













High-Energy Open Tibial Shaft Fracture with Bifocal Fibular Fractures and Syndesmotic Instability
Score and Comment on this Case
Clinical Details
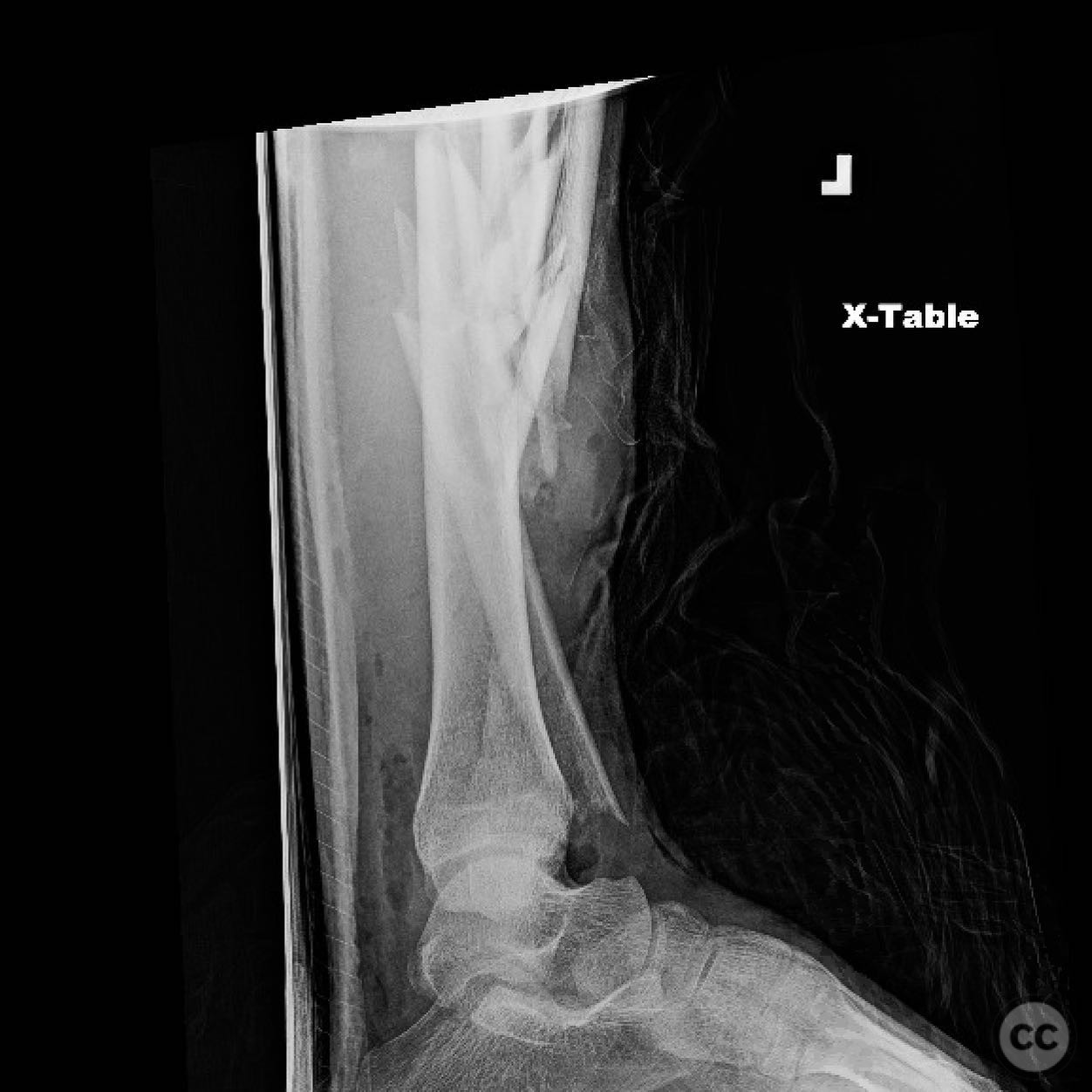
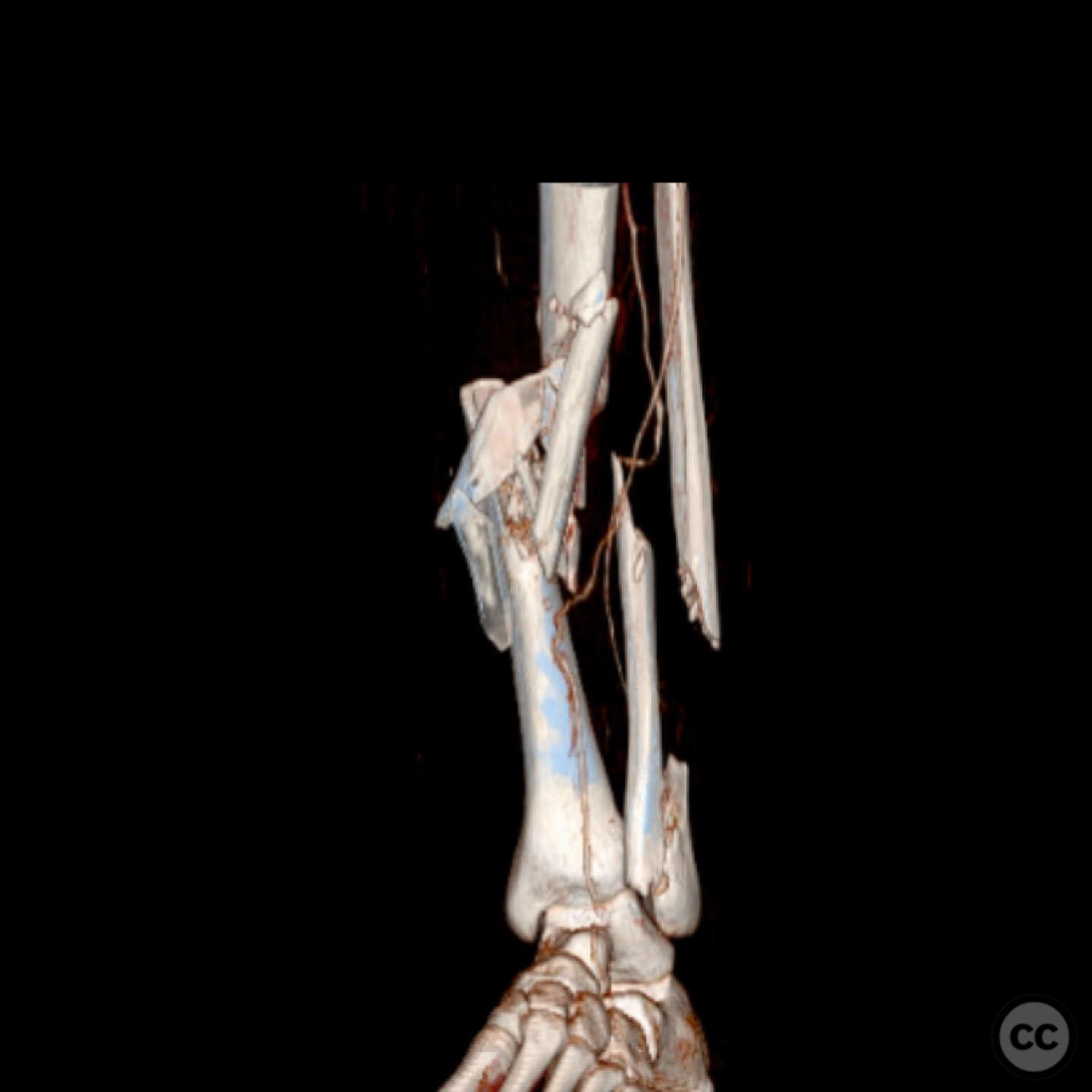
Clinical and radiological findings: A 30-year-old male sustained a high-energy open tibial shaft fracture following a motorcycle crash. The injury presented with a 20 x 15 cm open wound on the medial aspect of the tibia. The fibula exhibited bifocal open fractures, each with a 1 cm wound. Initial radiographs and clinical examination indicated disruption of the syndesmosis and intraosseous membrane. The AO/OTA classification for the tibial fracture is 42-C3, indicating a complex fracture pattern.
Preoperative Plan
Planning remarks: The preoperative plan included thorough debridement of the open wounds, assessment of intraosseous membrane integrity, and stabilization of both tibial and fibular fractures. A decision was made to fix both fibular fractures to restore length and stabilize the syndesmosis. Options for tibial defect management included the Masquelet technique or nail transport, depending on the vascularization of retained fragments.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the affected leg prepped and draped in a sterile fashion. A tourniquet was not applied due to the open nature of the injury.
Anatomical surgical approach: A direct medial approach to the tibia was utilized for debridement and fracture management. The fibular fractures were accessed through separate lateral incisions to allow for direct reduction and fixation. The syndesmosis was addressed through an anterolateral approach to the ankle.
Operative remarks:Intraoperatively, after debridement, the stripped tibial fragments were cleaned on the back table and used temporarily for reduction before removal. The distal fibula remained short after clamping, and a positive Cotton test confirmed syndesmotic instability, necessitating fixation of both fibular fractures followed by syndesmotic stabilization. Implant choice was considered carefully, with options including dual plating or a combination of plate and nail constructs. A fine wire frame was deemed suitable for external fixation. Coordination with plastic surgery was planned for soft tissue coverage within 48 hours.
Postoperative protocol: Postoperatively, the patient was placed in a fine wire frame for stabilization. Weight-bearing was restricted initially, with gradual progression based on clinical and radiographic healing. Early range of motion exercises were encouraged to prevent joint stiffness.
Follow up: Not specified.
Orthopaedic implants used: Dual plating for fibular fractures, external fixator (fine wire frame), syndesmotic screw fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 441 times
13 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). High-Energy Open Tibial Shaft Fracture with Bifocal Fibular Fractures and Syndesmotic Instability. Journal of Orthopaedic Surgery and Traumatology. Case Report 48236189 Published Online Jul 13 2025.