











Posterolateral Elbow Dislocation with Coronoid Base and Anteromedial Facet Fracture.
Score and Comment on this Case
Clinical Details
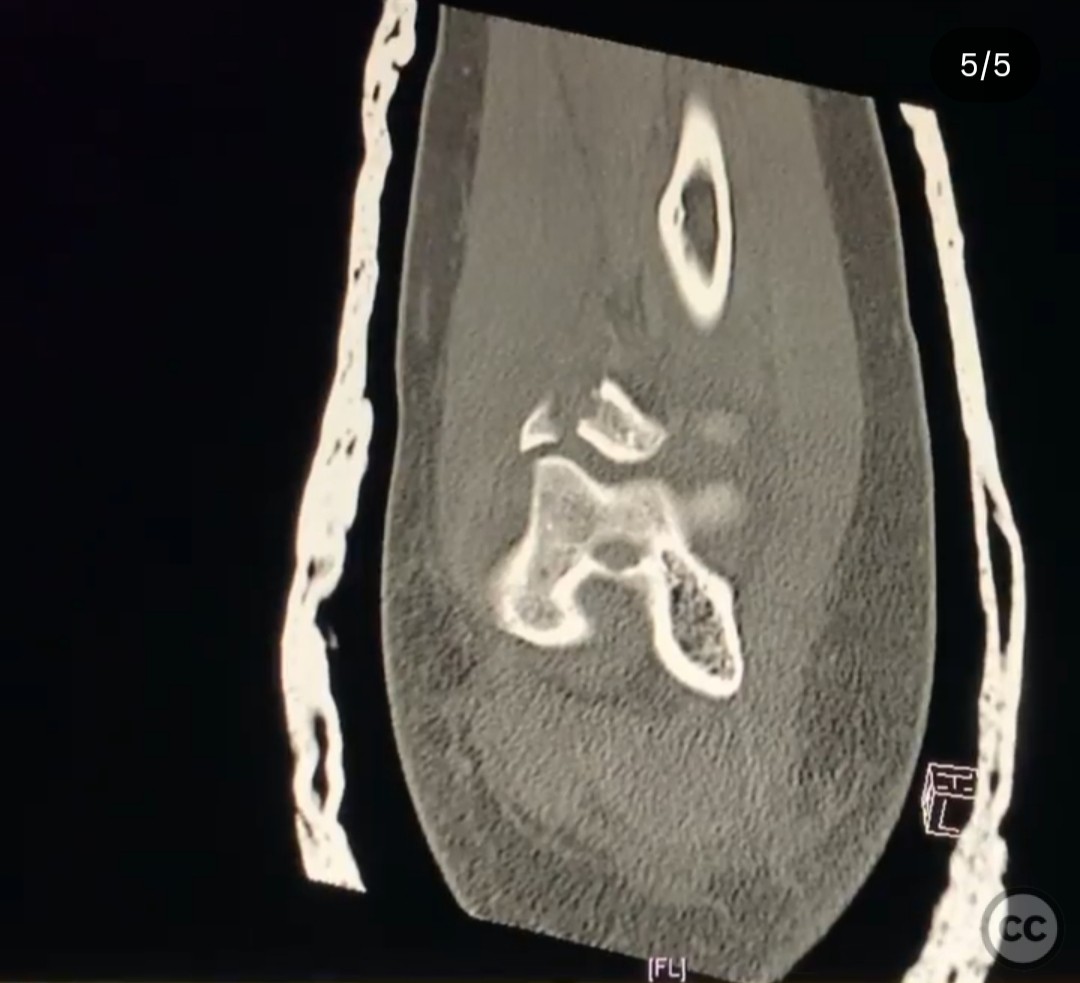
Clinical and radiological findings: A 34-year-old male sustained an isolated closed elbow injury following a fall while bouldering. The injury presented as a posterolateral elbow dislocation accompanied by a large coronoid base fracture and a separate anteromedial facet fracture. There was an associated rupture of the lateral ulnar collateral ligament (LUCL). Neurological and vascular examinations were unremarkable.
Preoperative Plan
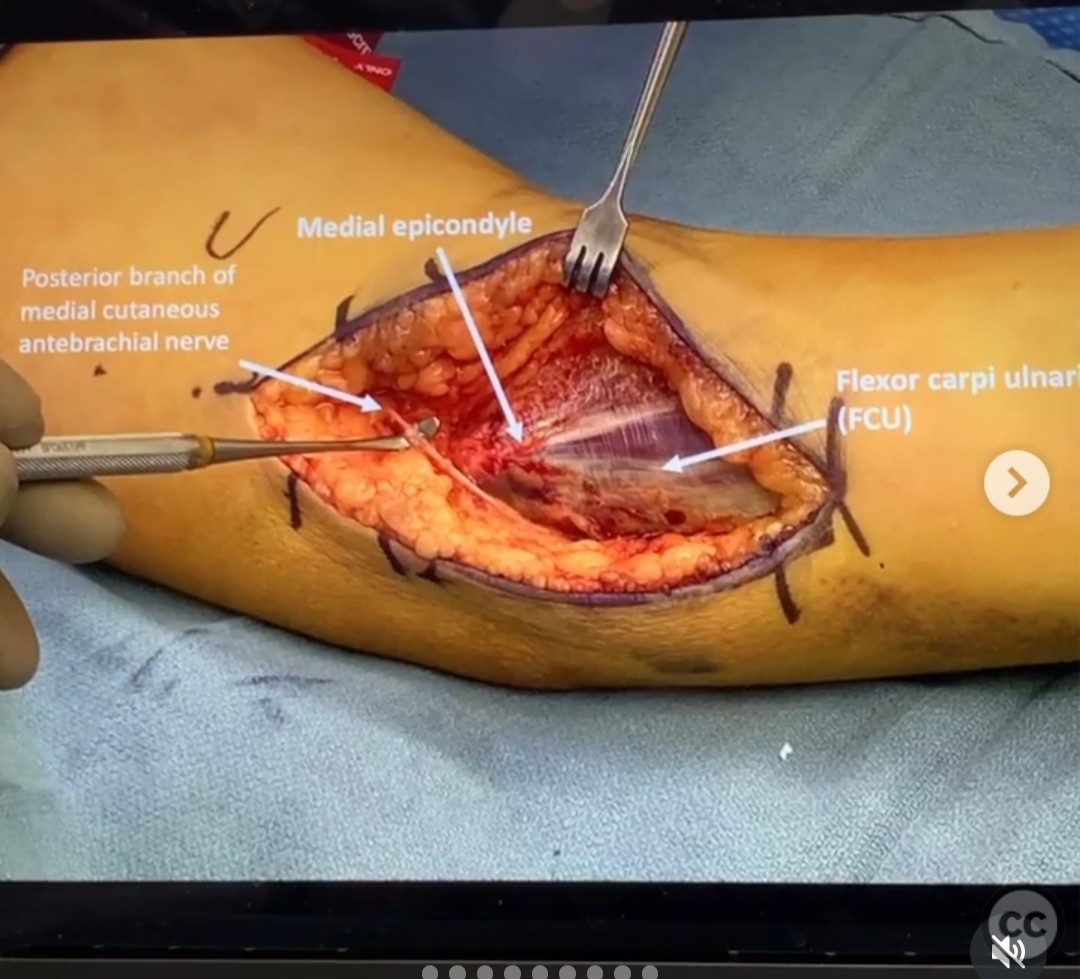
Planning remarks: The preoperative plan involved addressing both sides of the elbow to stabilize the joint. The surgical approach considered was either a posterior midline approach with large skin flaps or two separate incisions. The medial approach was chosen, specifically utilizing the flexor carpi ulnaris (FCU) split for optimal access to the fracture pattern.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the arm placed on an arm board to allow for optimal access to both medial and lateral aspects of the elbow.
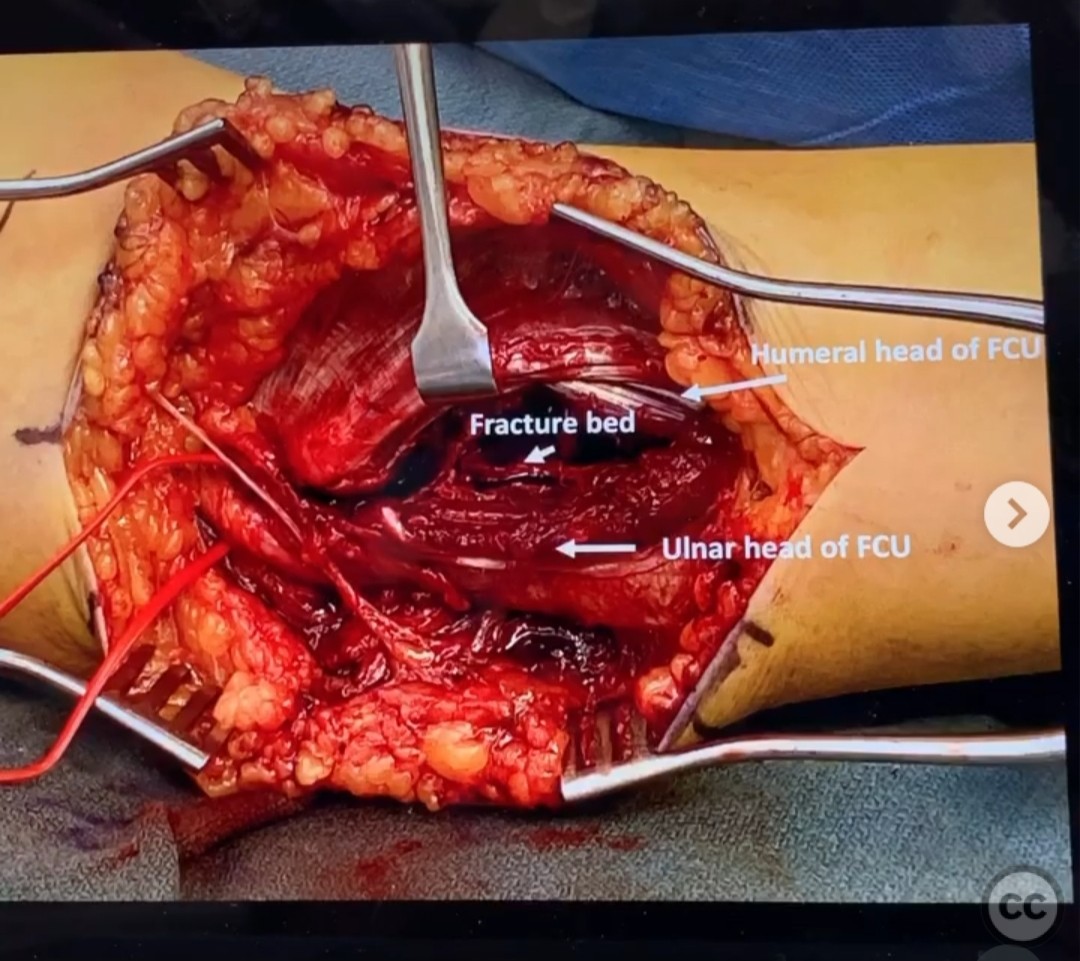
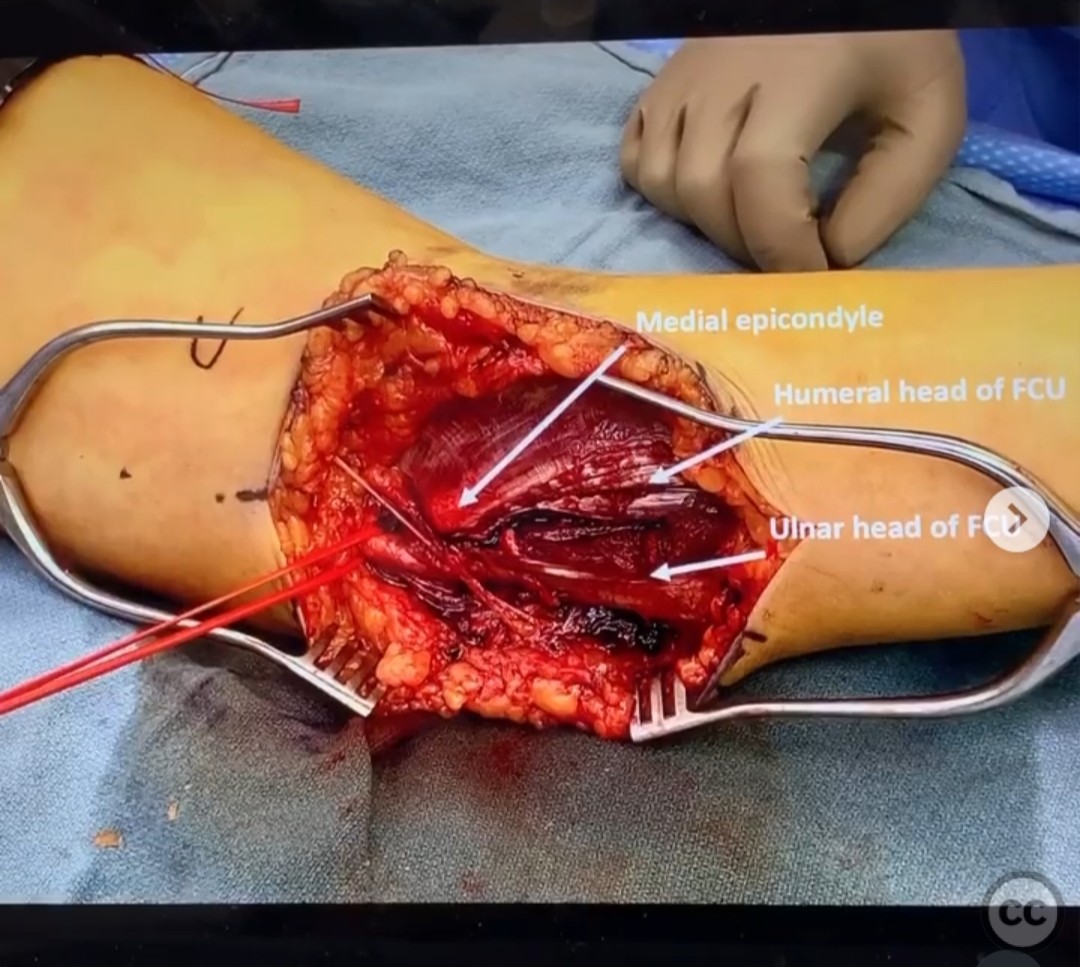
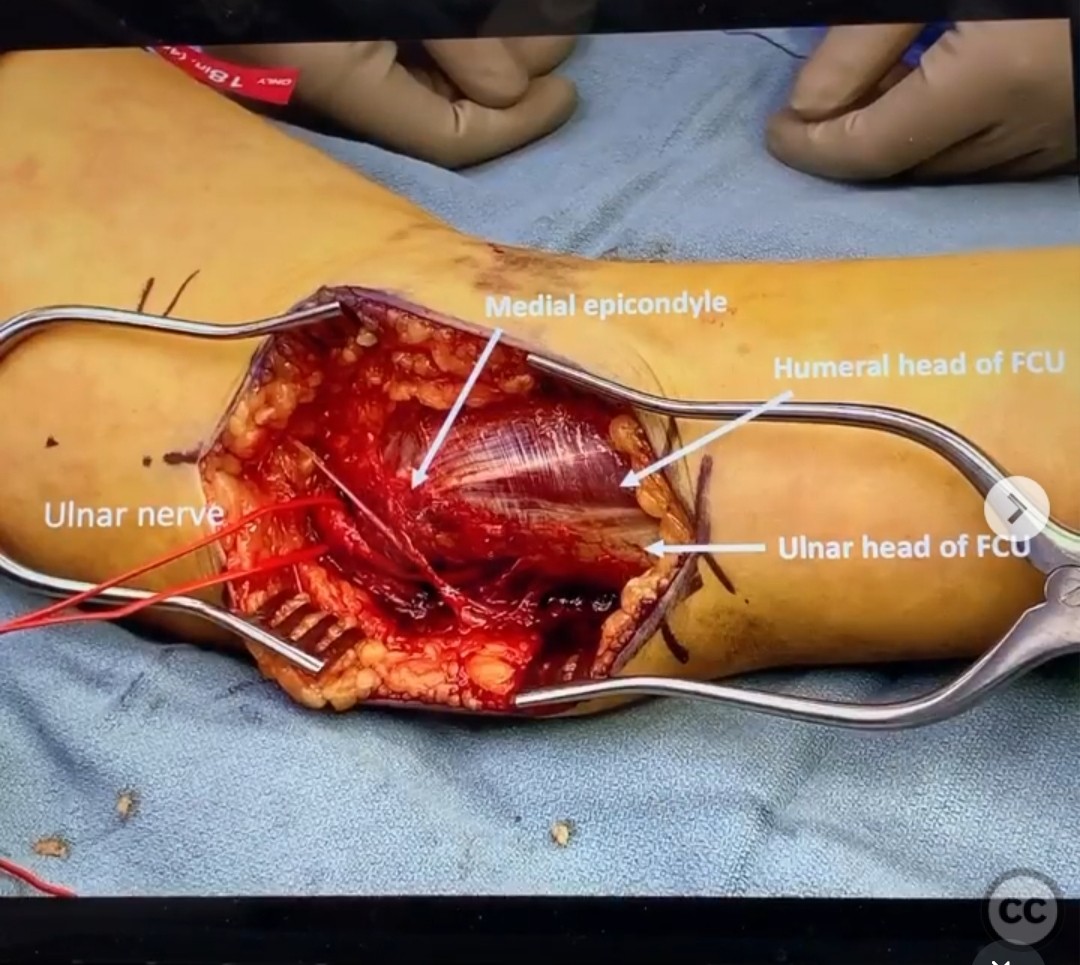
Anatomical surgical approach: The medial approach involved identifying and protecting the branches of the antebrachial nerve and the ulnar nerve. The flexor carpi ulnaris (FCU) was split by finding the interval between its ulnar and humeral heads. This provided access to the coronoid base and anteromedial facet fractures.
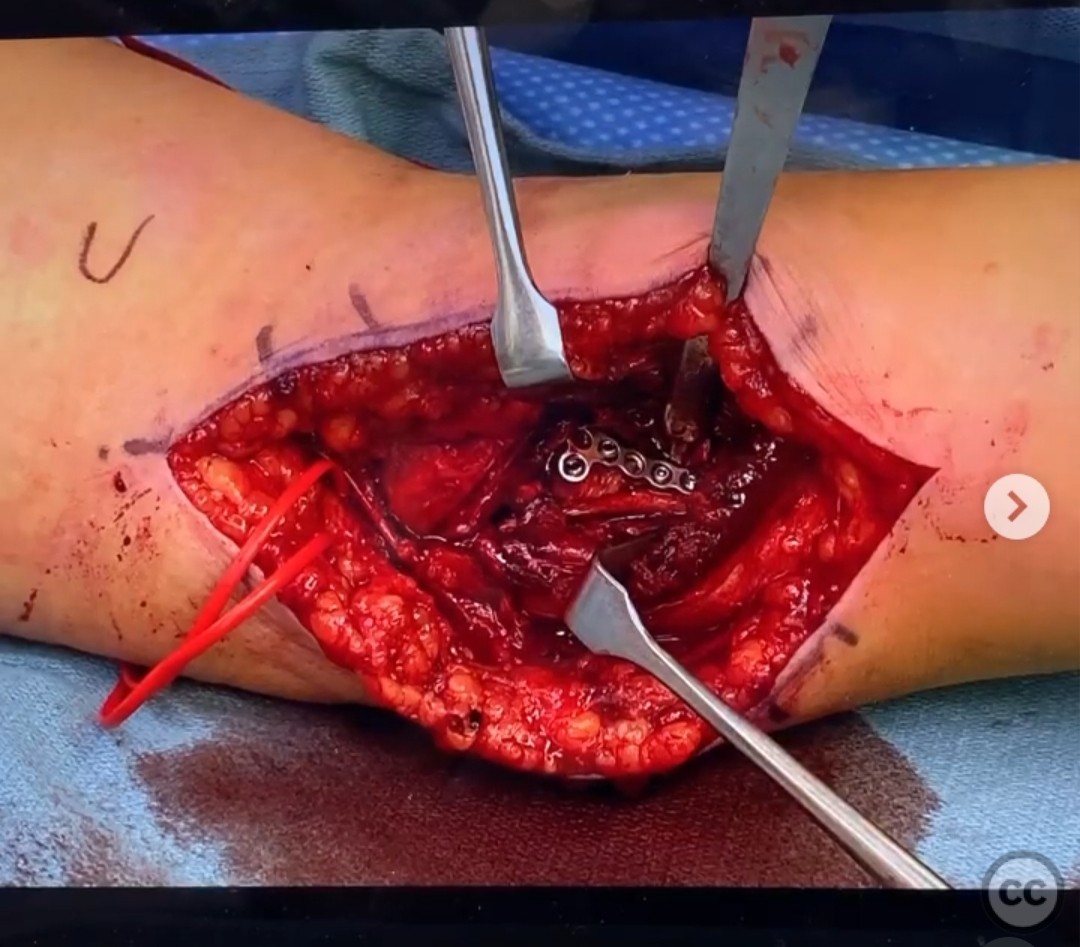
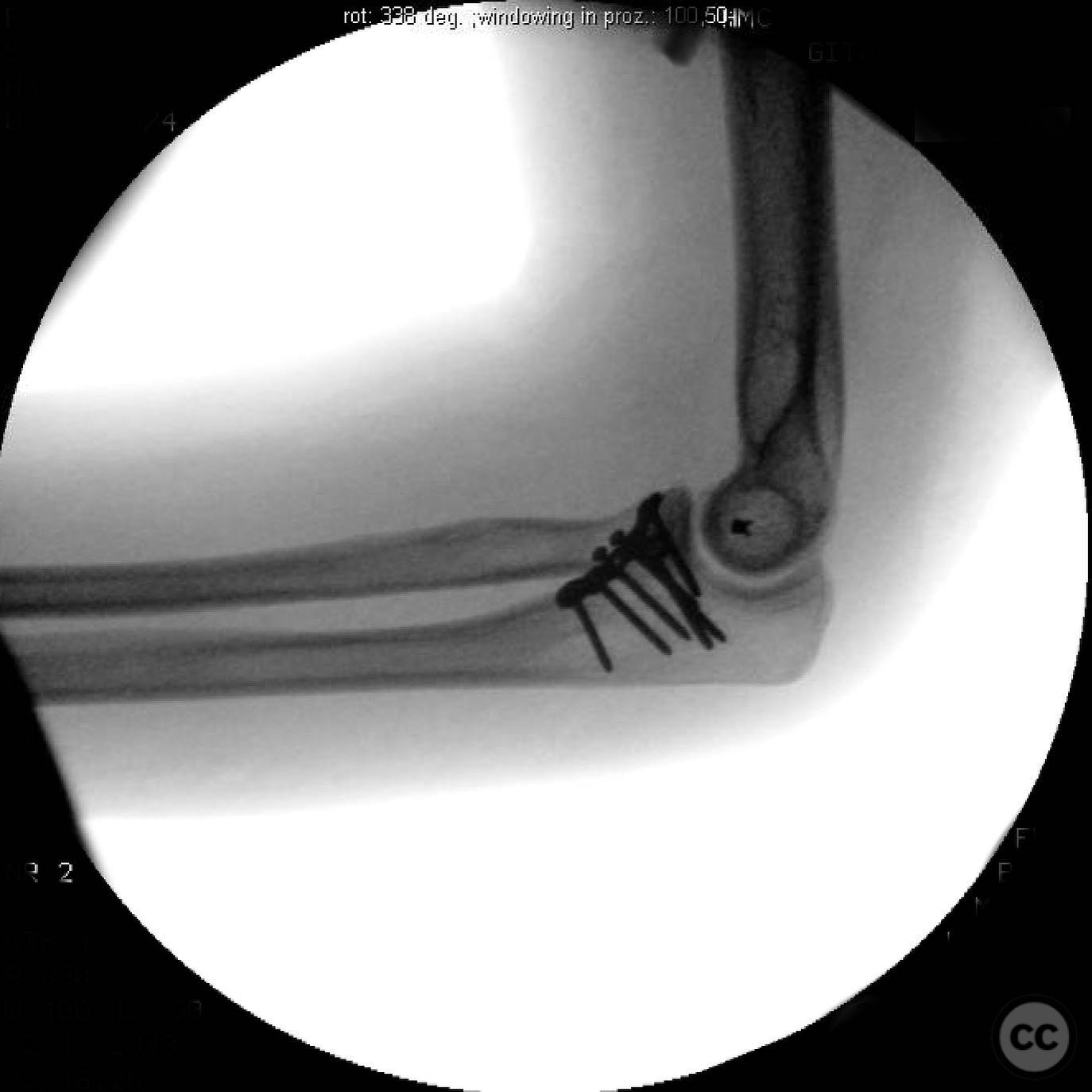
Operative remarks:The coronoid base was reduced first, followed by the anteromedial facet, which had the medial ulnar collateral ligament attached. Fixation was achieved using a 2.0mm T-plate and screws, ensuring no violation of the proximal radioulnar joint (PRUJ). The lateral ulnar collateral ligament (LUCL) had avulsed from its origin at the Kocher interval and was repaired using a suture anchor. Elbow stability was confirmed through a full range of motion, negating the need for additional stabilization methods such as an internal stabilizer or static external fixator.
Postoperative protocol: Postoperative rehabilitation included early mobilization with active range of motion exercises initiated immediately to prevent stiffness. Weight-bearing restrictions were maintained until radiographic evidence of fracture healing was confirmed.
Follow up: Not specified.
Orthopaedic implants used: 2.0mm T-plate, screws, suture anchor.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 242 times
18 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Posterolateral Elbow Dislocation with Coronoid Base and Anteromedial Facet Fracture.. Journal of Orthopaedic Surgery and Traumatology. Case Report 47983386 Published Online Jul 18 2025.