

Infected Pseudoarthrosis of Tibia and Fibula Managed with Sequential Surgical Interventions
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: The patient presented with an open fracture of the tibia and fibula, which evolved poorly into an infected pseudoarthrosis with osteomyelitis. Initial radiological evaluation confirmed the presence of non-union and infection. The AO/OTA classification for the initial fracture is likely 42-C3, indicating a complex multifragmentary fracture of both the tibia and fibula.
Preoperative Plan
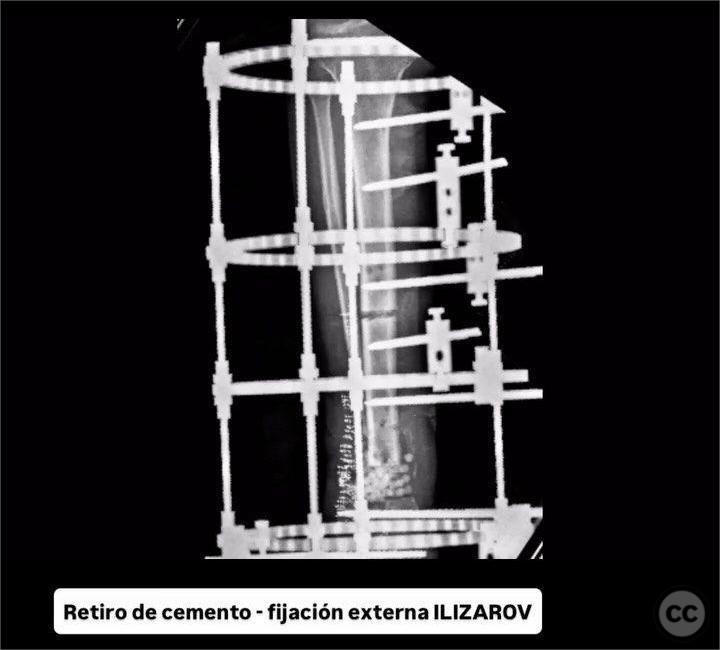
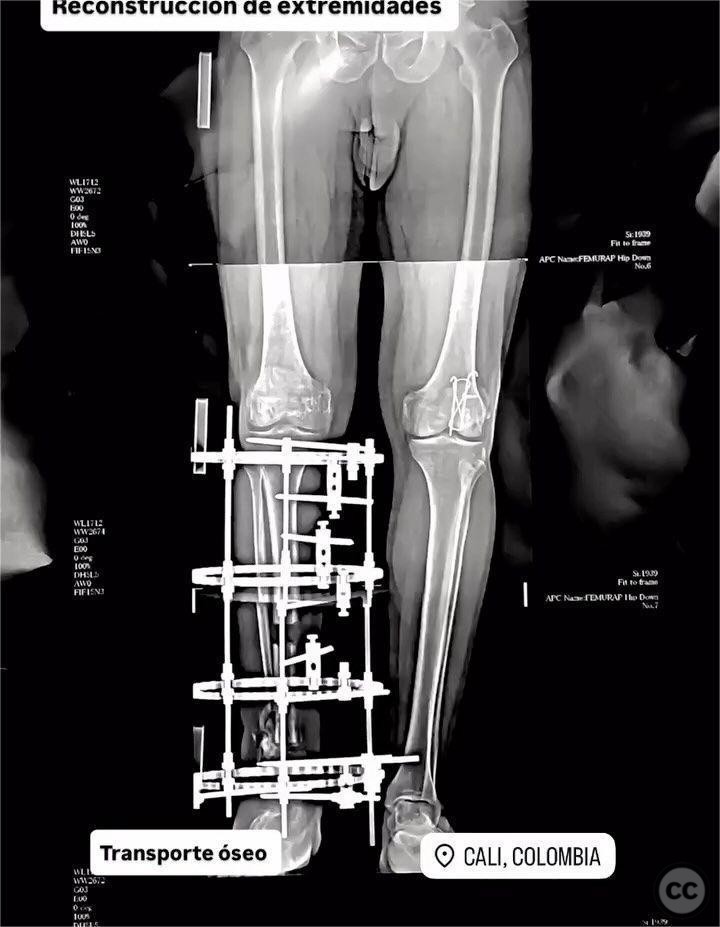
Planning remarks: The preoperative plan involved removal of any existing hardware, radical debridement of infected bone tissue, and placement of a provisional bone cement spacer. An elevated protective scaffold was utilized, and cultures were collected to guide antibiotic therapy. Following infection control, a bone substitute would be applied, and Ilizarov external fixation would be used for bone transport.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table to facilitate access to the tibial and fibular regions for debridement and subsequent procedures.
Anatomical surgical approach: A longitudinal incision was made over the anteromedial aspect of the tibia, extending from the proximal to distal third, allowing for exposure of both the tibia and fibula. Radical debridement was performed to excise all necrotic and infected tissue. A provisional bone cement spacer was placed within the defect, and an elevated protective scaffold was constructed to maintain limb length and alignment.
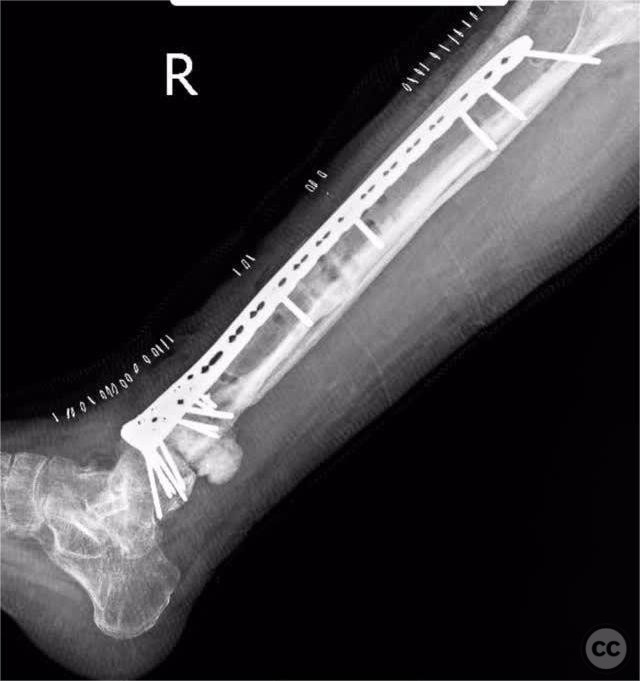
Operative remarks:The surgeon noted the extensive nature of the infection, necessitating thorough debridement to achieve a clean surgical field. Culture-guided antibiotic treatment was initiated postoperatively. After initial stabilization with a bone cement spacer, a bone substitute was applied, and an Ilizarov external fixator was used to facilitate bone transport at a rate of 1 mm per day. Walking training was incorporated into the rehabilitation protocol. Subsequently, conversion from external to internal fixation was achieved using a minimally invasive variable-angle distal tibial plate augmented with morphogenetic protein to promote osteogenesis.
Postoperative protocol: The postoperative rehabilitation protocol included immediate weight-bearing as tolerated with the Ilizarov frame in place, followed by progressive walking training. After conversion to internal fixation, weight-bearing was continued as tolerated, with emphasis on range of motion exercises and strengthening.
Follow up: Not specified.
Orthopaedic implants used: Ilizarov external fixator, variable-angle distal tibial plate, bone cement spacer, bone substitute, morphogenetic protein.
Search for Related Literature

Jhon Perez Casado
- Colombia , Cali - Valle del Cauca
- Area of Specialty - Lower Limb
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 739 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Perez Casado, J.J.. (2025). Infected Pseudoarthrosis of Tibia and Fibula Managed with Sequential Surgical Interventions. Journal of Orthopaedic Surgery and Traumatology. Case Report 6679914 Published Online Jul 21 2025.