

Posterior Talar Body Fracture Dislocation with Medial Subtalar Dislocation.
Score and Comment on this Case
Clinical Details
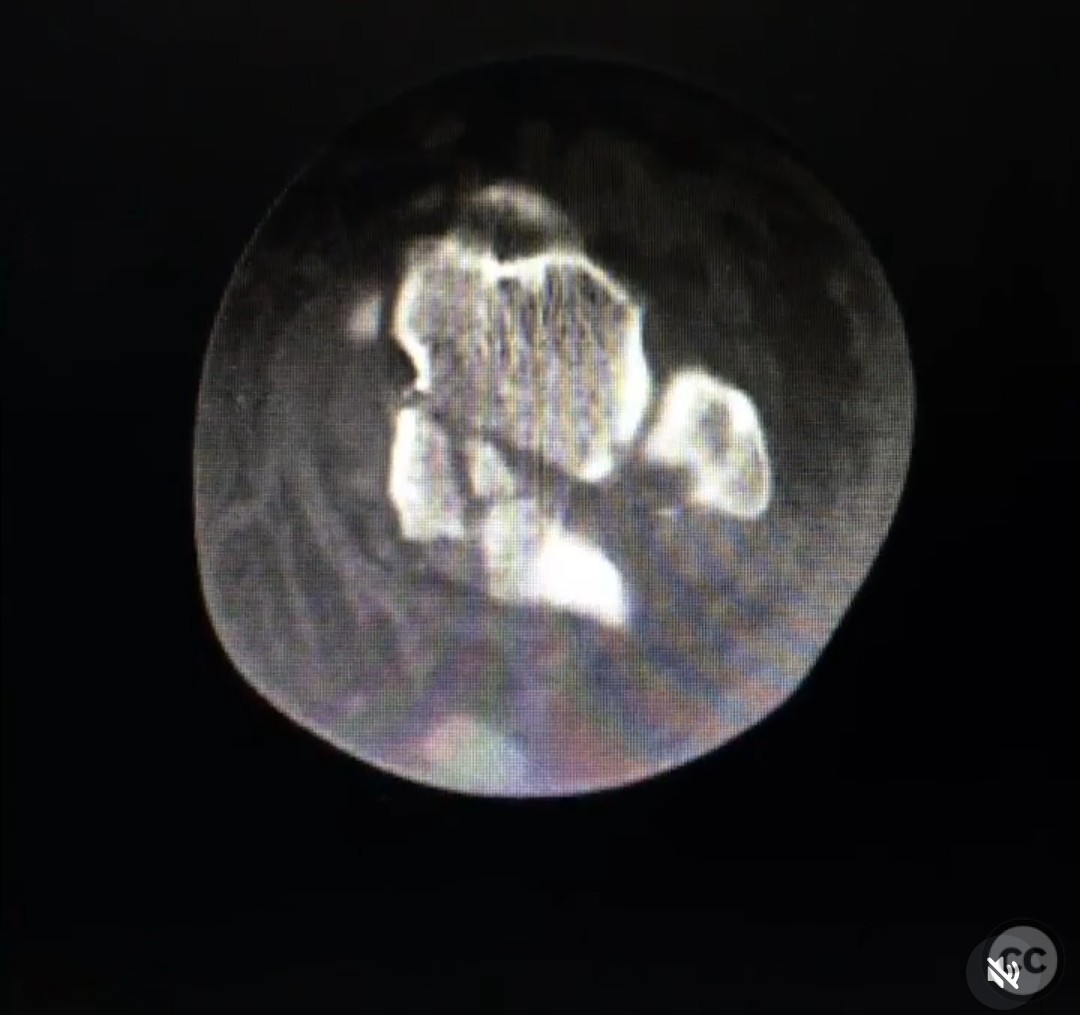
Clinical and radiological findings: A 22-year-old female sustained a closed medial subtalar fracture dislocation after falling 15 feet while bouldering. Initial management at an outside hospital included closed reduction and application of an external fixator. Axial and sagittal CT scans revealed a posterior talar body fracture dislocation. The fracture was predominantly located in the posterior half of the talar body.
Preoperative Plan
Planning remarks: The preoperative plan involved a two-stage approach. The talar head shear was addressed first using an anteromedial approach with the patient in a supine position. For the posterior talar body fracture, a posteromedial approach was planned with the patient in a prone position, utilizing distraction to enhance visualization of the tibiotalar and subtalar joints.
Surgical Discussion
Patient positioning: The patient was initially positioned supine for the anteromedial approach to address the talar head shear. Subsequently, the patient was repositioned prone for the posteromedial approach to access the posterior talar body fracture.
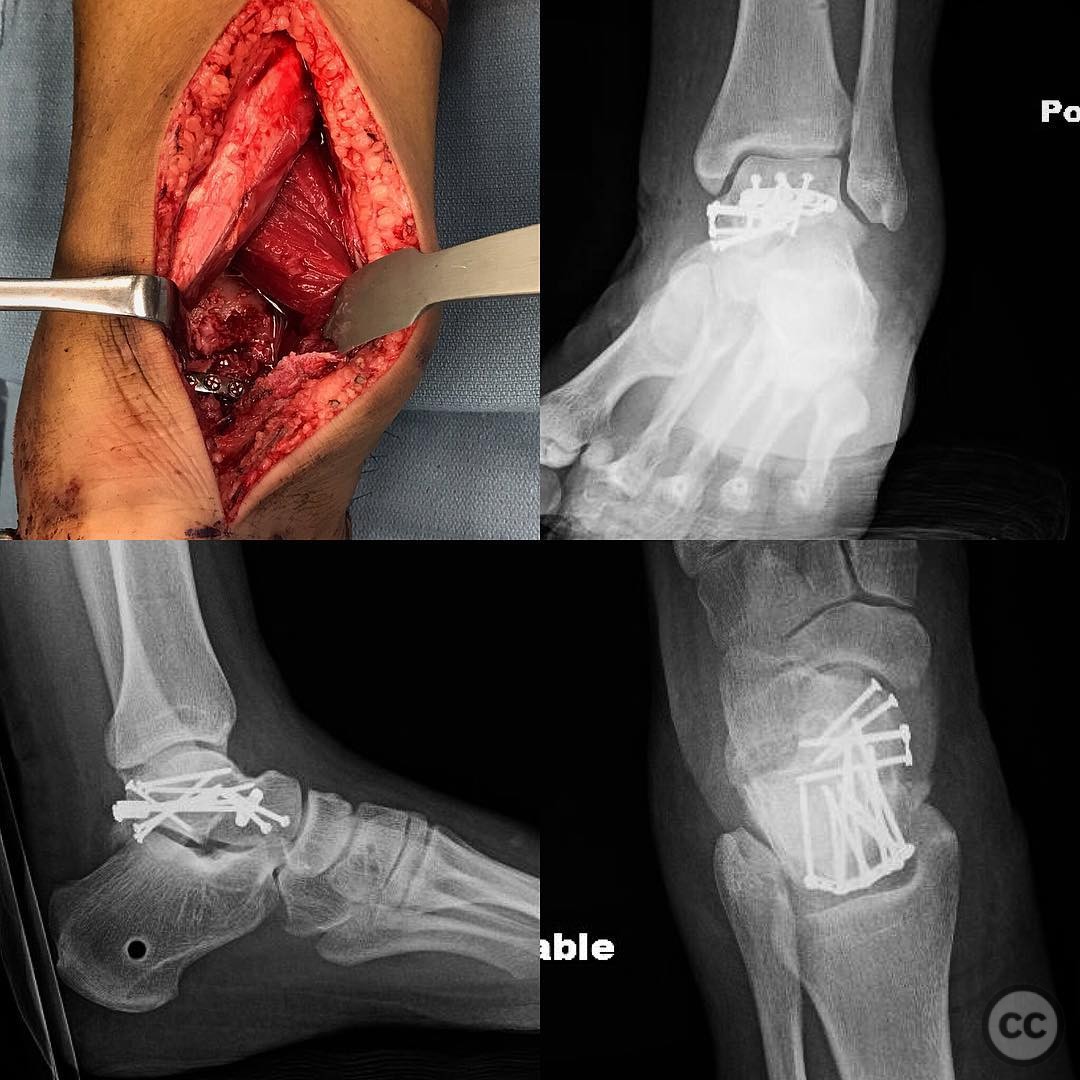
Anatomical surgical approach: The anteromedial approach involved an incision over the anteromedial aspect of the ankle, allowing access to the talar head. For the posteromedial approach, a skin incision was made just medial to the Achilles tendon. The Achilles tendon was retracted laterally, and the deep posterior compartment was retracted medially. A large Homan retractor was used to protect the neurovascular bundle.
Operative remarks:The talar head shear was fixed first with the patient supine using an anteromedial approach. The posteromedial approach required distraction to improve visualization of the tibiotalar and subtalar joints, which was crucial for accessing the posterior talar body fracture. Without distraction, this approach would have been ineffective. Fixation was achieved using 1.5 and 2.0 mm screws and plates.
Postoperative protocol: Postoperative rehabilitation included immobilization in a splint for initial healing, followed by gradual weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness, with progression to strengthening exercises as healing allowed.
Follow up: Not specified.
Orthopaedic implants used: 1.5 mm screws, 2.0 mm screws, plates.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 317 times
04 Aug 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Posterior Talar Body Fracture Dislocation with Medial Subtalar Dislocation.. Journal of Orthopaedic Surgery and Traumatology. Case Report 7117332 Published Online Aug 04 2025.