





High-Energy Basi-Cervical and Subtrochanteric Femur Fracture in a 54-Year-Old Male.
Score and Comment on this Case
Clinical Details
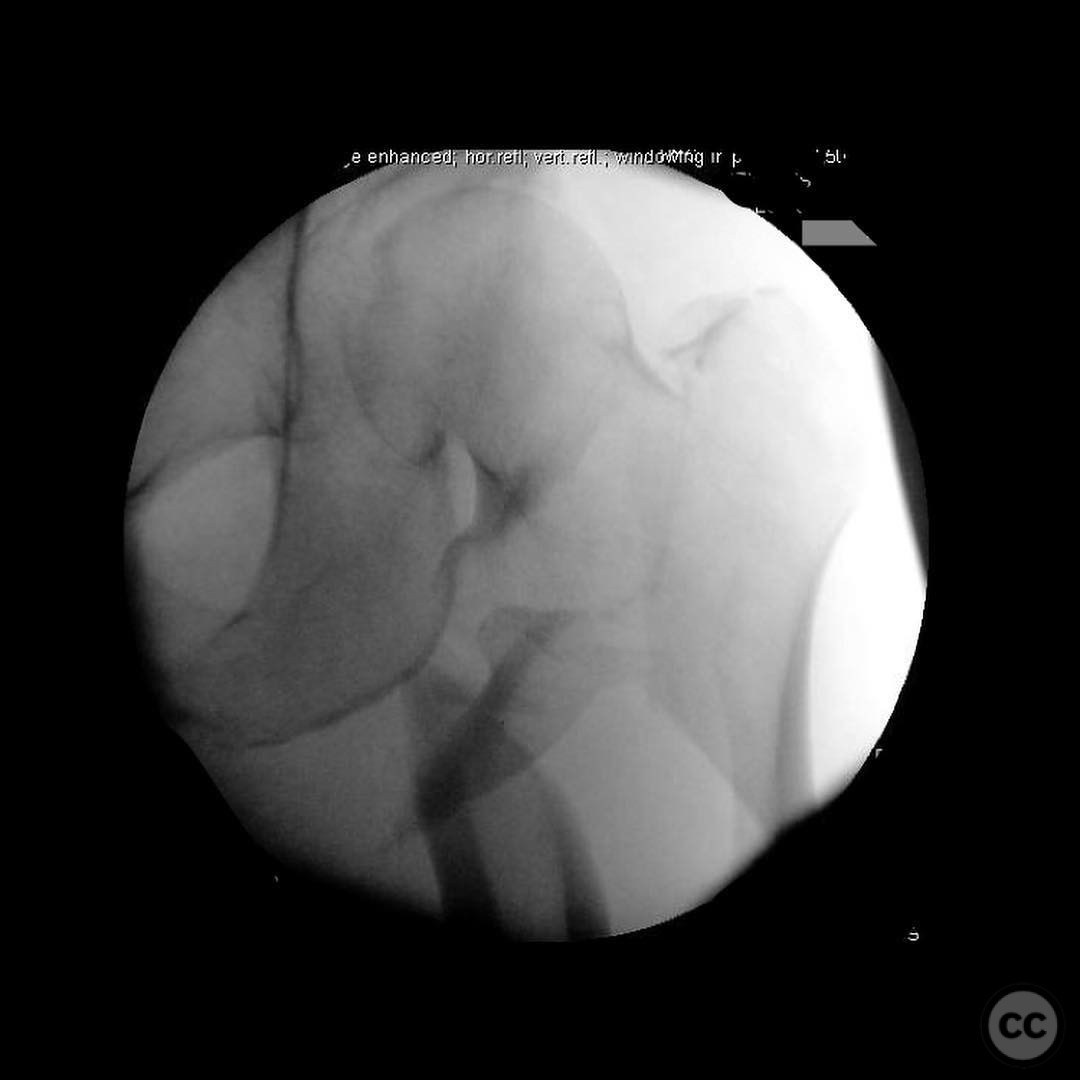
Clinical and radiological findings: A 54-year-old male, previously healthy, sustained a high-energy injury after colliding with a tree while mountain biking at high speed. Initial radiographs and fluoroscopic images revealed a complex fracture pattern involving a basi-cervical neck fracture in conjunction with a subtrochanteric fracture of the proximal femur. The fracture pattern was classified as AO/OTA 31-B2.3 for the basi-cervical component and 32-A3 for the subtrochanteric component. Due to the high-energy mechanism, closed reduction attempts were deemed unlikely to succeed.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction approach due to the complexity of the fracture pattern. A lateral subvastus approach was planned for the subtrochanteric region, combined with a Watson-Jones approach for the femoral neck. The use of a collinear clamp was anticipated to aid in the reduction of the neck and trochanteric fragments, followed by cerclage wiring for stabilization of the subtrochanteric component.
Surgical Discussion
Patient positioning: The patient was positioned laterally on a flat-top operating table with the affected leg free to allow for optimal access and manipulation during the surgical procedure.
Anatomical surgical approach: A lateral subvastus approach was performed, involving an incision along the lateral aspect of the thigh, with careful dissection through the vastus lateralis muscle to expose the subtrochanteric region. Concurrently, a Watson-Jones approach was utilized for the femoral neck, involving an incision over the anterior aspect of the hip, retracting the tensor fascia lata and gluteus medius to access the femoral neck.
Operative remarks:The surgeon noted that closed reduction was not feasible due to the fracture complexity)Scroll through the fluoro images — these are manual traction views, closely simulating what you'd expect to see if the patient were placed on a fracture table.)
. A collinear clamp was employed to achieve reduction of the neck and trochanteric fragments, ensuring proper alignment. Cerclage wiring was applied to stabilize the subtrochanteric fracture. The nail entry point was deliberately medialized to prevent varus malalignment. The integrated screw design of the chosen implant allowed for significant compression across the basi-cervical fracture, achieving stable fixation.
Postoperative protocol: Postoperatively, the patient was advised to adhere to a non-weight-bearing protocol on the affected limb for 6 weeks, followed by progressive weight-bearing as tolerated. Range of motion exercises were initiated early to prevent joint stiffness.
Follow up: Not specified.
Orthopaedic implants used: Intramedullary nail with integrated screw design, collinear clamp, cerclage wires.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 372 times
23 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). High-Energy Basi-Cervical and Subtrochanteric Femur Fracture in a 54-Year-Old Male.. Journal of Orthopaedic Surgery and Traumatology. Case Report 48430657 Published Online Jul 23 2025.