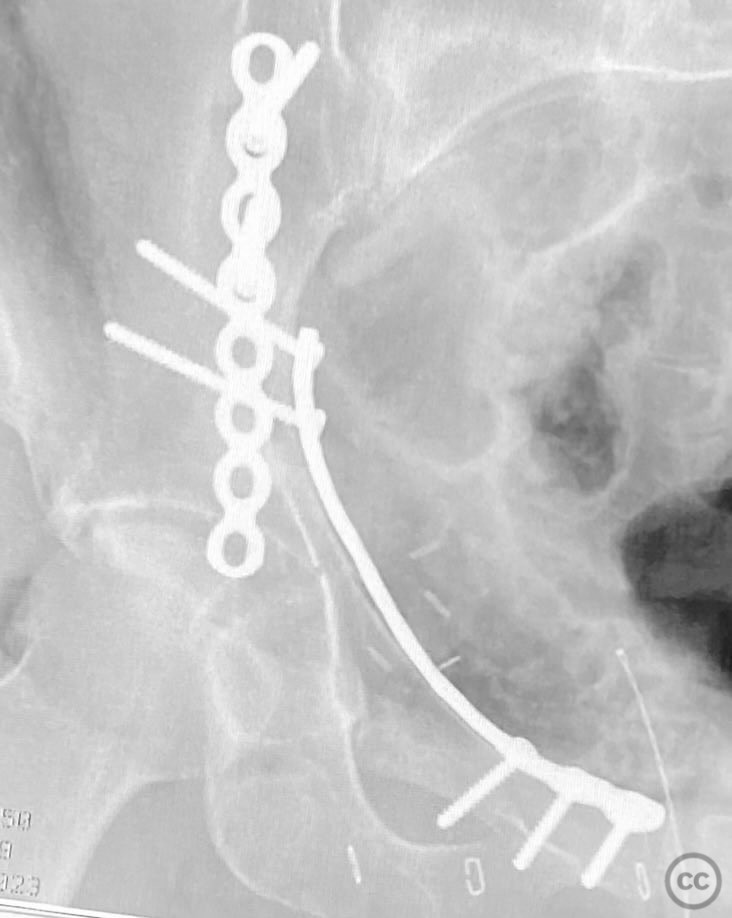
Anatomical surgical approach: A classical ilioinguinal approach was performed, developing the lateral, middle, and medial windows. The intrapelvic interval was used to access the quadrilateral surface and posterior column. The rhomboid cortical fragment was excised to allow direct visualization and manipulation of the impacted posterior medial dome fragment. Reduction was achieved using a spiked pusher under fluoroscopic guidance. The defect was filled with morselized allograft, and the rhomboid fragment was anatomically reduced. The anterior column was stabilized with a contoured plate. Posterior column reduction was further improved using a reduction clamp applied with one tine lateral to the anterior inferior iliac spine (AIIS) and the other on the quadrilateral surface via the middle window, followed by lag screw fixation.
Operative remarks:This case demonstrates that certain impacted dome fragments, which are otherwise inaccessible, can be directly addressed by temporarily removing overlying cortical fragments. The ilioinguinal approach, specifically through the middle window, provided unobstructed access for clamp placement and direct manipulation of both anterior and posterior column fragments. Sequential reduction and stabilization were facilitated by direct visualization and intraoperative fluoroscopy, allowing for anatomical restoration of the articular surface.
Postoperative protocol: Postoperatively, the patient was maintained non-weight bearing on the affected limb for 8 weeks, with passive range of motion exercises initiated immediately. Progressive weight bearing was introduced at 8–10 weeks postoperatively based on radiographic evidence of healing.
Follow up: Not specified
Orthopaedic implants used: Contoured intrapelvic reconstruction plate, contoured anterior column plate, lag screws, morselized allograft
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 1024 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Posterior Medial Dome Impaction in Associated Acetabular Fracture: Direct Access via Ilioinguinal Approach. Journal of Orthopaedic Surgery and Traumatology. Case Report 7825826 Published Online Sep 12 2025.