 How did it f(.jpg)
 How did it _1.jpg)
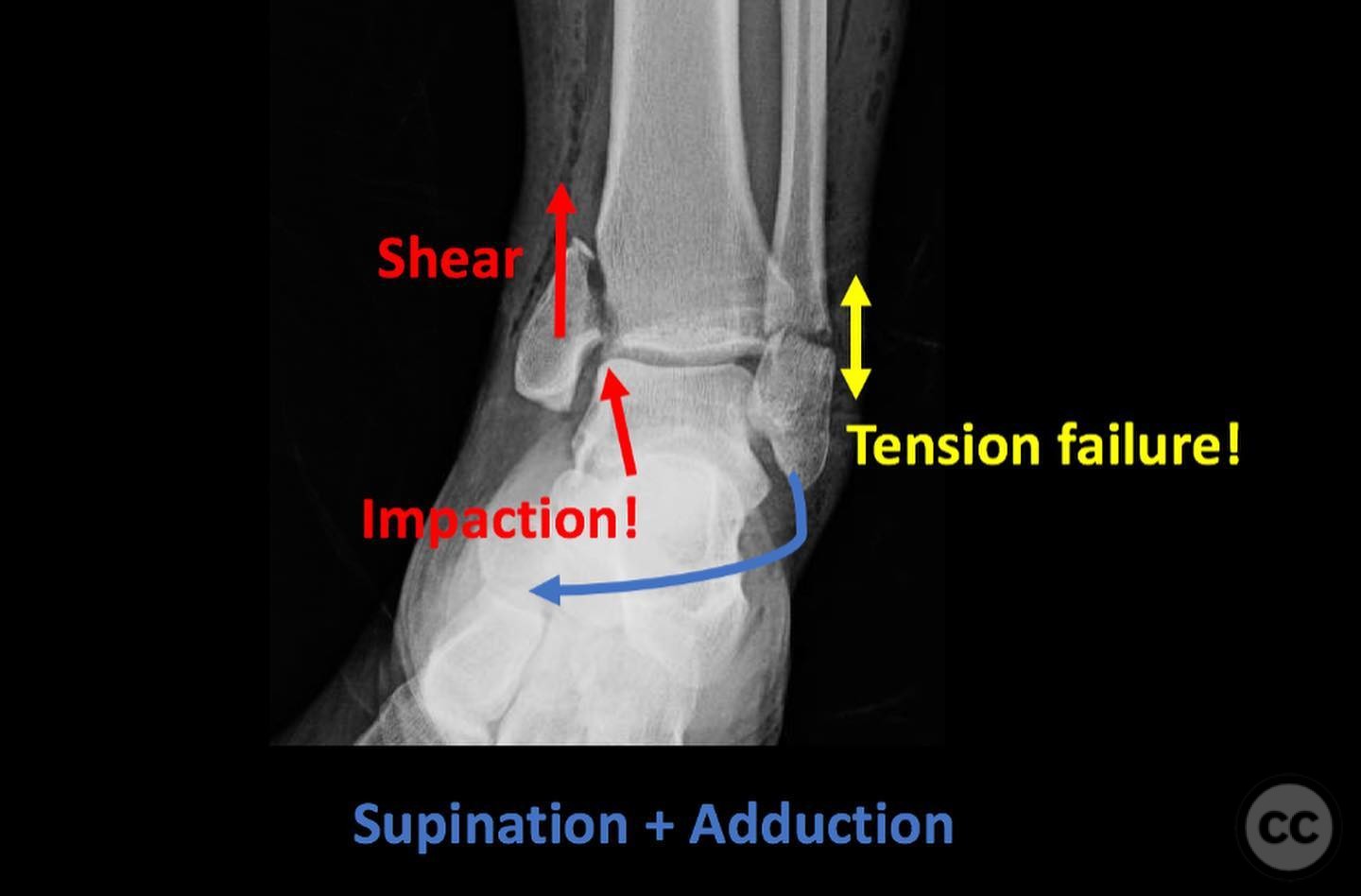
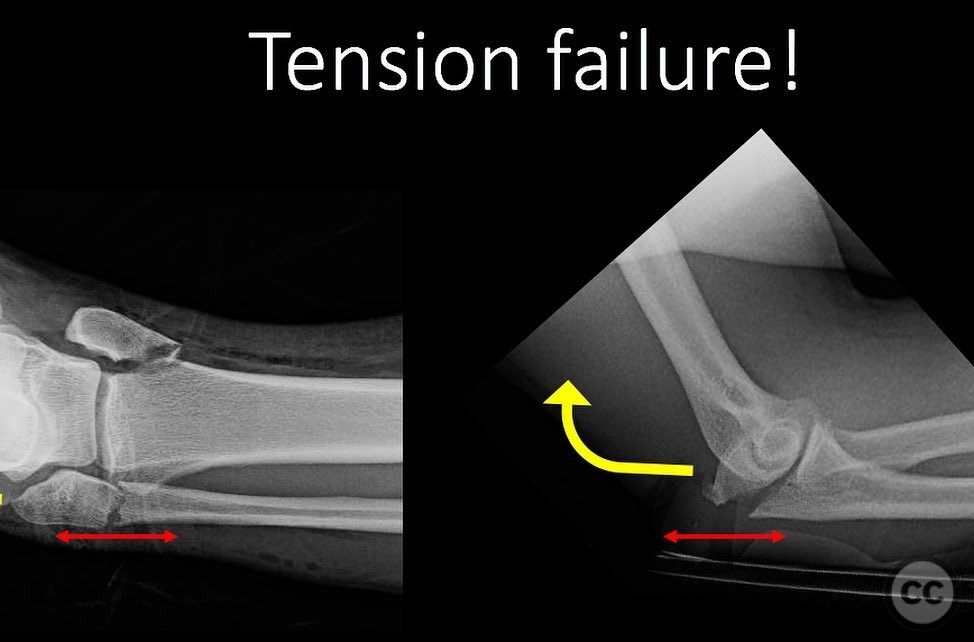

Supination-Adduction Ankle Fracture: Fix the Mechanism, Not Just the Bone
Score and Comment on this Case
Clinical Details
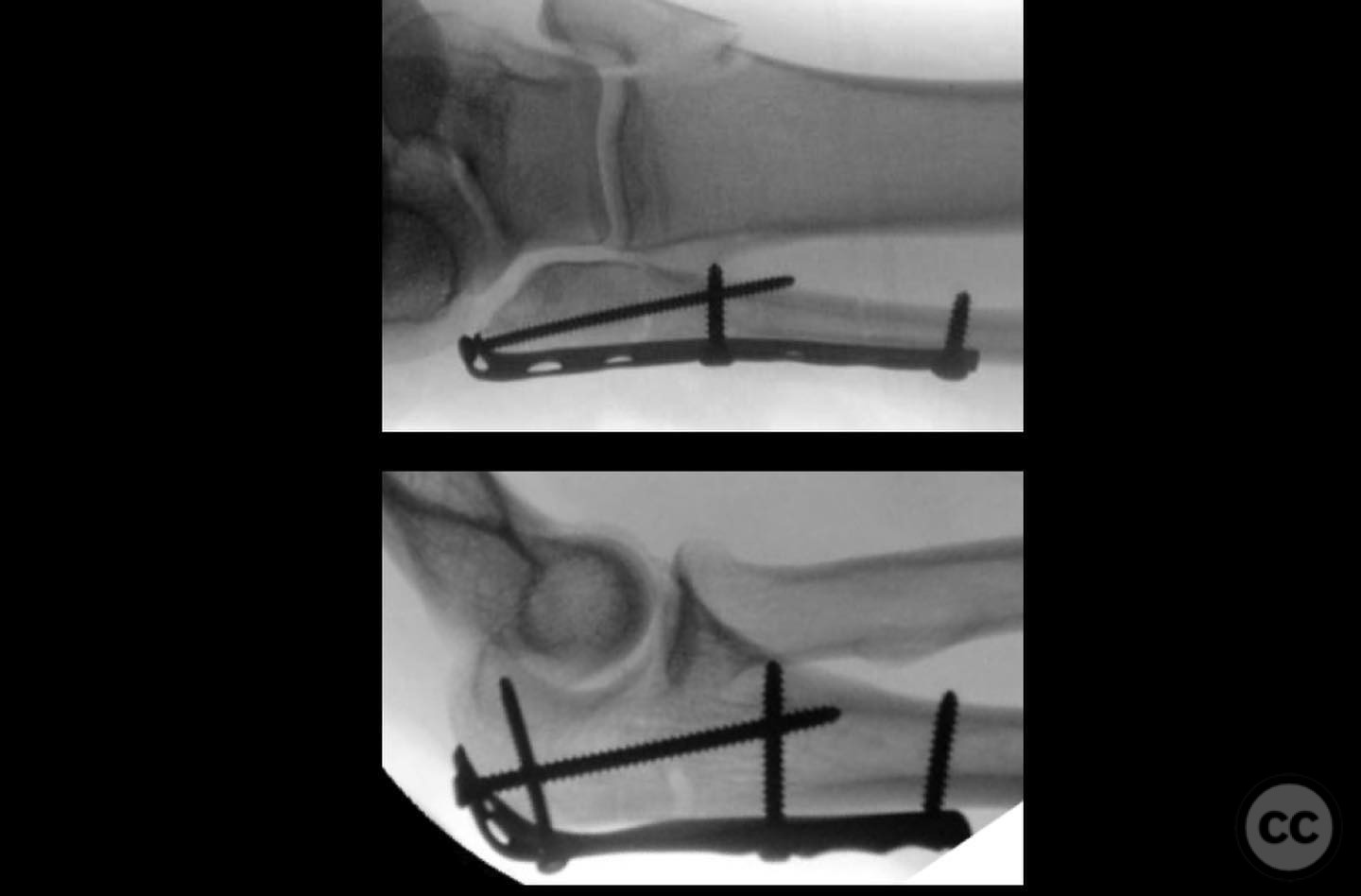
Clinical and radiological findings: A 45-year-old male presented following a fall from a height, landing on an inverted and adducted right foot. Clinical examination revealed swelling and tenderness over the medial and lateral aspects of the ankle. Radiographs demonstrated a transverse fracture of the distal fibula and a vertical shear fracture of the medial malleolus, with evidence of impaction on the medial plafond. A CT scan confirmed multifragmentary impaction involving the medial gutter.
Preoperative Plan
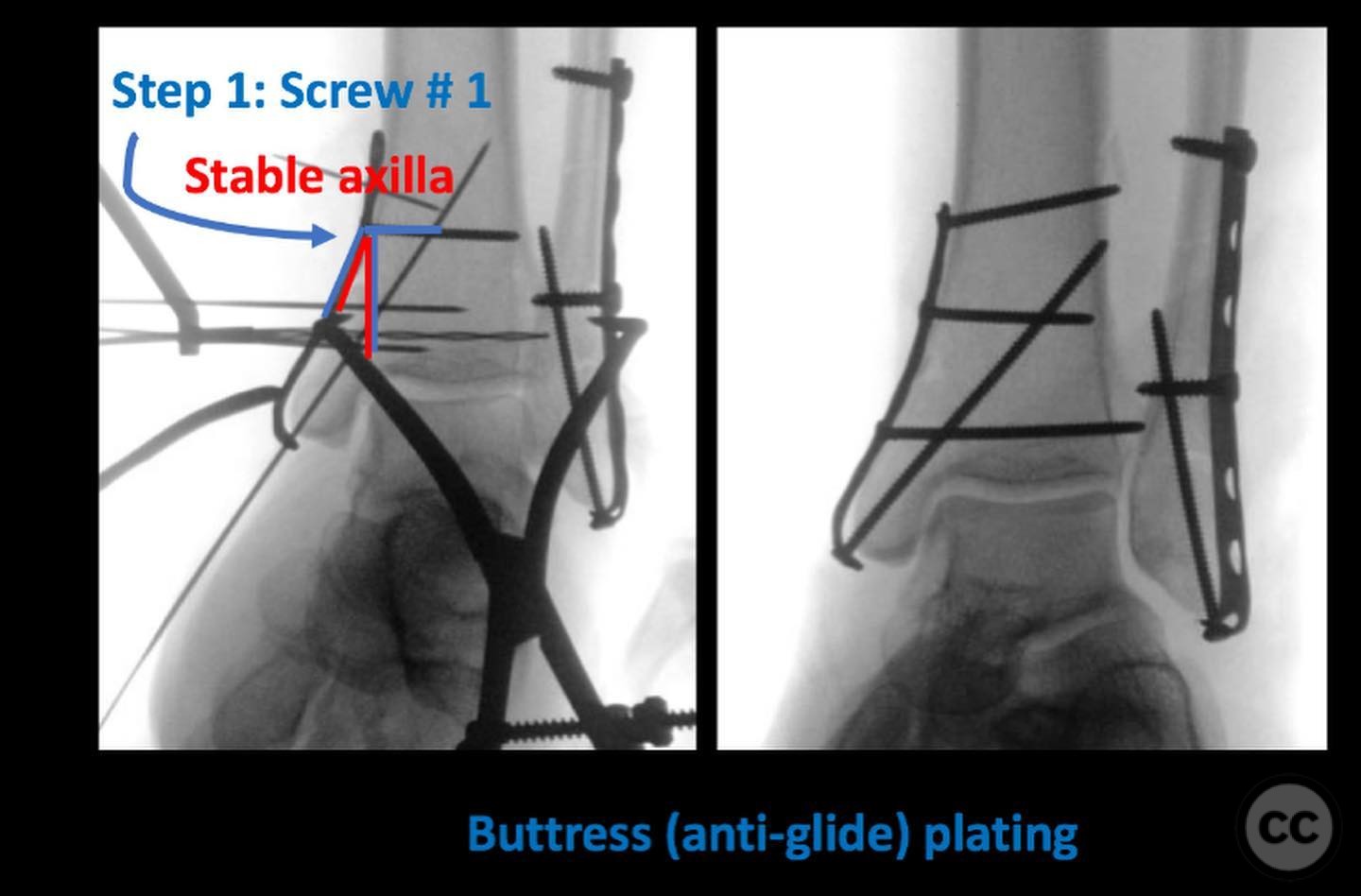
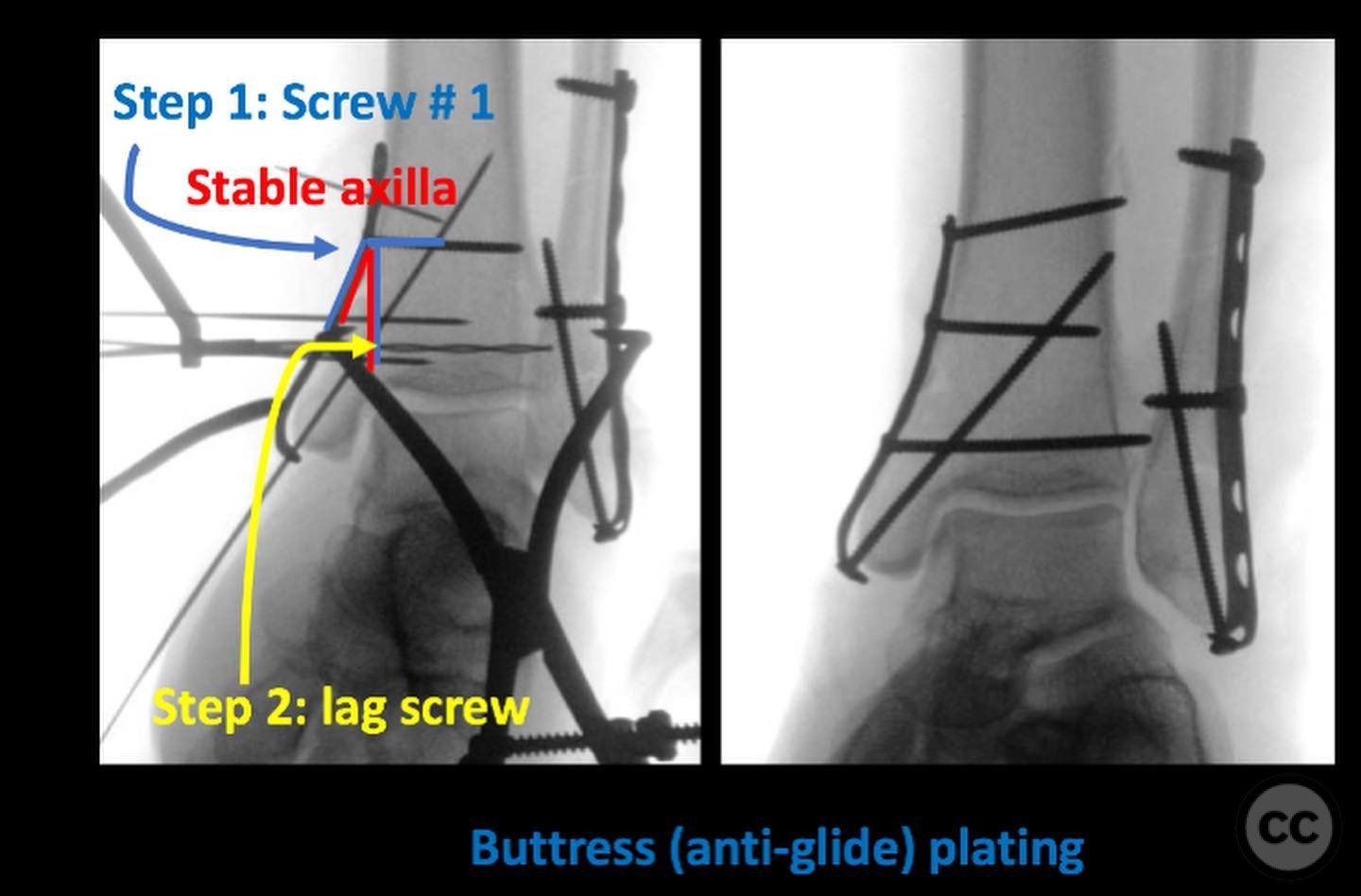
Planning remarks: The preoperative plan included a lateral approach to the fibula for tension band plating and a medial approach to the medial malleolus for buttress plating. The articular impaction was to be addressed through direct reduction and fixation.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with a bolster under the ipsilateral hip to allow for external rotation of the limb, facilitating access to both the lateral and medial aspects of the ankle.
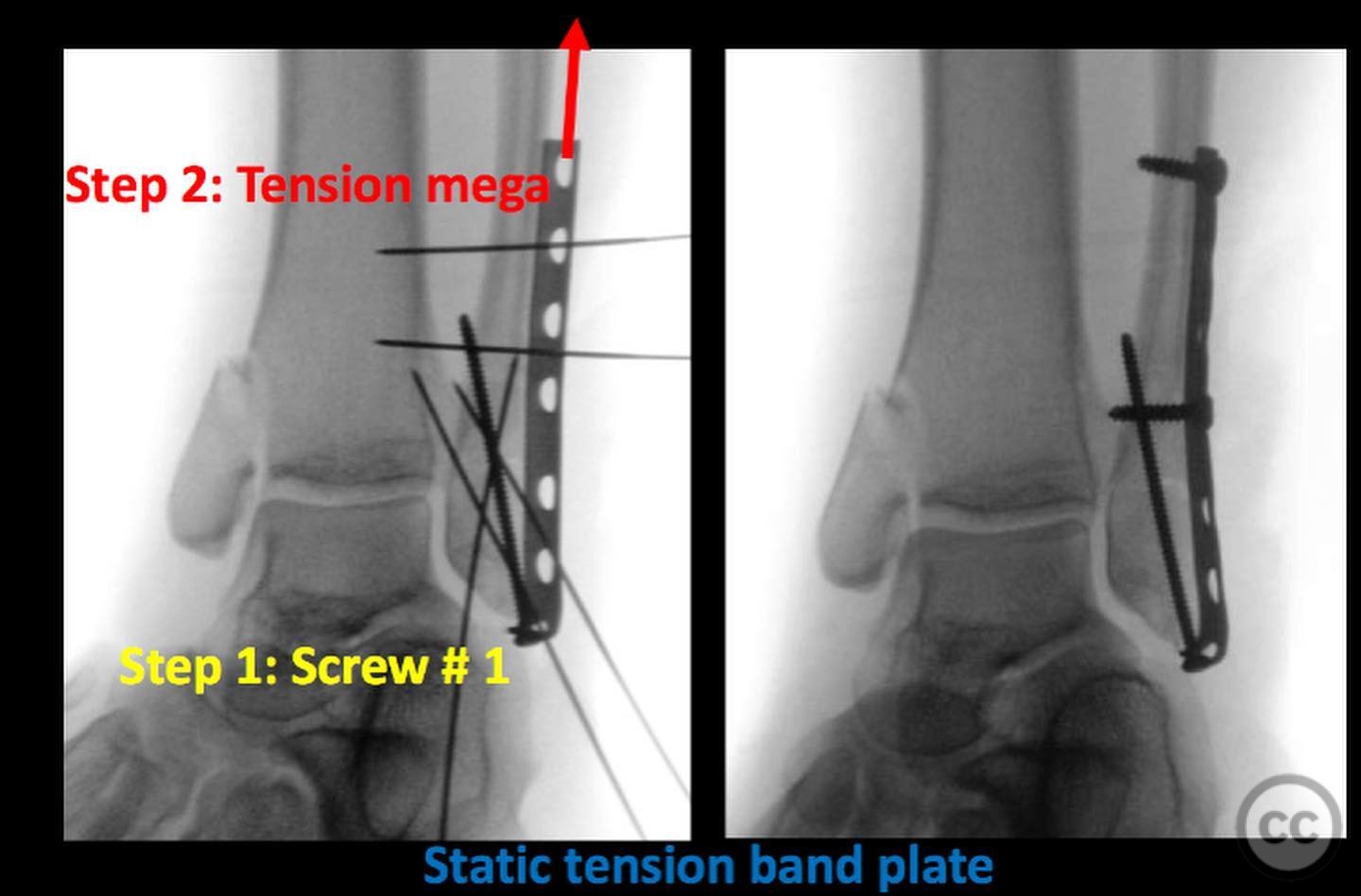
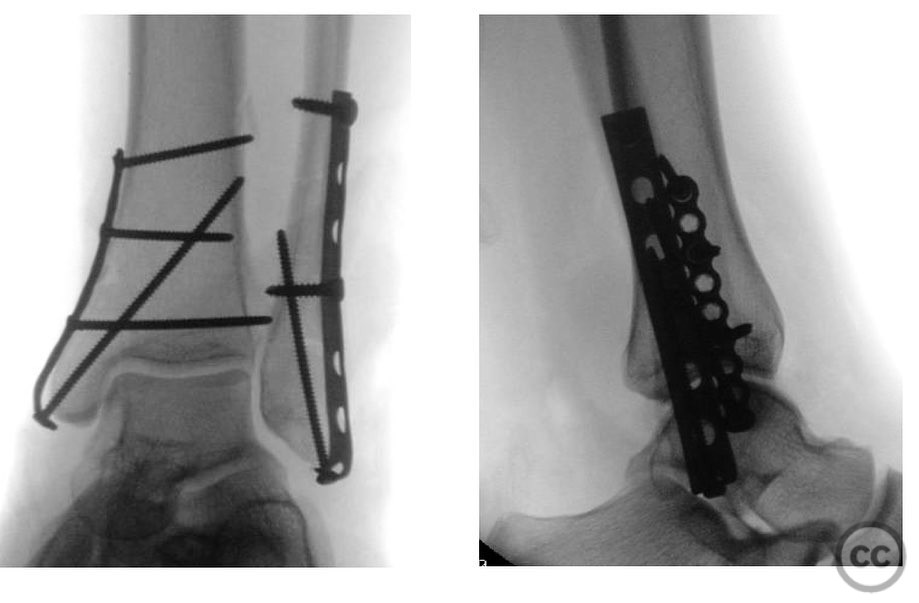
Anatomical surgical approach: A longitudinal incision was made over the lateral aspect of the distal fibula, followed by subperiosteal dissection to expose the fracture site. A static tension band plate was applied to the fibula. Medially, a separate incision was made over the medial malleolus, and subperiosteal dissection was performed to expose the fracture and impacted plafond. A buttress plate was applied to stabilize the medial malleolus, and the articular impaction was reduced and fixed with screws.
Operative remarks:The surgeon noted that the fibular fracture was highly distracted, necessitating careful tension band application to achieve stable fixation. The medial malleolar fracture required meticulous reduction due to significant articular impaction, which was addressed with multiple small fragment screws after buttress plating.
Postoperative protocol: Postoperatively, the patient was placed in a short leg splint for immobilization. Non-weight bearing was advised for 6 weeks, followed by progressive weight-bearing as tolerated, with physiotherapy initiated at 8 weeks to restore range of motion and strength.
Follow up: Not specified.
Orthopaedic implants used: Static tension band plate for fibula, buttress plate for medial malleolus, small fragment screws for articular impaction fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 390 times
19 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Supination-Adduction Ankle Fracture: Fix the Mechanism, Not Just the Bone. Journal of Orthopaedic Surgery and Traumatology. Case Report 49657088 Published Online Jul 19 2025.