










Hawkins IV Talar Neck Fracture Dislocation with Insensate Tibial Nerve.
Score and Comment on this Case
Clinical Details
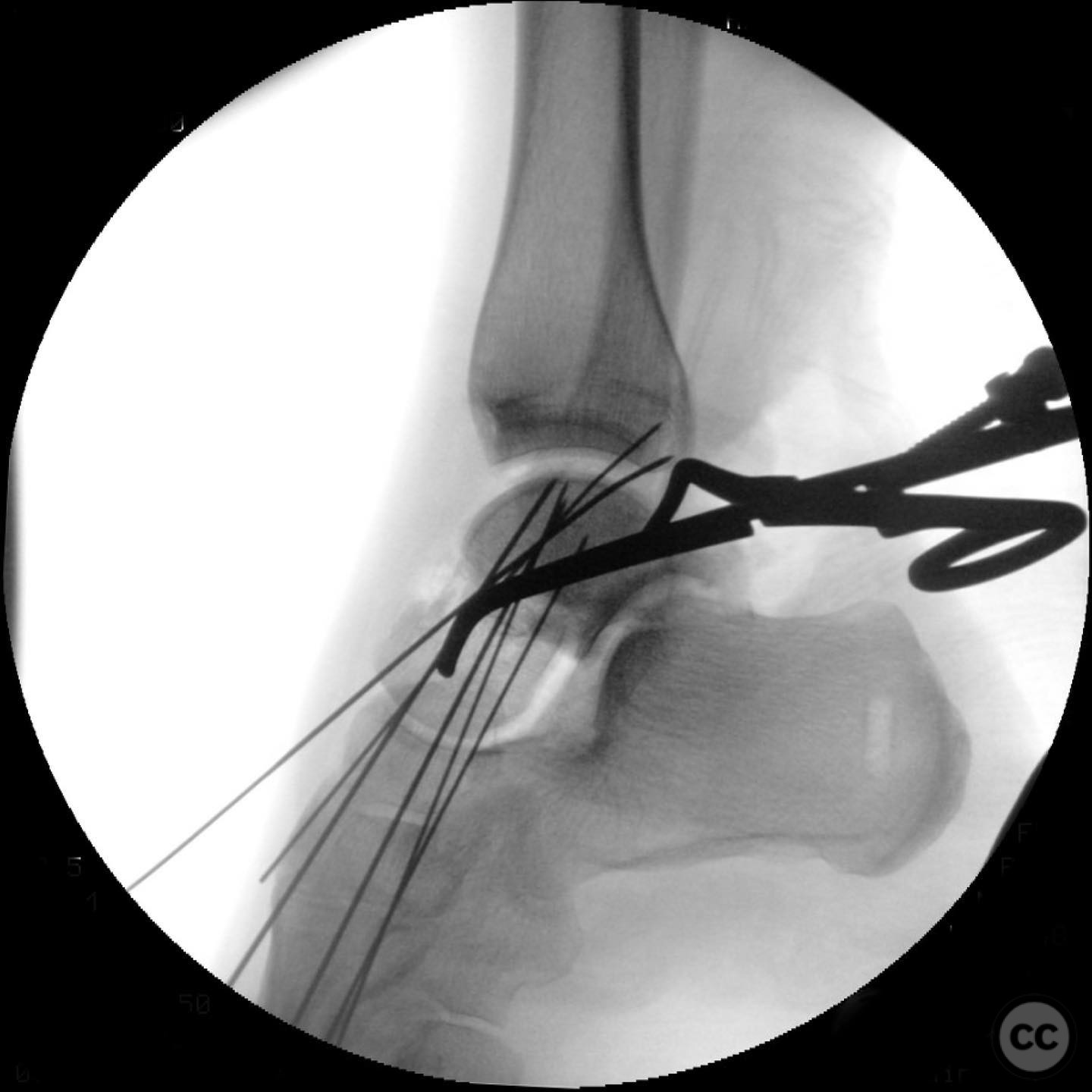
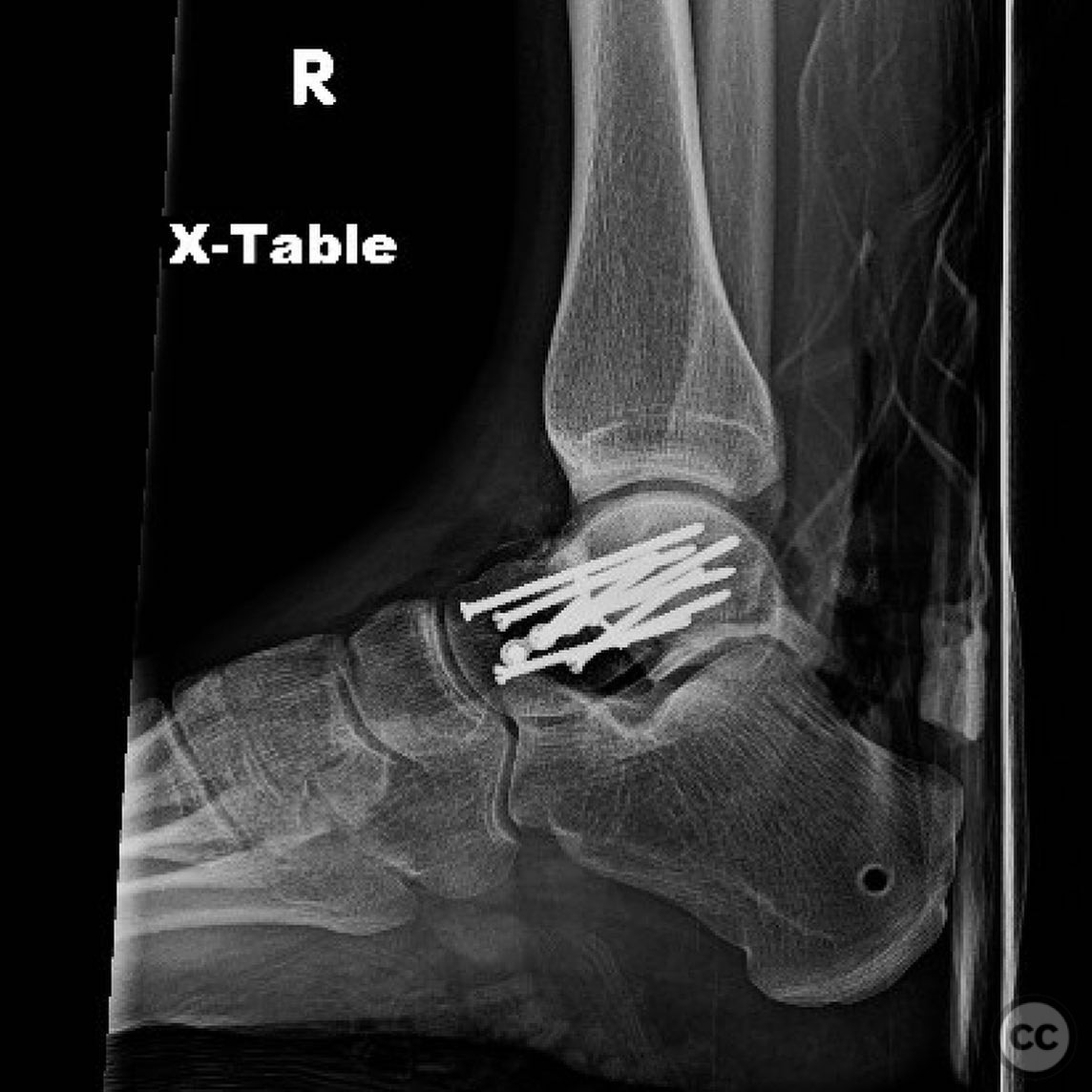
Clinical and radiological findings: A healthy rock climber presented with a closed talar neck fracture dislocation, classified as Hawkins IV, characterized by subtalar, tibiotalar, and talonavicular dislocations. The patient exhibited moderate swelling of the foot with minor medial hindfoot blistering and an insensate tibial nerve. The foot was well perfused. The injury was not reducible in the emergency department despite full paralysis and proper technique.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction due to the inability to achieve closed reduction, likely due to entrapped structures such as the posterior tibial tendon, flexor hallucis longus, flexor digitorum longus, tibial nerve, and artery. A preoperative CT scan was mandatory to guide the surgical approach.
Surgical Discussion
Patient positioning: The patient was positioned supine with the affected limb prepared for a posteromedial approach.
Anatomical surgical approach: A posteromedial approach was utilized to address the dislocated talar body and associated structures. This involved incision along the posteromedial aspect of the ankle, careful dissection to identify and protect neurovascular structures, and reduction of the talar body back into the capsule.
Operative remarks:The surgeon noted that an open reduction was necessary due to entrapped structures preventing closed reduction. An external fixator was applied to facilitate reduction and maintain stability while allowing for soft tissue recovery. The decision for single-stage treatment was based on acceptable soft tissue conditions and manageable fracture pattern complexity.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing for 6 weeks, followed by gradual weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: External fixator system.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 368 times
12 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Hawkins IV Talar Neck Fracture Dislocation with Insensate Tibial Nerve.. Journal of Orthopaedic Surgery and Traumatology. Case Report 5445282 Published Online Jul 12 2025.