








High Anterior Column Acetabular Fracture with Indirect Reduction Technique.
Score and Comment on this Case
Clinical Details
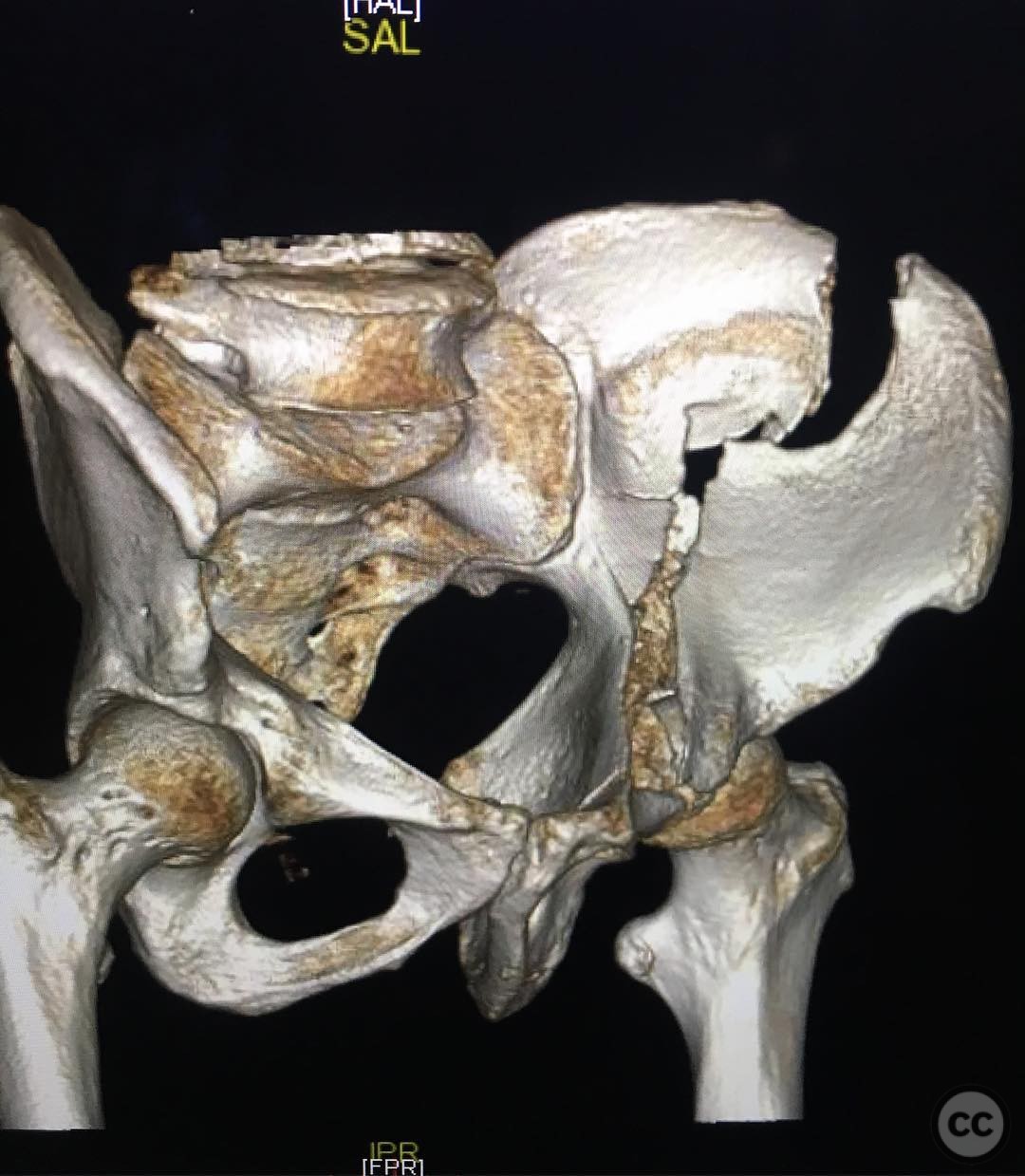
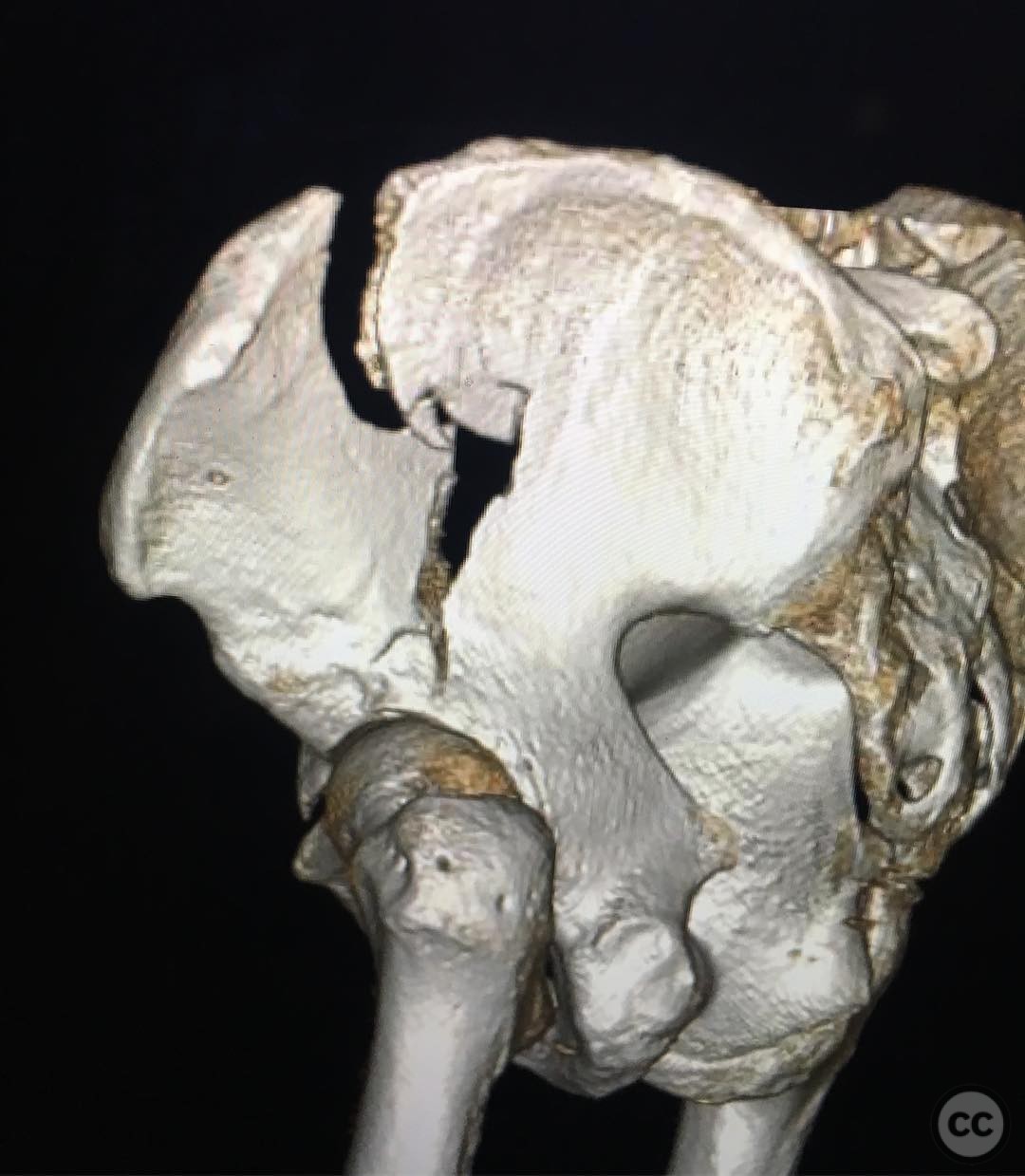
Clinical and radiological findings: A 56-year-old male sustained a high anterior column acetabular fracture following a fall from a ladder. The injury was isolated with no impaction noted. Radiological assessment confirmed the fracture pattern, consistent with the AO/OTA classification 62A3. The primary clinical objective was to achieve anatomic reduction of the articular surface and stable fixation to facilitate early hip motion.
Preoperative Plan
Planning remarks: The preoperative plan involved utilizing a lateral window approach to achieve indirect reduction of the articular surface by focusing on the iliac wing exit, fossa reads, and brim reads. The strategy included the use of fluoroscopic guidance to ensure accurate reduction of peripheral structures.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table. Skeletal traction was applied to the distal femur with 20 pounds of weight to aid in fracture reduction.
Anatomical surgical approach: A lateral window approach was employed, providing access to the iliac wing. The iliac wing exit was reduced by internally rotating the fragment using a Farabeuf clamp or Schanz pin, followed by clamping and fixation.
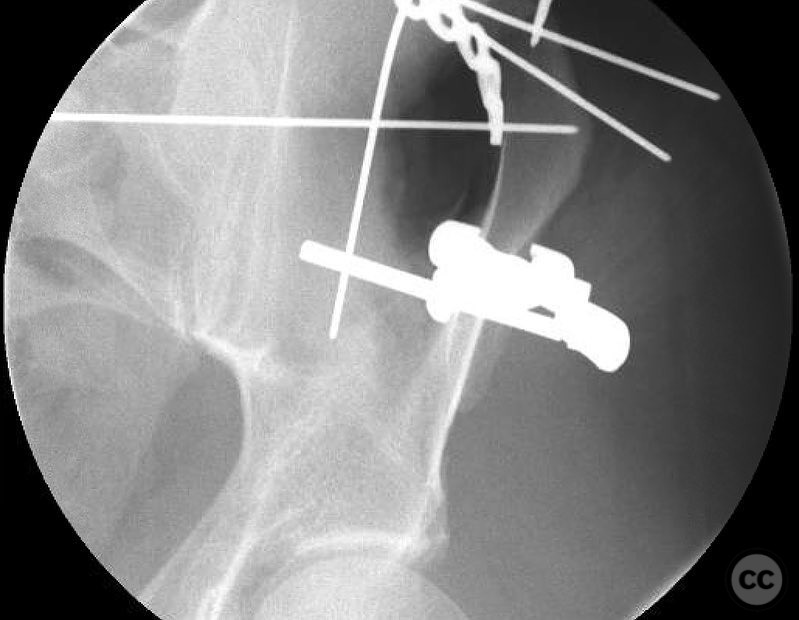
Operative remarks:Intraoperatively, the reduction of the iliac wing exit was achieved through indirect manipulation, ensuring precise alignment at the peripheral reads to indirectly restore the articular surface. A LC2 corridor screw was placed in lag fashion, and a fossa buttress plate was applied with a posterior column lag screw through the plate for stabilization. Fluoroscopic imaging was utilized extensively to confirm accurate reduction and fixation.
Postoperative protocol: Postoperative rehabilitation included early mobilization with protected weight-bearing as tolerated. Progressive range of motion exercises were initiated to maintain joint flexibility and prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: LC2 corridor screw, fossa buttress plate, posterior column lag screw.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 299 times
25 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). High Anterior Column Acetabular Fracture with Indirect Reduction Technique.. Journal of Orthopaedic Surgery and Traumatology. Case Report 48596683 Published Online Jul 25 2025.