






Nonunion of Supracondylar Distal Humerus with Metaphyseal Bone Loss
Score and Comment on this Case
Clinical Details
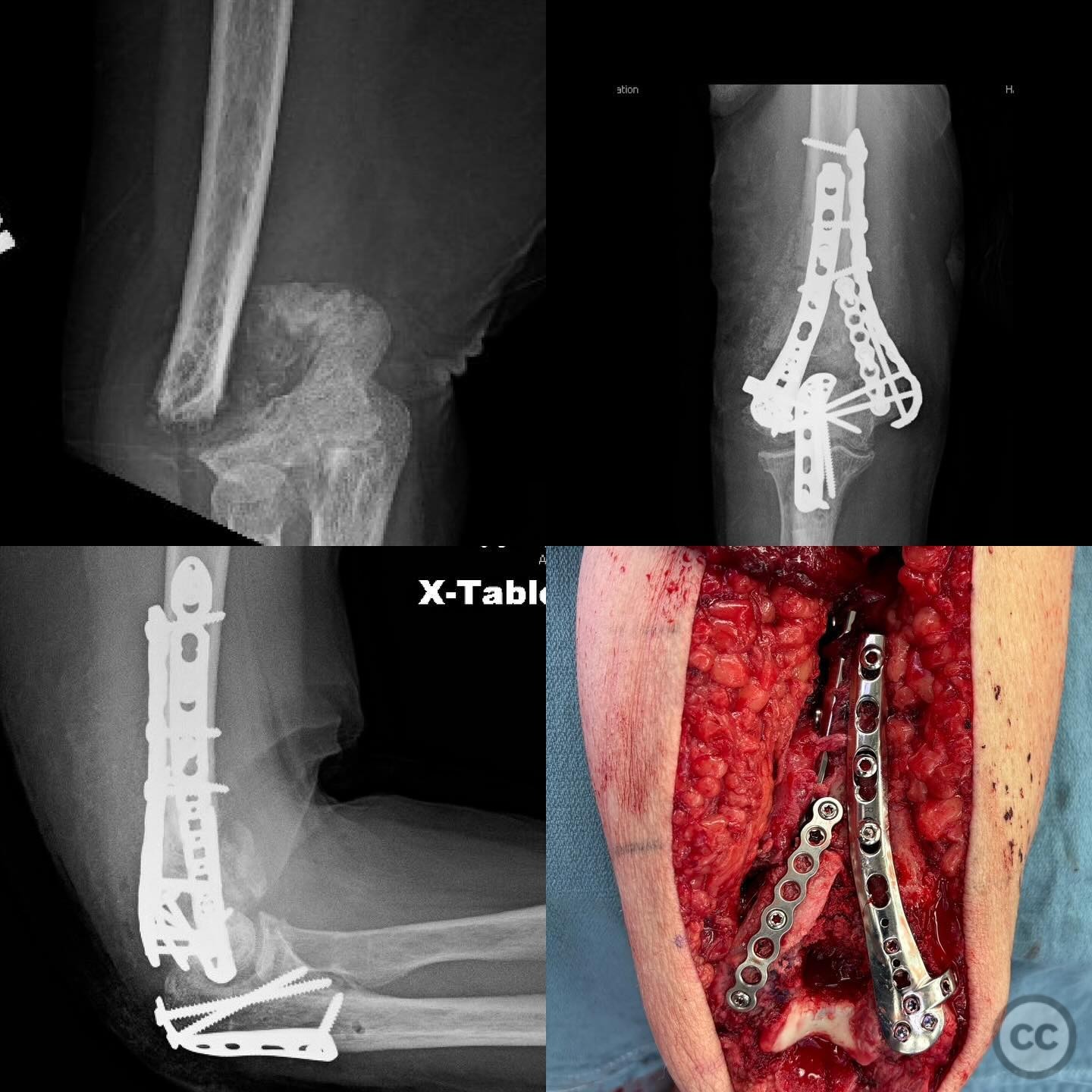
Clinical and radiological findings: A 57-year-old female with a history of a supracondylar distal humerus fracture treated non-operatively 1.5 years ago presents with pain, deformity, and inability to use the arm. The patient has non-insulin-dependent diabetes mellitus. Radiological evaluation reveals a nonunion with significant bone loss in the metaphyseal region, specifically involving the olecranon fossa. There are no metabolic, nutritional, or infectious concerns identified in the nonunion workup.
Preoperative Plan
Planning remarks: The preoperative plan involves a posterior approach to the distal humerus to address the nonunion and restore distal humeral morphology. The plan includes debridement of the synovial pseudoarthrosis, correction of coronal, sagittal, and axial alignment, and reconstruction of the bone defect using an osteoperiosteal corticocancellous graft harvested from the iliac crest.
Surgical Discussion
Patient positioning: The patient is positioned in a lateral decubitus position with the affected arm supported and draped to allow full access to the posterior aspect of the elbow.
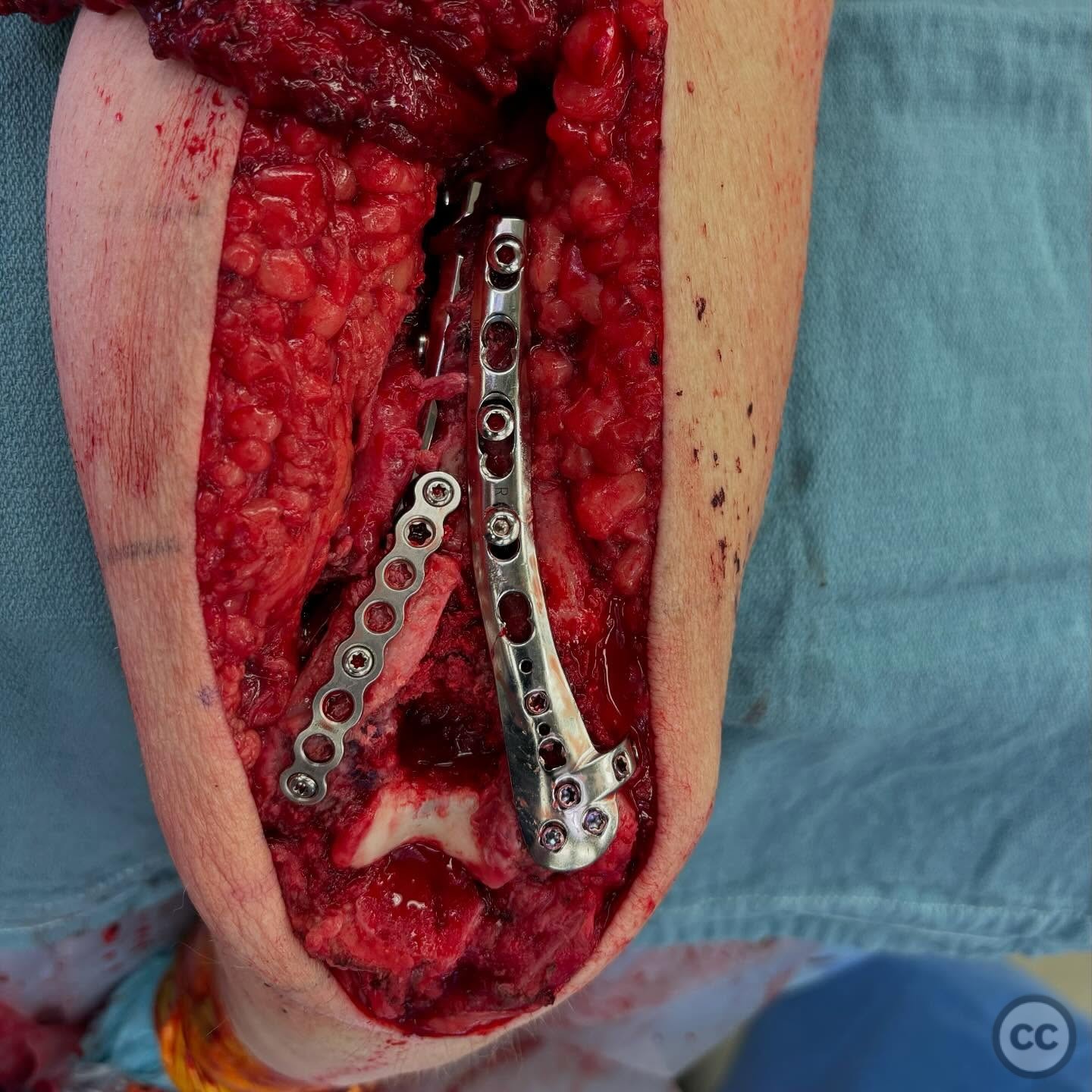
Anatomical surgical approach: A posterior approach to the distal humerus is utilized. A midline incision is made over the posterior aspect of the elbow, extending proximally and distally as needed. The triceps muscle is split in line with its fibers to expose the distal humerus. The synovial pseudoarthrosis is debrided, and alignment is restored. The residual defect is measured, and an osteoperiosteal corticocancellous graft is harvested from the gluteal pillar of the iliac crest, shaped to fit the defect, and fixed in place. The olecranon fossa is recreated using a burr.
Operative remarks:The surgeon notes that one of the major concerns in this case is elbow joint arthrofibrosis due to prolonged nonunion. To prevent motion concentration through the nonunion repair, which could be detrimental, a comprehensive 360-degree soft tissue release and debridement around the elbow joint is performed to improve range of motion.
Postoperative protocol: Postoperative rehabilitation includes early mobilization to prevent stiffness. Passive range of motion exercises are initiated immediately postoperatively, progressing to active-assisted and active range of motion as tolerated. Weight-bearing activities are restricted until radiographic evidence of union is observed.
Follow up: Not specified
Orthopaedic implants used: Osteoperiosteal corticocancellous graft from iliac crest
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 364 times
09 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Nonunion of Supracondylar Distal Humerus with Metaphyseal Bone Loss. Journal of Orthopaedic Surgery and Traumatology. Case Report 7490469 Published Online Jul 09 2025.