










Ipsilateral Pertrochanteric and Distal Femoral Fractures with Knee Dislocation.
Score and Comment on this Case
Clinical Details
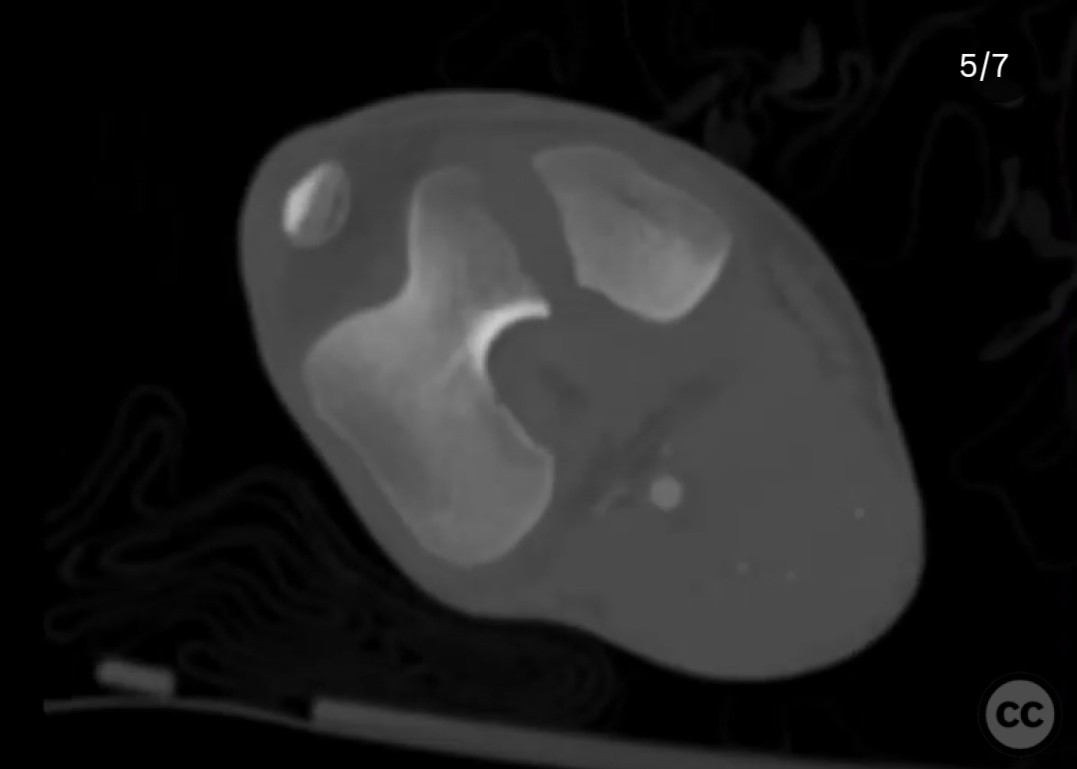
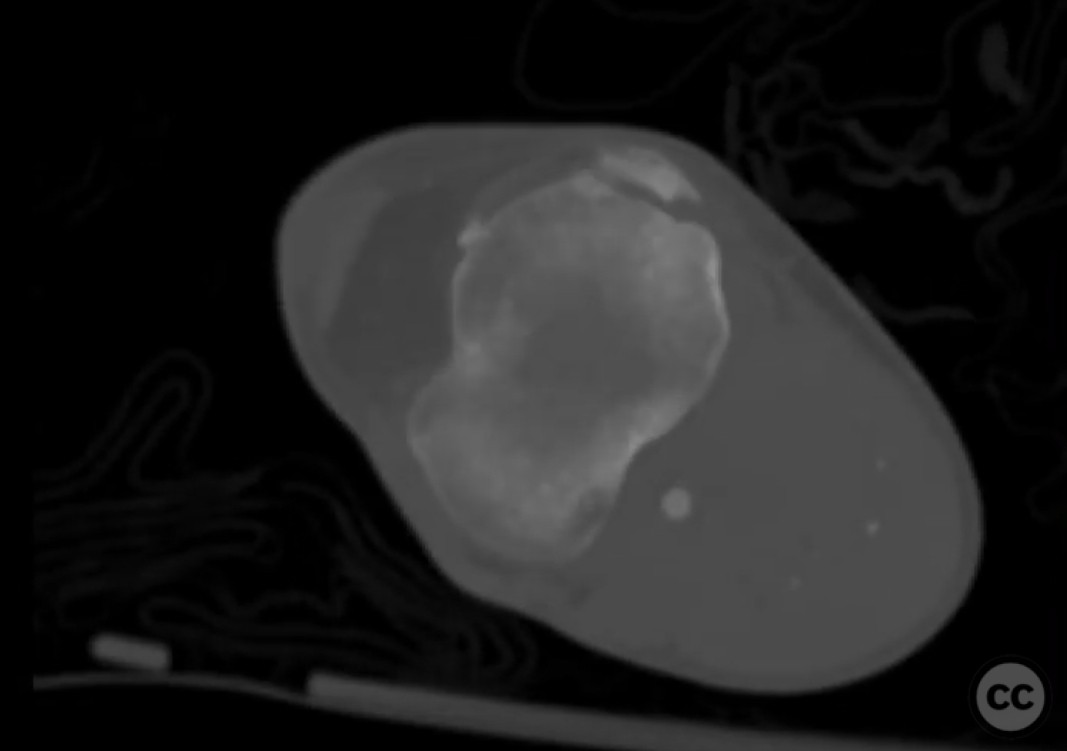
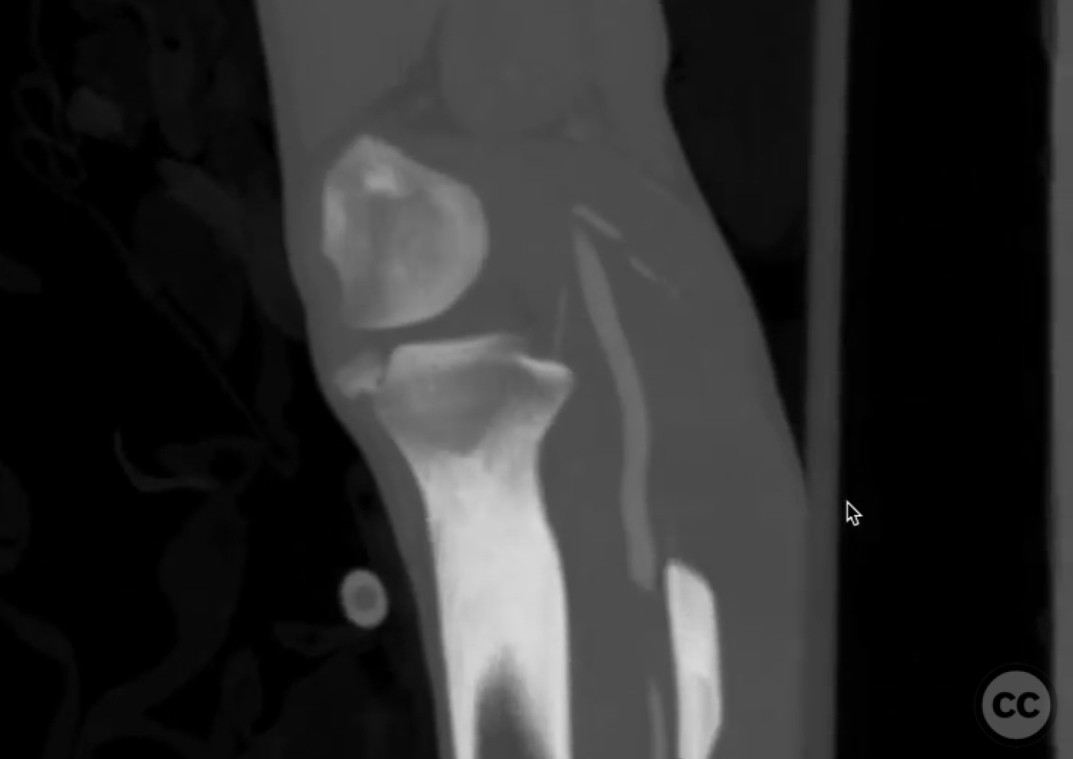
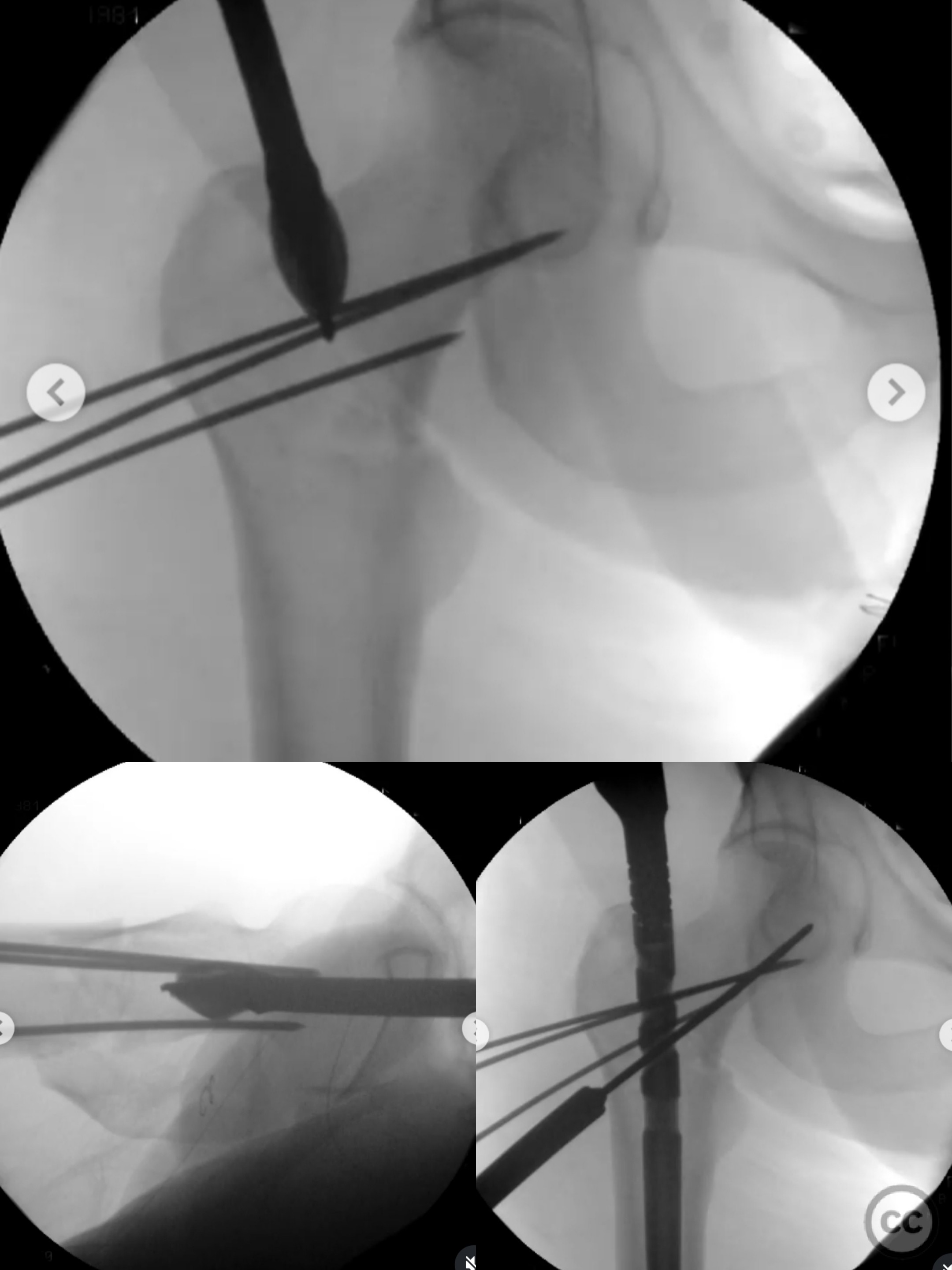
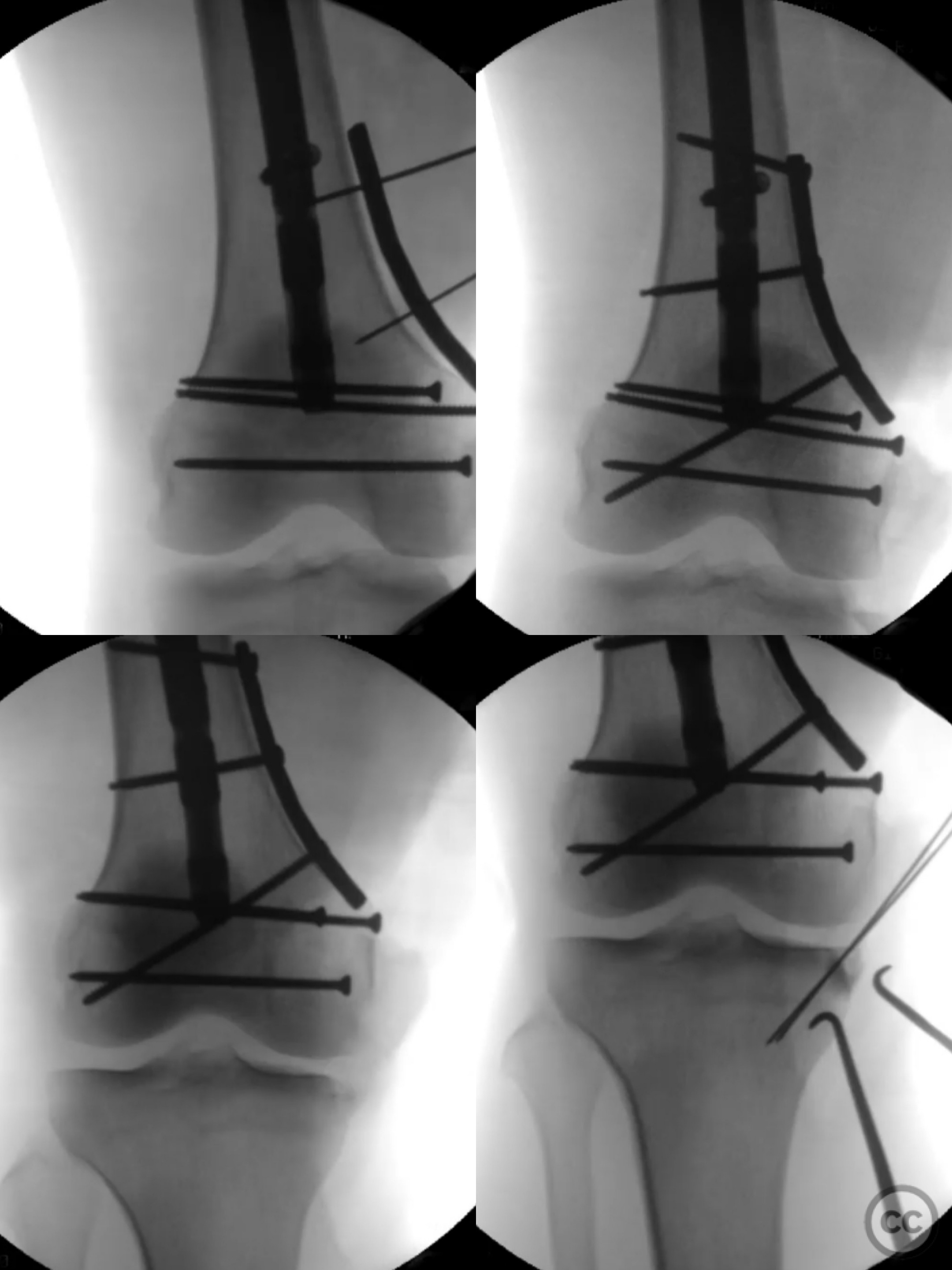
Clinical and radiological findings: A 32-year-old male sustained high-energy trauma from a motorcycle accident, resulting in an ipsilateral pertrochanteric femur fracture and a complex knee fracture dislocation. The knee injury included a medial femoral condyle fracture, medial tibial plateau rim fracture, tibial spine avulsion fractures, and lateral ligamentous injury. Initial imaging was not provided, but the description suggests significant bony and soft tissue involvement.
Preoperative Plan
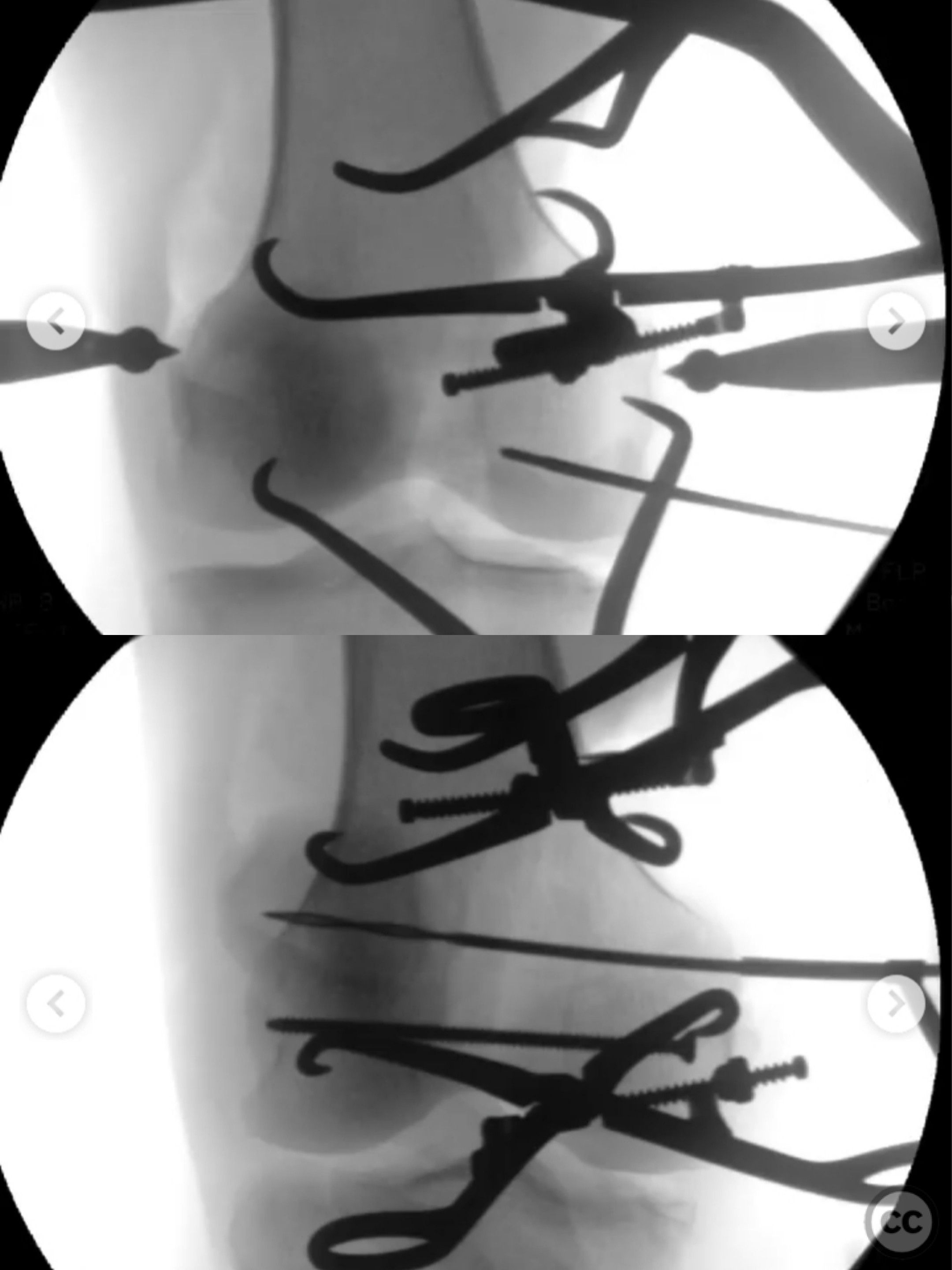
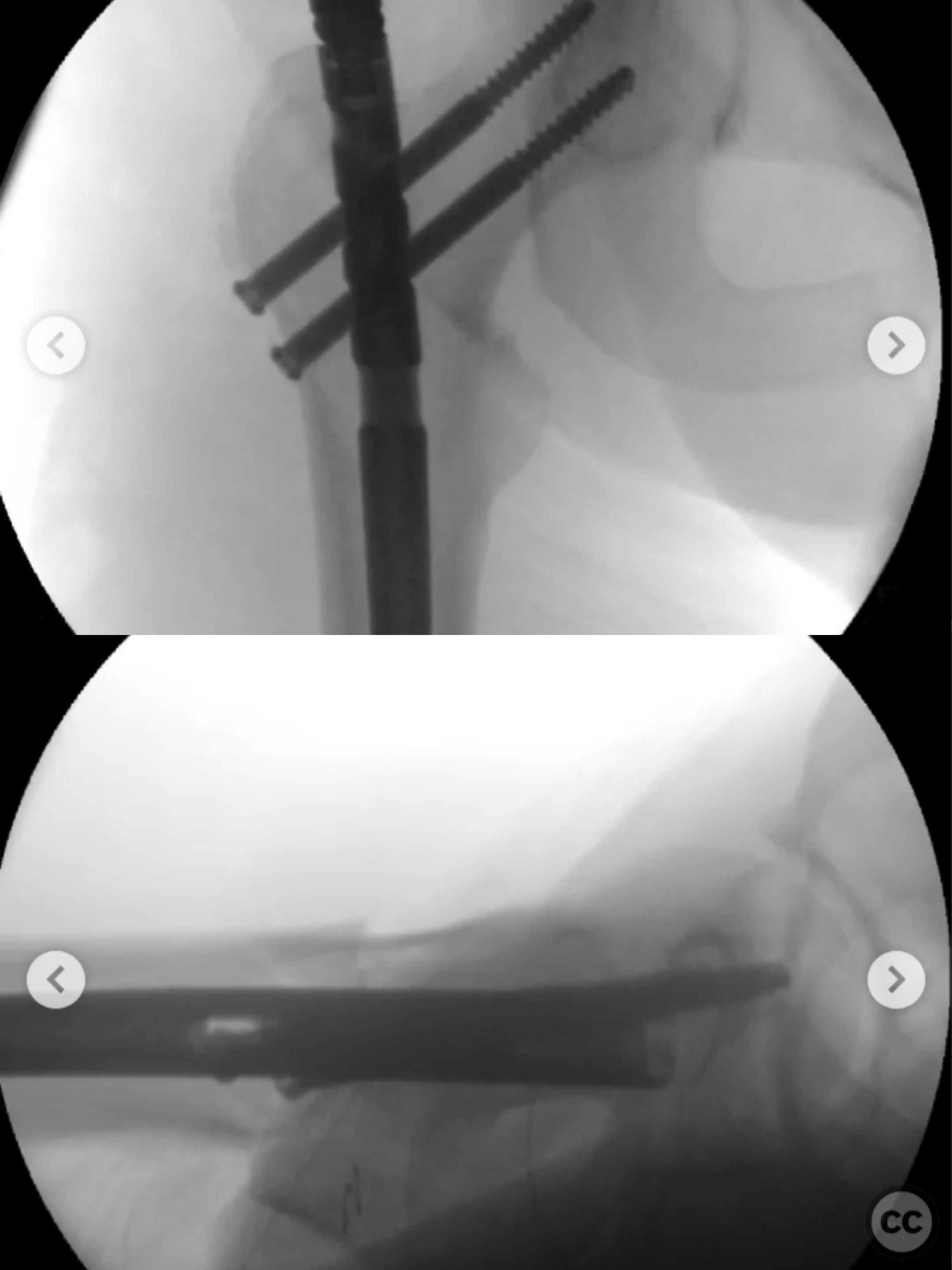
Planning remarks: The preoperative plan involved a medial subvastus approach to address the distal femoral fracture initially. A terminally threaded 2.5mm Schanz pin was used for sagittal plane control, followed by direct clamp reduction. Interfragmentary lag screws were placed anterior and posterior to the planned intramedullary nail path. Subsequent steps included distal femoral skeletal traction and percutaneous reduction for the pertrochanteric fracture, maintained with 2.4mm wires.
Surgical Discussion
Patient positioning: The patient was positioned supine for the procedure, allowing access to both the proximal and distal femur as well as the knee joint.
Anatomical surgical approach: A medial subvastus approach was utilized for the distal femoral fracture. This involved splitting the vastus medialis muscle to access the fracture site. A terminally threaded Schanz pin was placed in the condyle for control, followed by interfragmentary lag screw placement. Percutaneous techniques were employed for reduction of the pertrochanteric fracture, with subsequent reaming and nailing.
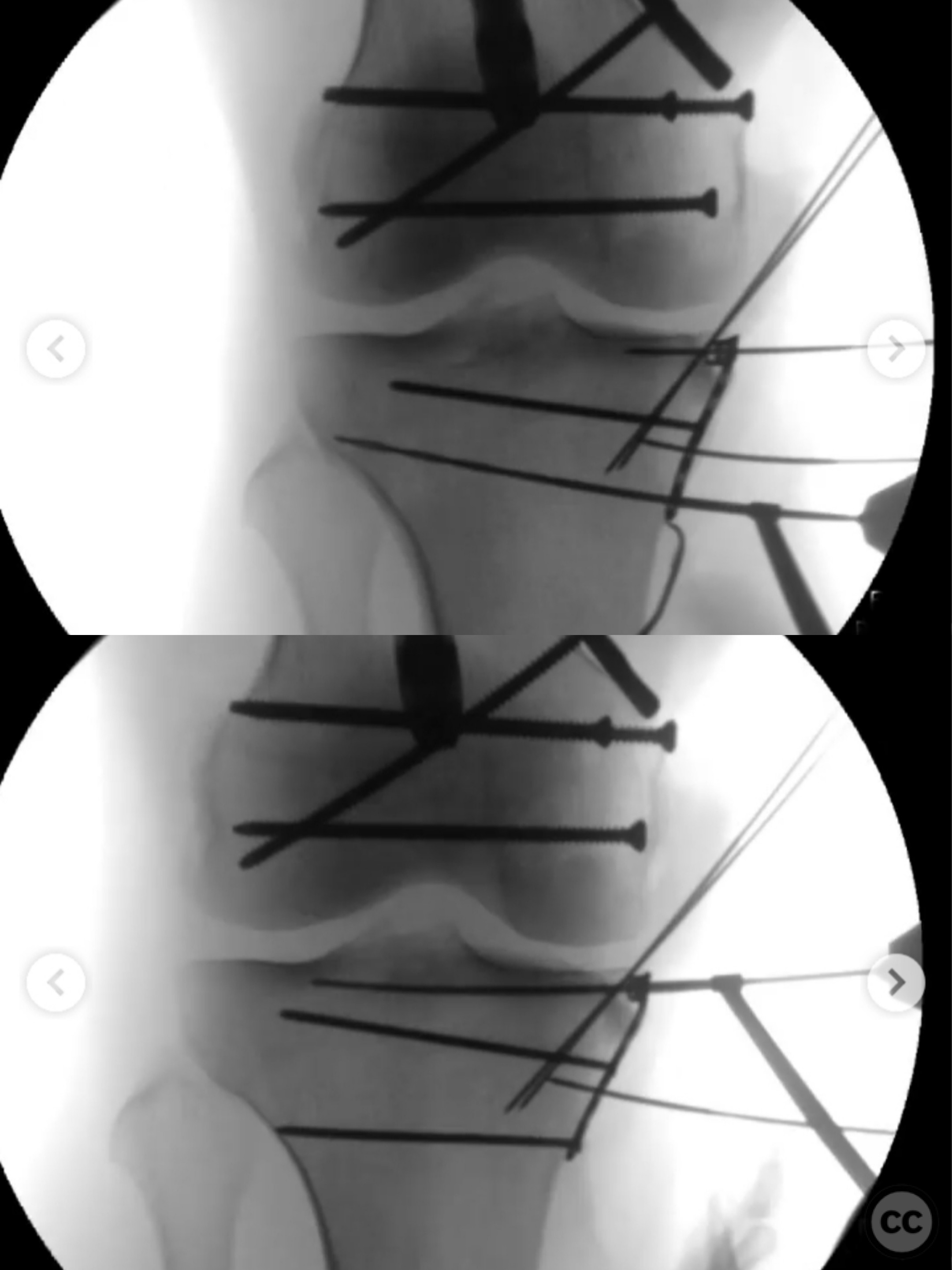
Operative remarks:The surgeon noted that maintaining reduction during nailing was critical, achieved through strategic placement of wires and clamps. After addressing the femoral fractures, attention was turned to the knee joint. The medial meniscus had an anterior root avulsion with the anterior half flipped under the rim fragment. Reduction of the meniscus and plateau fragment was performed through a small split in the anterior medial collateral ligament, supported with calcium phosphate (CaPO4) and buttressed. Despite some residual varus instability, it was anticipated that bracing would facilitate healing of the knee injuries.
Postoperative protocol: Postoperative rehabilitation included bracing to address residual varus instability of the knee. Specific weight-bearing instructions were not detailed.
Follow up: Not specified.
Orthopaedic implants used: Terminally threaded 2.5mm Schanz pin, interfragmentary lag screws, 2.4mm wires, intramedullary nail, buttress plate, calcium phosphate (CaPO4).
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 357 times
12 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Ipsilateral Pertrochanteric and Distal Femoral Fractures with Knee Dislocation.. Journal of Orthopaedic Surgery and Traumatology. Case Report 5786762 Published Online Jul 12 2025.