

Type 2 Coronoid Base and Anteromedial Facet Fracture with LUCL Injury.
Score and Comment on this Case
Clinical Details
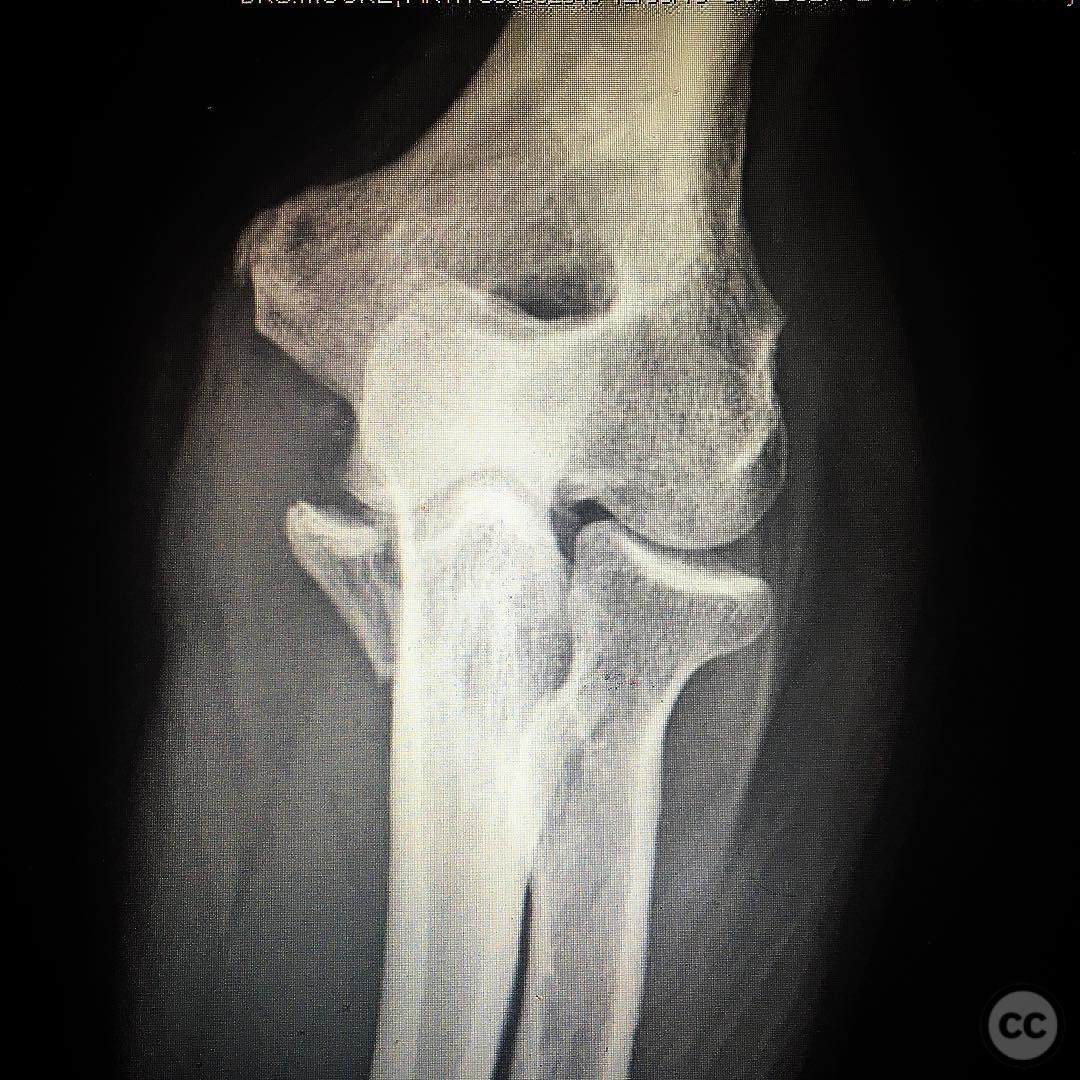
Clinical and radiological findings: A 36-year-old male presented following a fall while skateboarding, reporting a sensation of his elbow "popping out" and self-reduction. Initial radiographs and sagittal CT scans revealed a type 2 coronoid base fracture with an associated anteromedial facet fracture. This injury pattern is indicative of potential posteromedial rotatory instability, often accompanied by lateral ulnar collateral ligament (LUCL) injury. The coronal CT scan confirmed the involvement of the sublime tubercle, the insertion site of the ulnar collateral ligament, crucial for maintaining elbow stability.
Preoperative Plan
Planning remarks: The preoperative plan involved a midline posterior incision to access both medial and lateral aspects of the elbow. The surgical approach aimed to reduce and fix the coronoid base and sublime tubercle fractures using the Hotchkiss "over the top" technique. Repair of the LUCL was planned using #5 Fiberwire through bone tunnels in the lateral epicondyle.
Surgical Discussion
Patient positioning: The patient was positioned prone on the operating table to facilitate a posterior approach to the elbow.
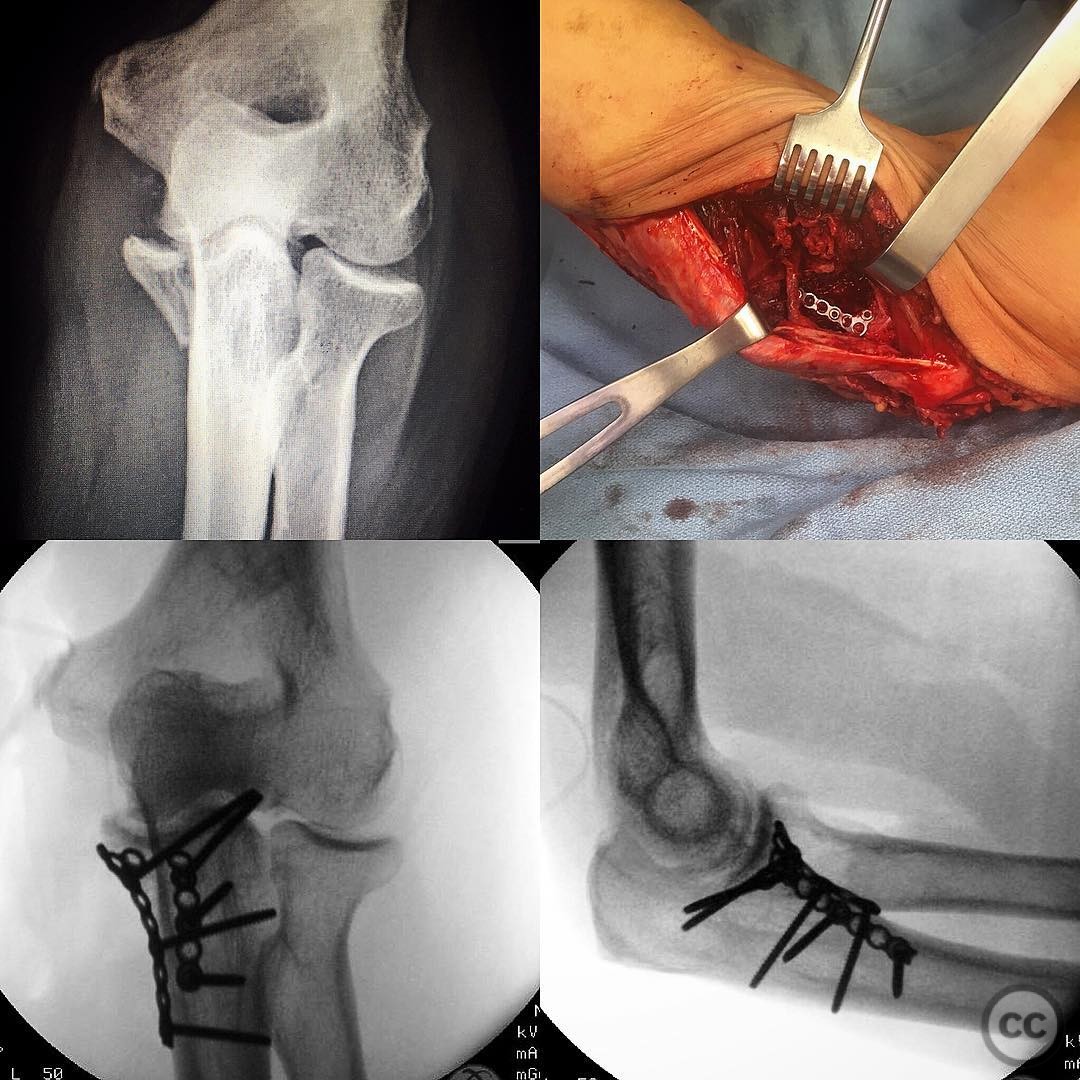
Anatomical surgical approach: A standard midline posterior approach was employed, involving an incision through the triceps fascia, olecranon, and subcutaneous border of the ulna. A large subcutaneous flap was raised medially, followed by complete neurolysis of the ulnar nerve from the triceps into the two heads of the flexor carpi ulnaris (FCU). The fascia overlying the flexor pronator mass was incised, and the natural raphe was bluntly dissected to reach the proximal anteromedial ulna. Care was taken to preserve crossing branches of the ulnar motor nerve. The midline approach allowed for lateral subcutaneous flap elevation to access Kaplan or Kocher intervals for LUCL or radial head intervention as needed.
Operative remarks:Intraoperatively, both the coronoid base fracture and sublime tubercle fracture were successfully reduced and fixed. The LUCL was repaired using #5 Fiberwire through bone tunnels on the lateral epicondyle. The meticulous protection of the ulnar nerve and preservation of motor nerve branches were critical steps in preventing postoperative complications. The surgical team emphasized the importance of addressing this injury pattern to prevent posteromedial rotatory instability and subsequent joint arthrosis.
Postoperative protocol: Postoperatively, a structured rehabilitation protocol was initiated, focusing on early mobilization while protecting the repair. Initial immobilization in a hinged elbow brace was followed by gradual range of motion exercises, progressing to strengthening exercises as tolerated.
Follow up: Not specified.
Orthopaedic implants used: #5 Fiberwire for LUCL repair.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 302 times
05 Aug 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Type 2 Coronoid Base and Anteromedial Facet Fracture with LUCL Injury.. Journal of Orthopaedic Surgery and Traumatology. Case Report 6200167 Published Online Aug 05 2025.