




Percutaneous Screw Fixation of AO/OTA 61-B2 Fragility Pelvic Ring Injury in an Elderly Female
Score and Comment on this Case
Clinical Details
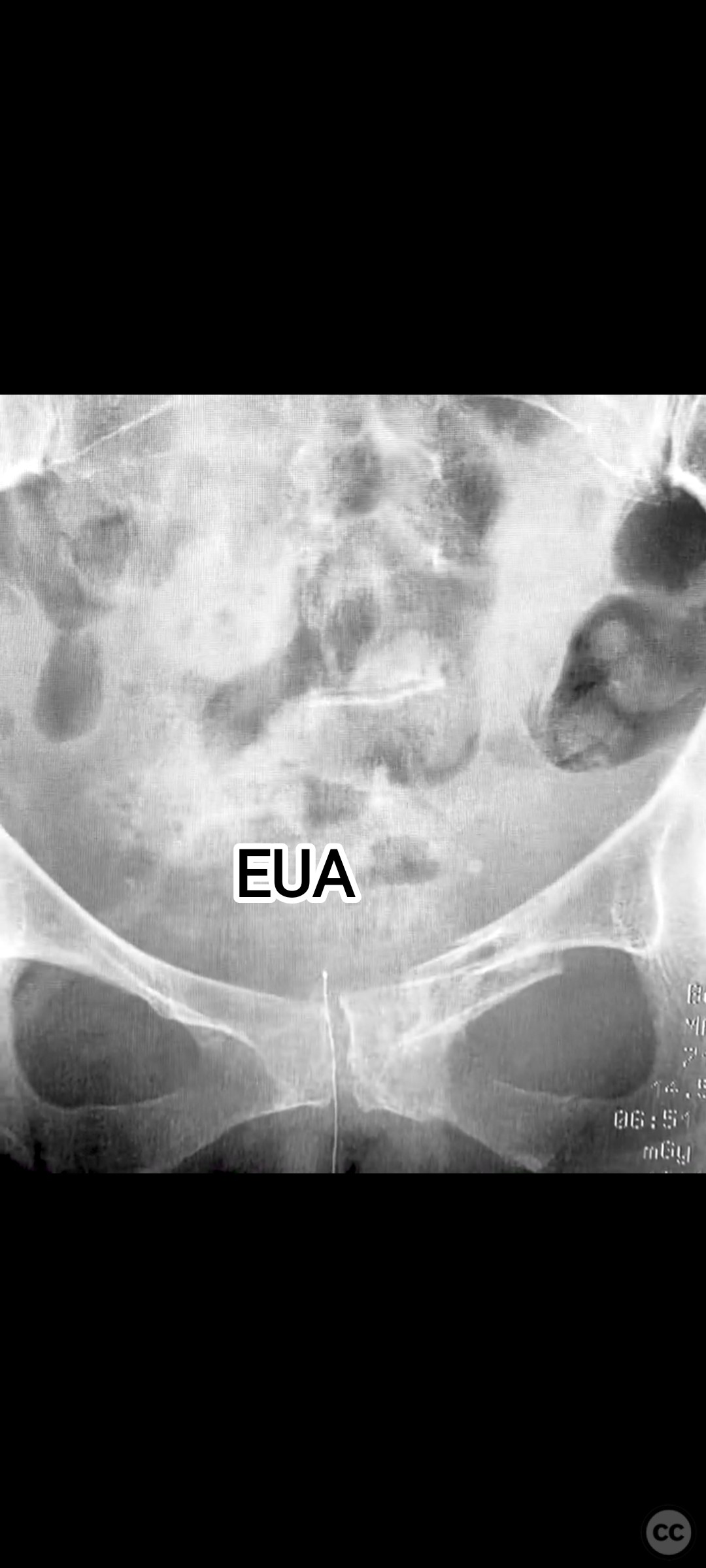
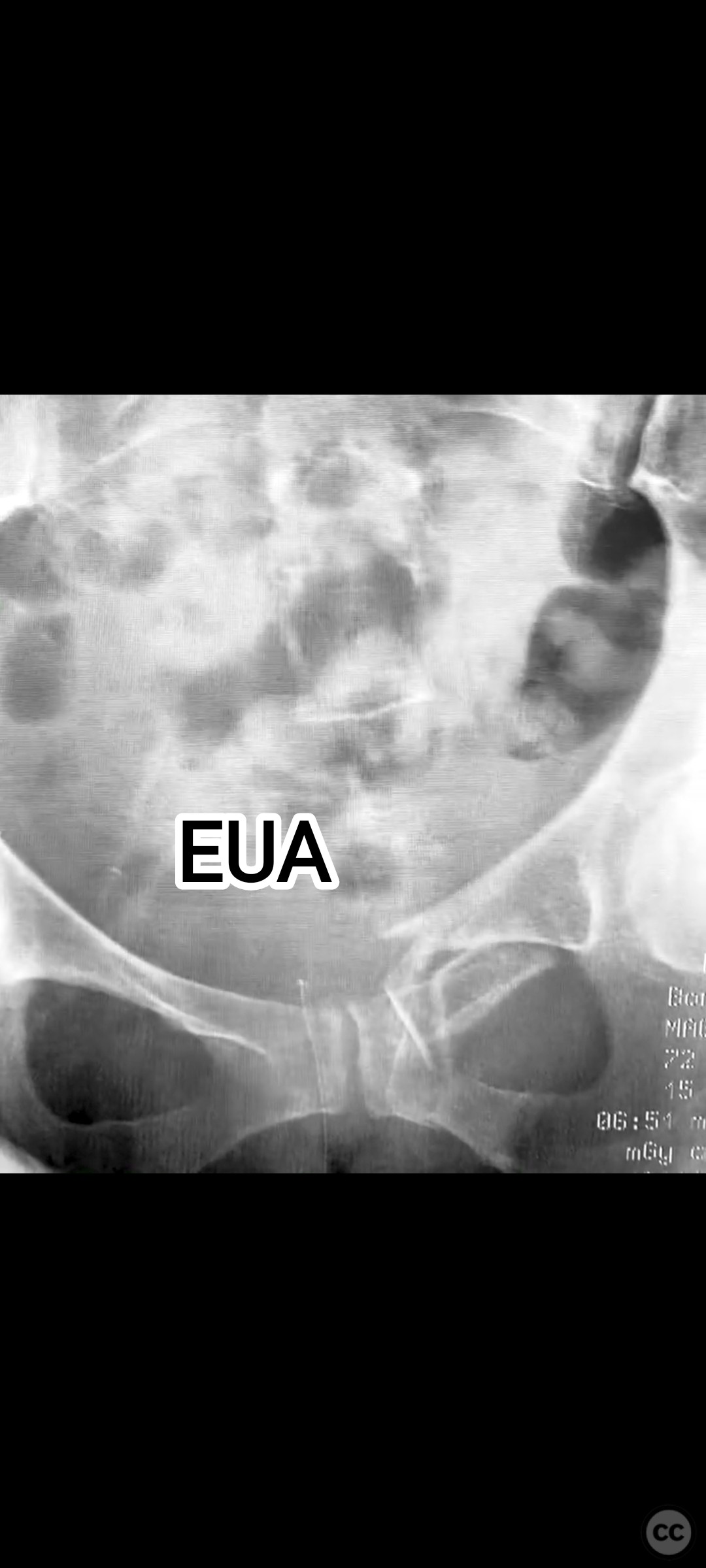
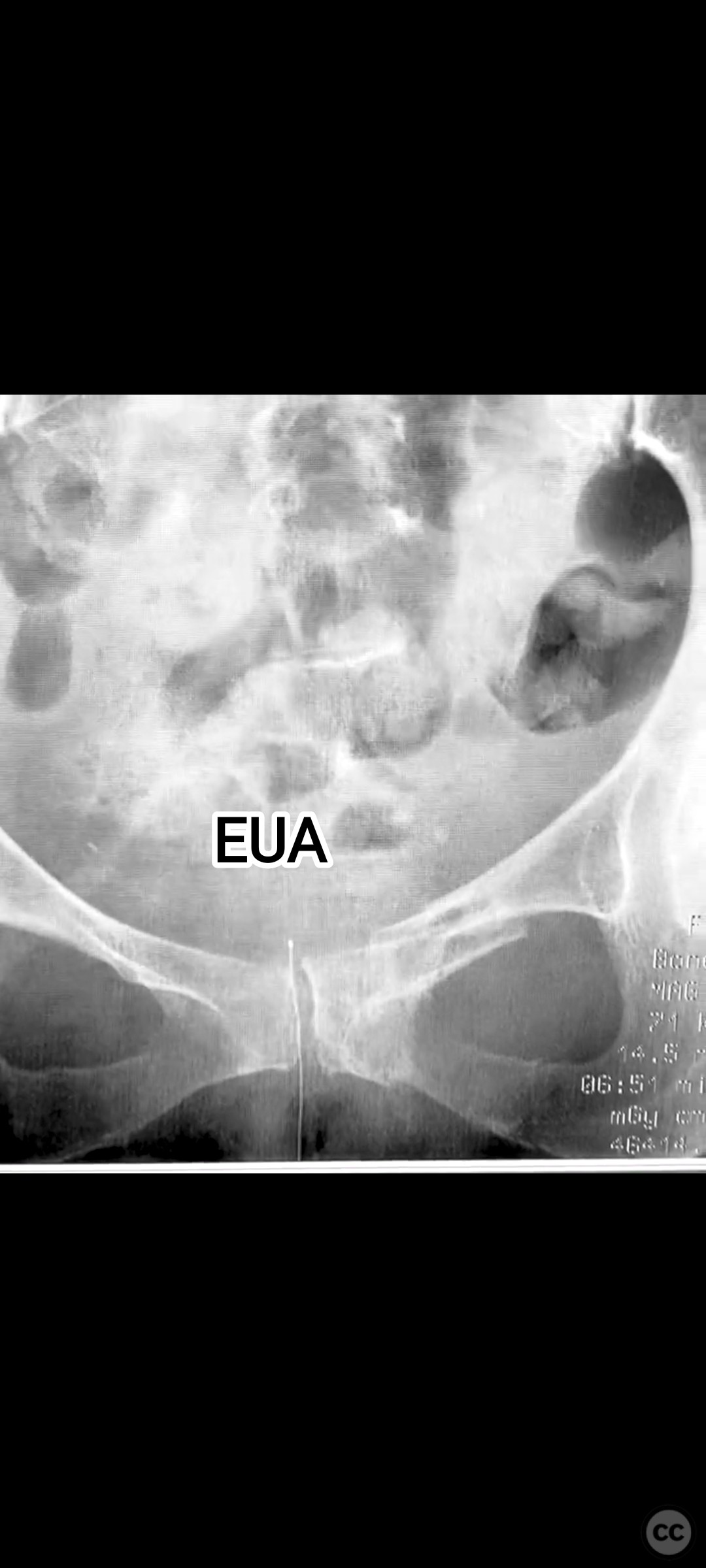
Clinical and radiological findings: A 74-year-old female presented following a fall from standing height, unable to mobilize due to severe pelvic pain (9/10). Examination under anesthesia with fluoroscopic assessment (AP and inlet views) demonstrated instability and displacement of the pelvic ring with minimal manual compression at the iliac crests. Imaging revealed left-sided posterior iliac/sacral and pubic ramus fractures consistent with an AO/OTA 61-B2 (lateral compression type) pelvic ring injury. No neurovascular deficits were noted.
Preoperative Plan
Planning remarks: The preoperative plan involved closed reduction of the pelvic ring under fluoroscopic guidance, followed by percutaneous screw fixation of the left posterior iliac/sacral region and the ipsilateral pubic ramus. Detailed preoperative CT imaging was used to plan safe osseous corridors for screw placement, correlating with intraoperative fluoroscopic landmarks.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table to facilitate unobstructed fluoroscopic imaging in AP, inlet, and outlet projections.
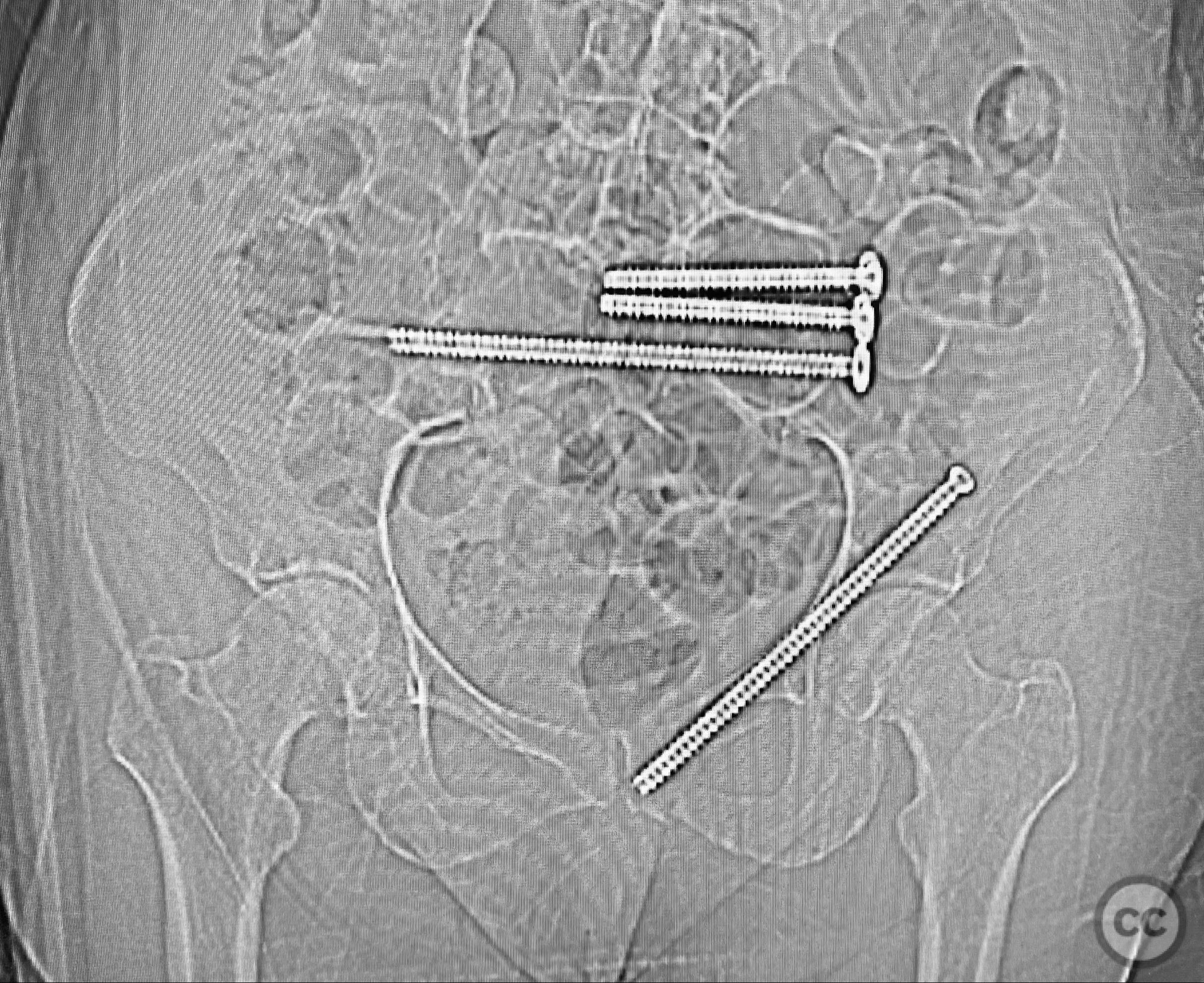
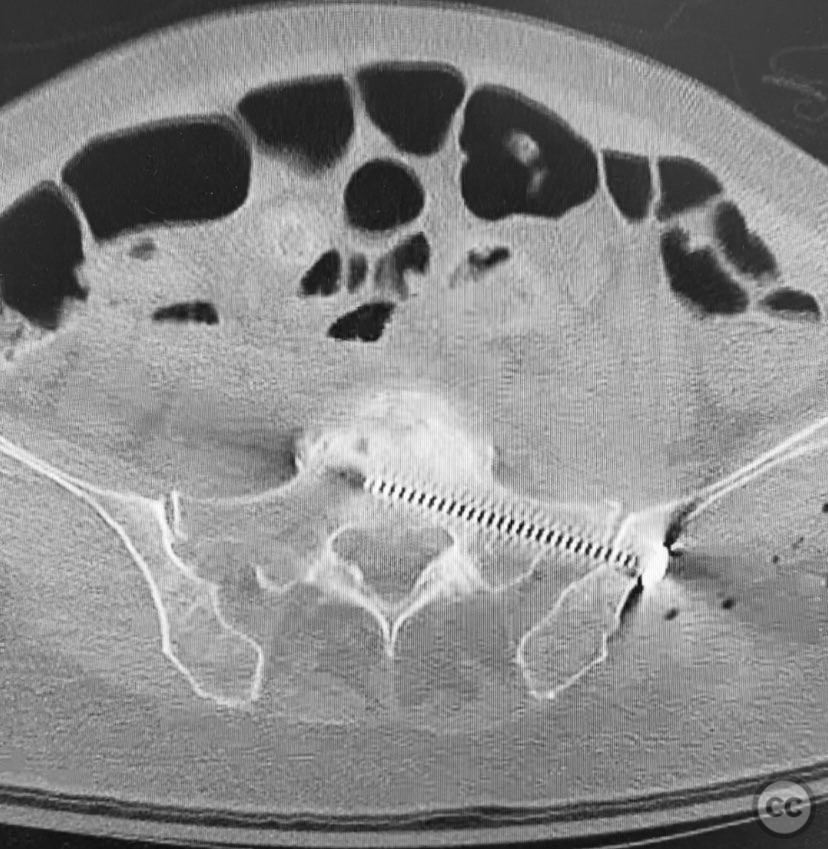
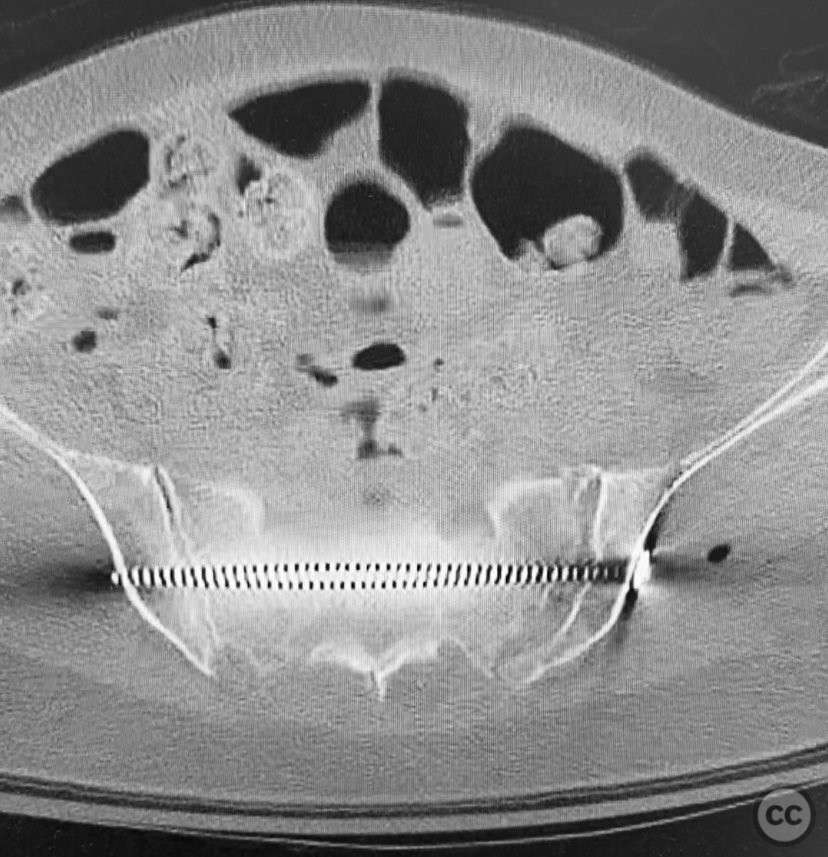
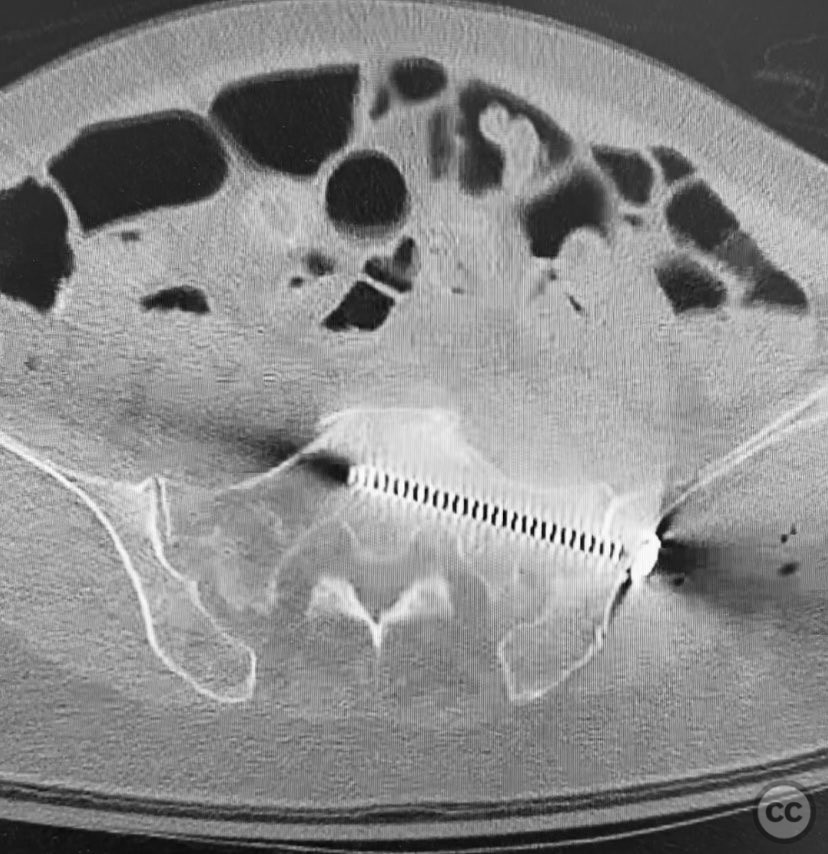
Anatomical surgical approach: Percutaneous technique was employed. Small stab incisions were made over the lateral aspect of the pelvis. Under continuous fluoroscopic guidance, guidewires were advanced through the ilium into the sacrum (iliosacral region) and through the superior pubic ramus. Cannulated screws were then inserted over the guidewires, ensuring extra-articular and intraosseous positioning within the safe bone corridors as determined by preoperative CT analysis.
Operative remarks:Intraoperatively, manual manipulation of the pelvis was performed to achieve improved reduction prior to fixation. The stability achieved by percutaneous screw fixation provided immediate symptomatic relief, allowing for early mobilization. The procedure emphasized meticulous attention to fluoroscopic imaging and preoperative CT planning to avoid neurovascular compromise and optimize screw trajectory within osteoporotic bone.
Postoperative protocol: Early mobilization with weight bearing as tolerated was initiated postoperatively, with physiotherapy focusing on transfer training and progressive ambulation. No external immobilization was used.
Follow up: Not specified
Orthopaedic implants used: Cannulated iliosacral screw, cannulated pubic ramus screw
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 329 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Percutaneous Screw Fixation of AO/OTA 61-B2 Fragility Pelvic Ring Injury in an Elderly Female. Journal of Orthopaedic Surgery and Traumatology. Case Report 6523869 Published Online Sep 12 2025.