











Talar Body Fracture Dislocation with Medial Malleolus Osteotomy
Score and Comment on this Case
Clinical Details
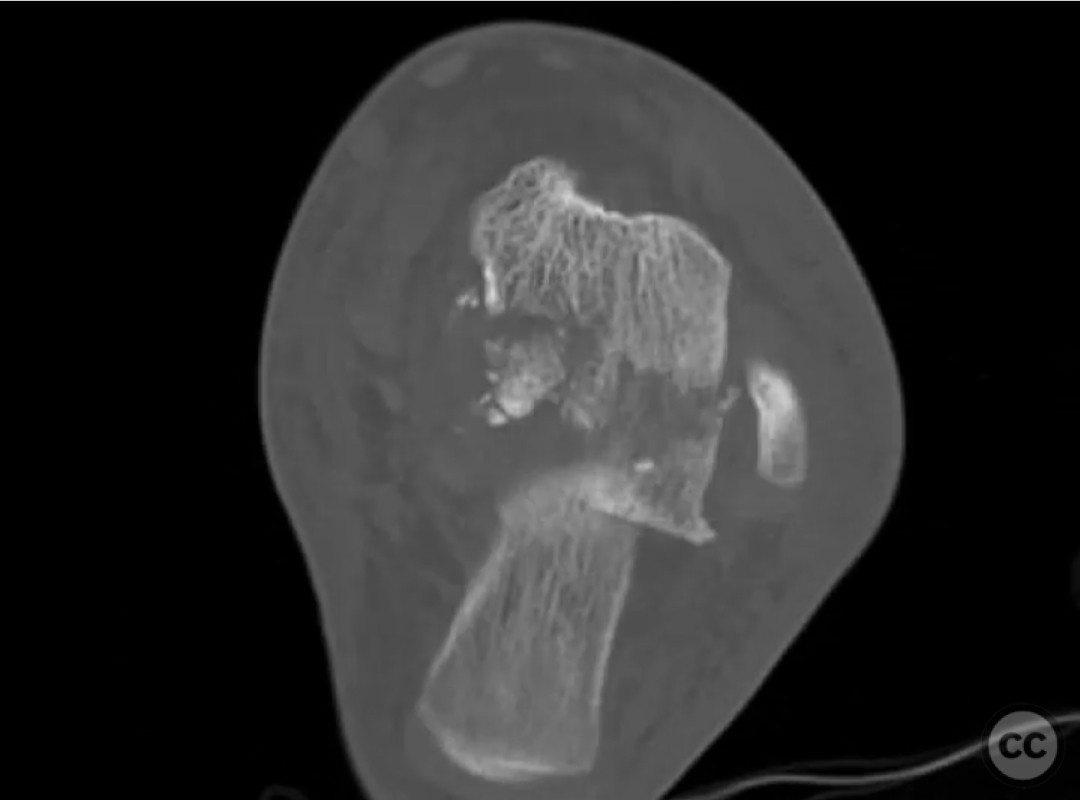
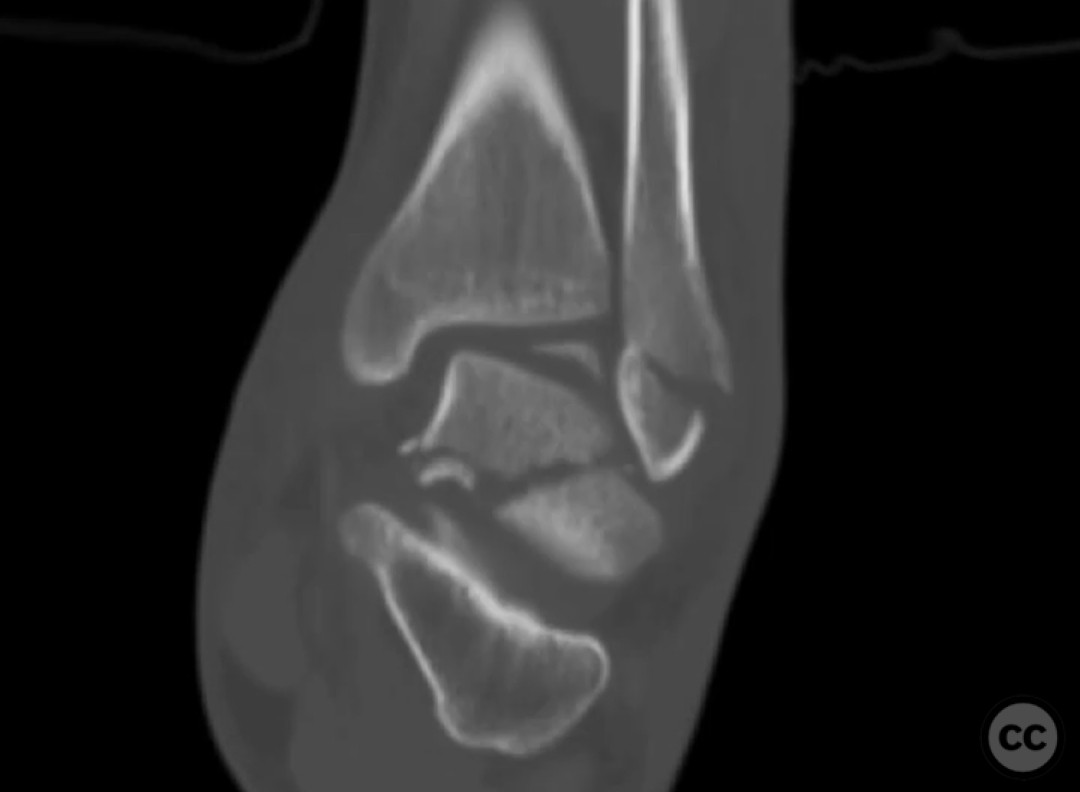
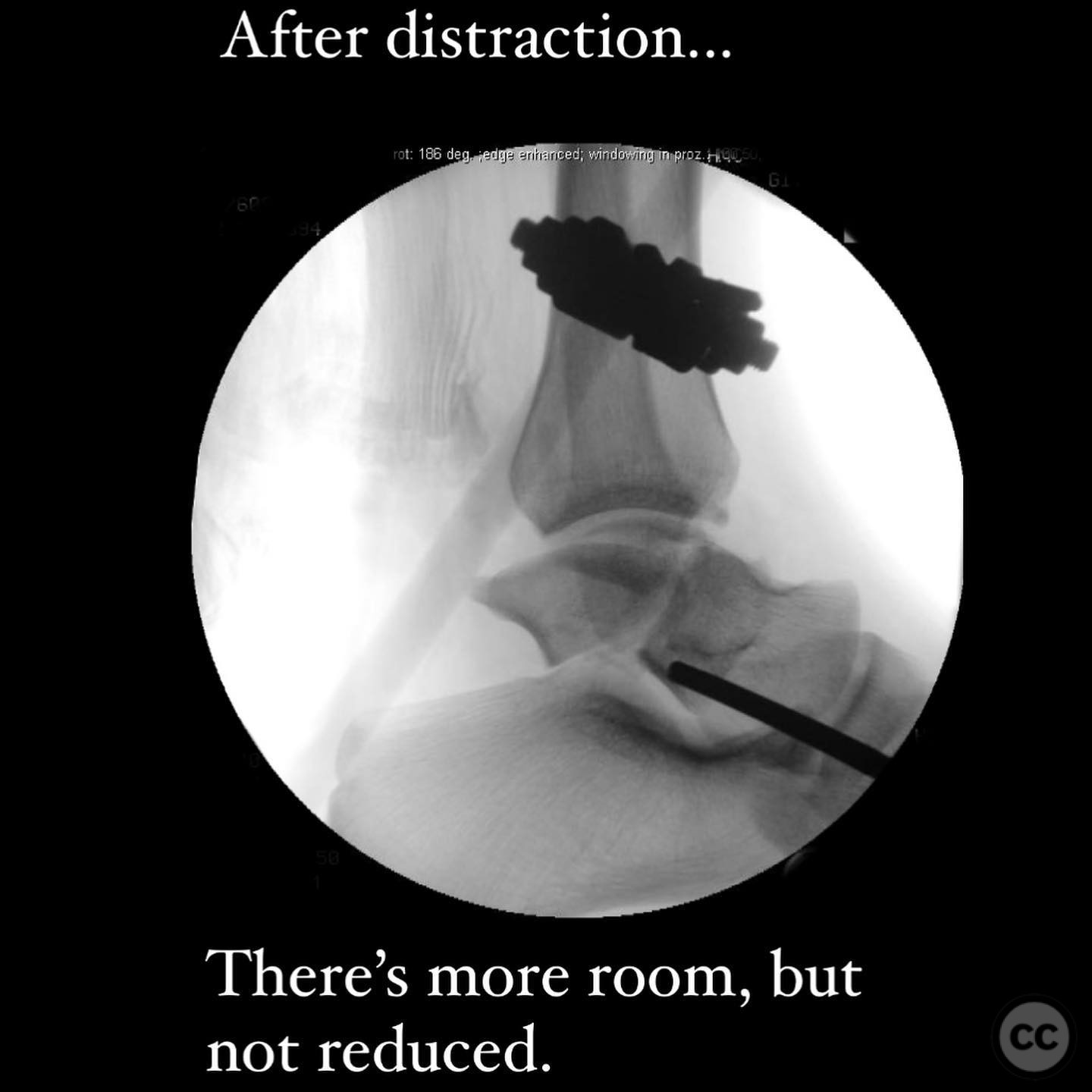
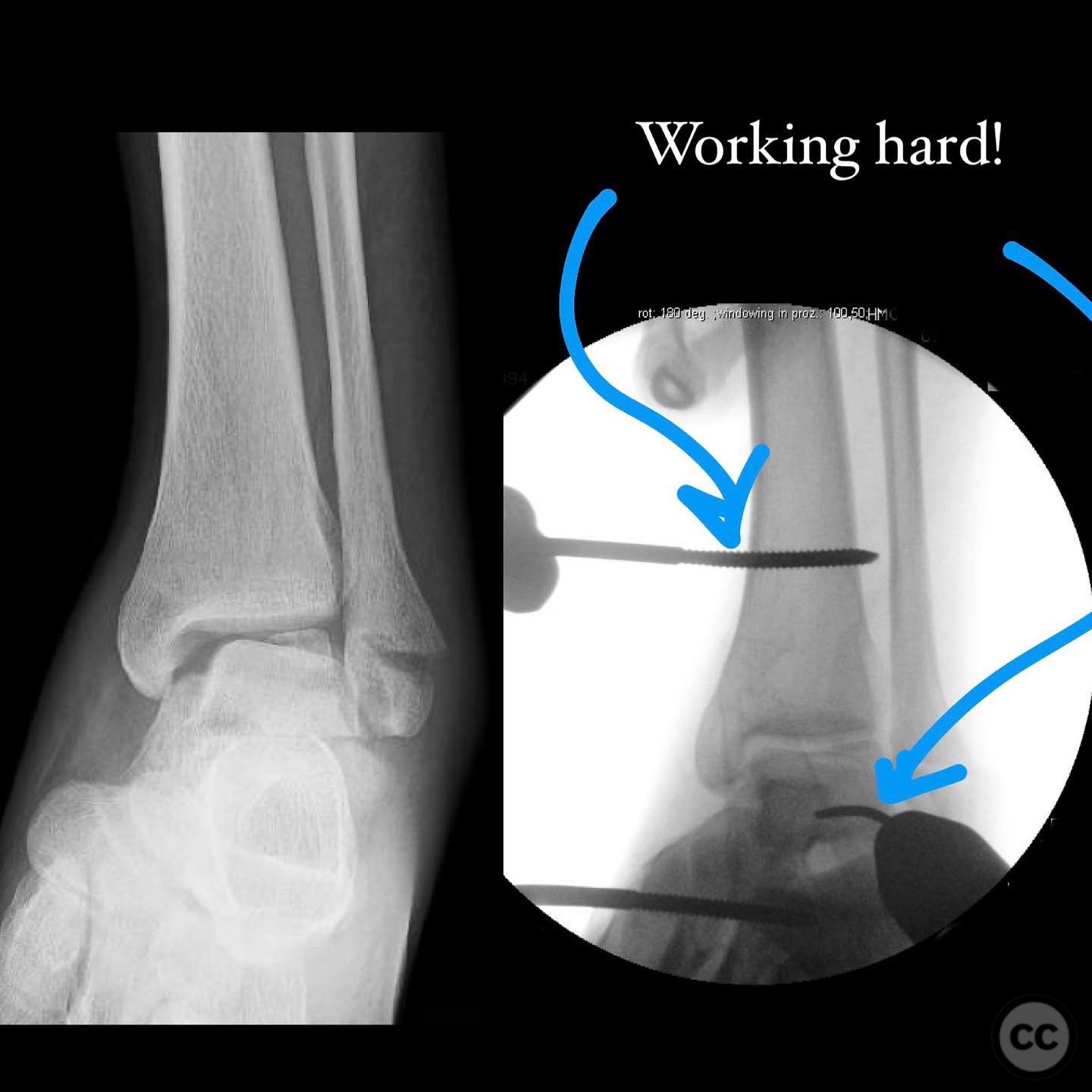
Clinical and radiological findings: A 22-year-old male sustained a closed talar body fracture dislocation following a fall while bouldering. The injury was characterized by significant swelling, with intact neurovascular status. The fracture involved a coronal plane separation of the talar body from the anterior plafond, with posterior dislocation and axial plane dome fragment involvement. There was medial subtalar impaction due to axial loading and supination. The fibula exhibited a tension failure fracture.
Preoperative Plan
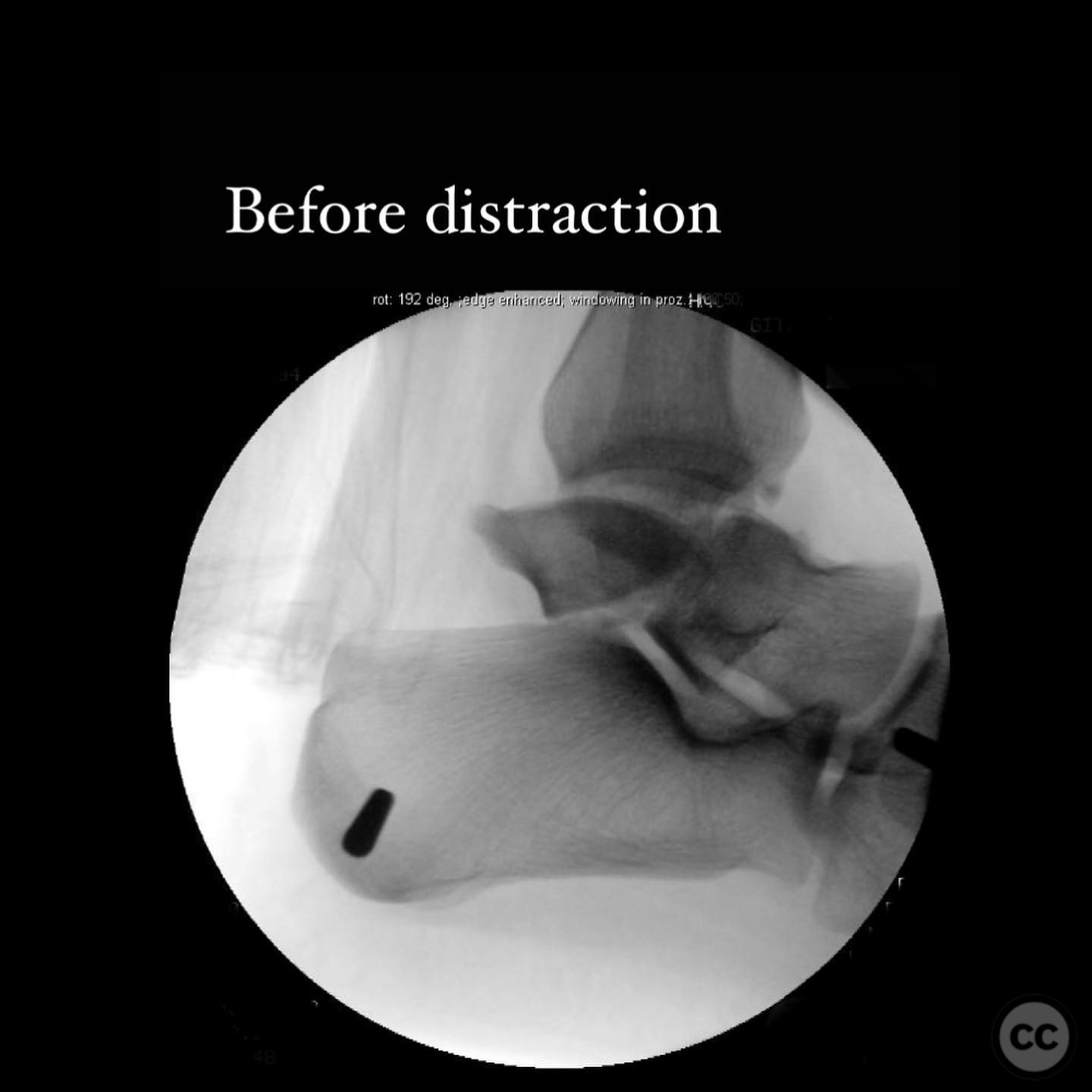
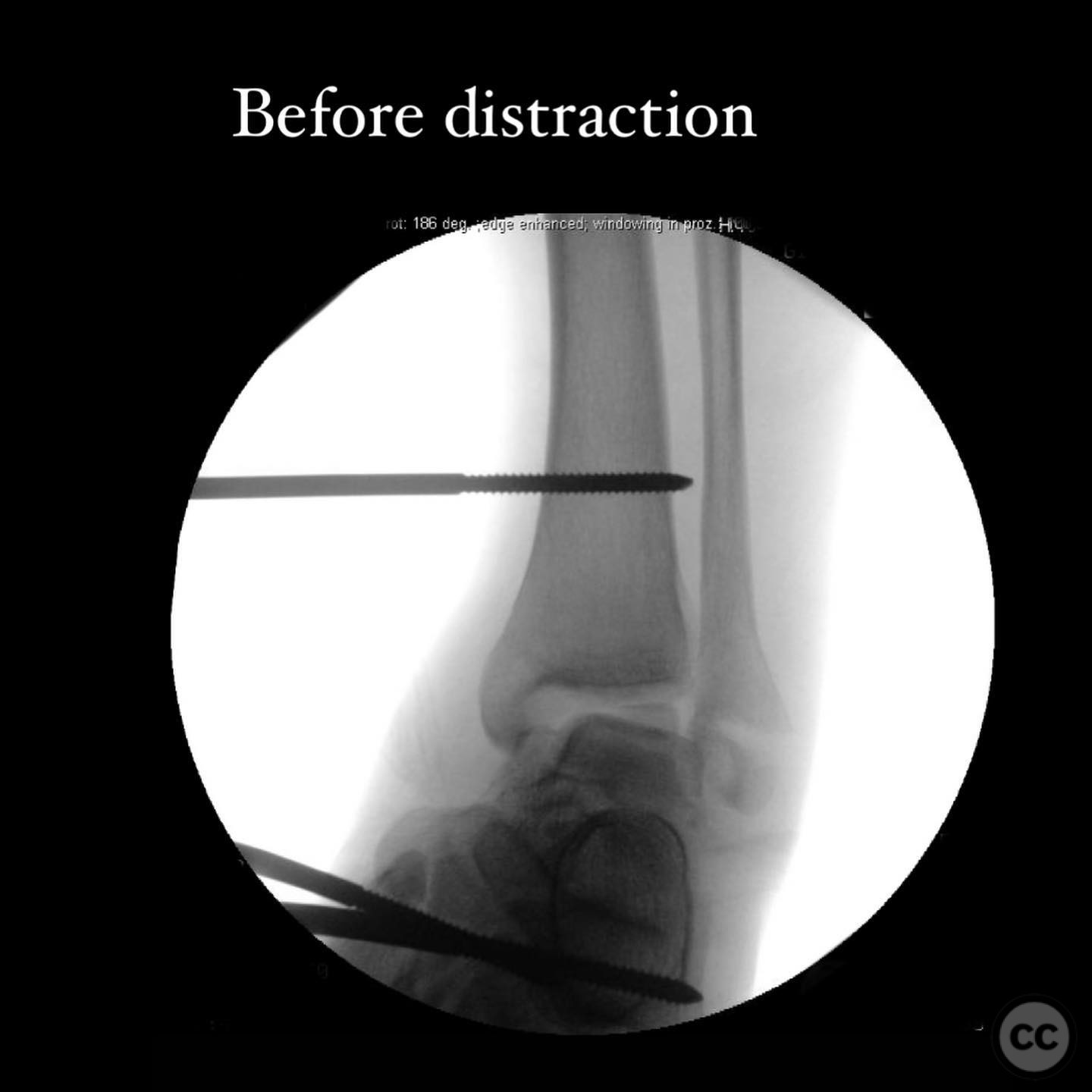
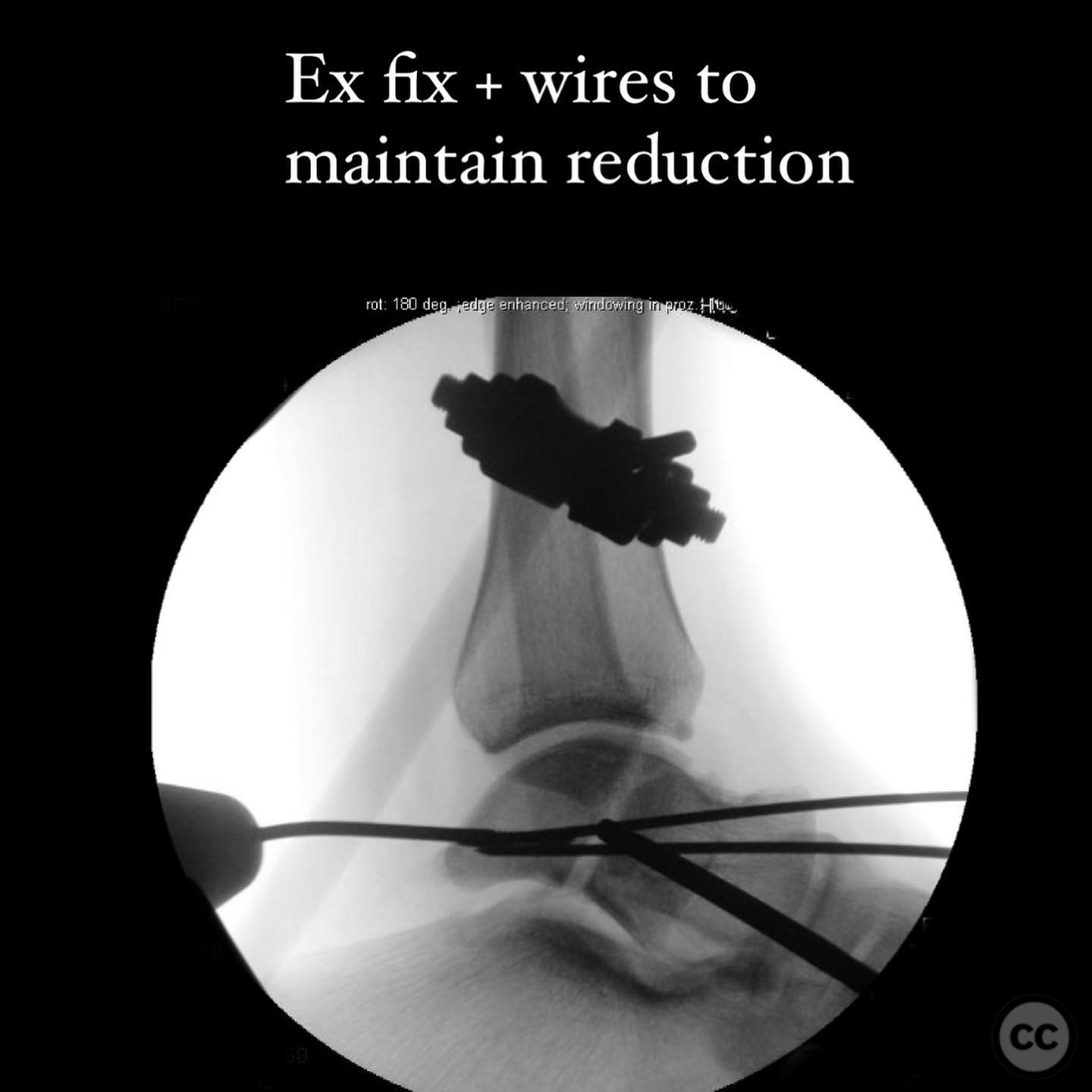
Planning remarks: The preoperative plan involved urgent reduction of the dislocated talus, followed by stabilization using a medial external fixation and controlled distraction. A percutaneous Schanz pin was used for manipulative reduction, with 2mm wires maintaining the reduction. Definitive surgical management was planned via anteromedial and anterolateral approaches, necessitating a medial malleolus osteotomy for optimal visualization and reduction of the dome fragment.
Surgical Discussion
Patient positioning: Supine positioning with the foot in plantarflexion to facilitate anterior surgical access.
Anatomical surgical approach: Anteromedial and anterolateral approaches were utilized for direct visualization of the talar body fracture. A medial malleolus osteotomy was performed to improve access to the dome fragment. The fibula fracture was addressed with a tension band plate, and bioabsorbable darts were used to secure the thin dome fragment.
Operative remarks:The surgeon noted that the medial malleolus osteotomy significantly aided in manipulating and reducing the fracture, which was otherwise challenging due to the location of the dome fragment. The fibula fracture did not provide useful access due to its distal location and tension failure nature. Fixation was orthogonal to the main fracture line, and headless compression screws were deemed unnecessary.
Postoperative protocol: Postoperative rehabilitation included immobilization with external fixation maintained until soft tissue swelling resolved, followed by progressive weight-bearing as tolerated.
Follow up: Not specified.
Orthopaedic implants used: Bioabsorbable darts, tension band plate, 2mm wires, 2.5mm Schanz pin.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 309 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Talar Body Fracture Dislocation with Medial Malleolus Osteotomy. Journal of Orthopaedic Surgery and Traumatology. Case Report 710174 Published Online Jul 14 2025.