





Unstable Displaced Posterior Column/Posterior Wall Acetabular Fracture with Intra-articular Chondrocancellous Fragment in Morbid Obesity
Score and Comment on this Case
Clinical Details
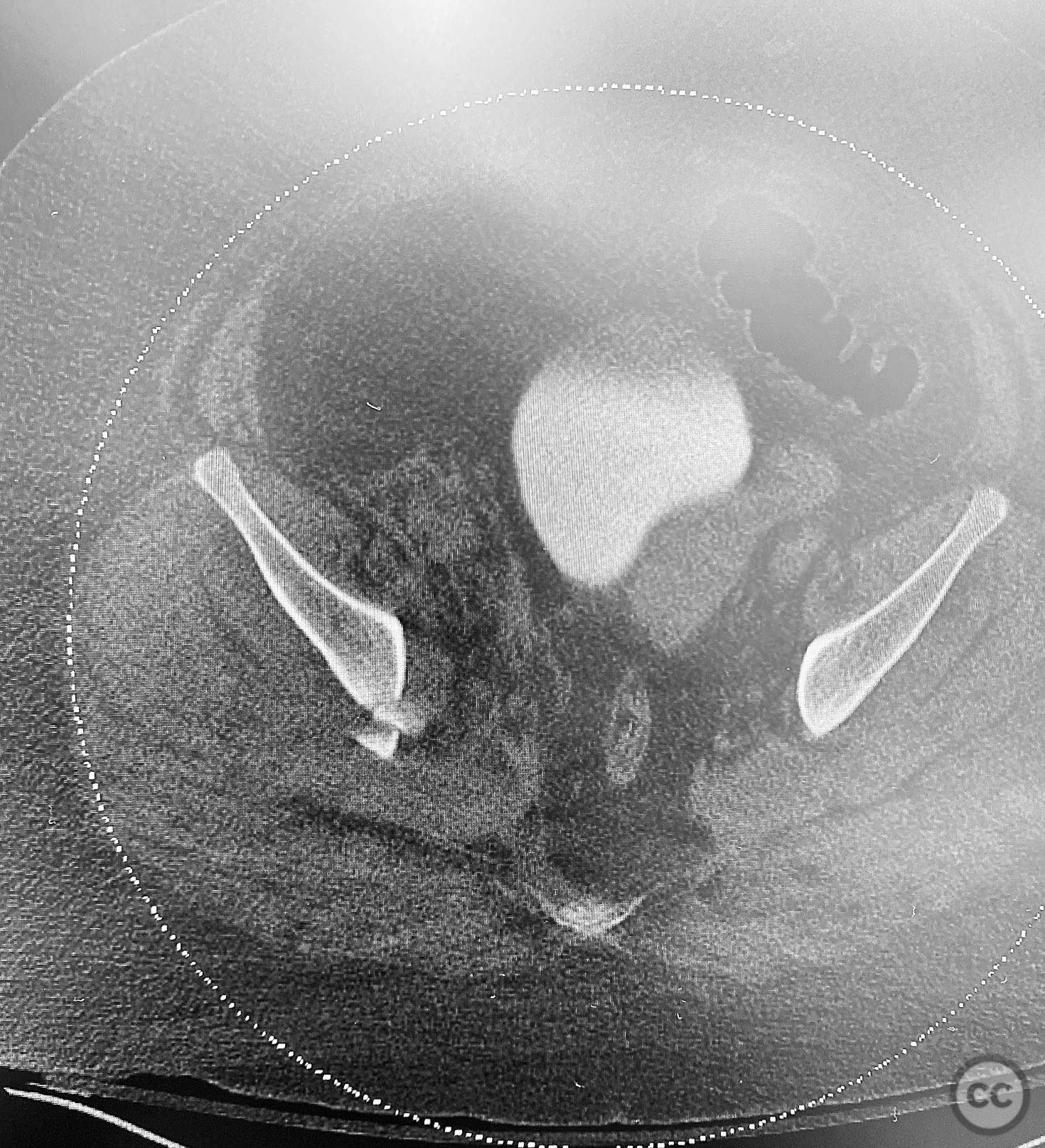
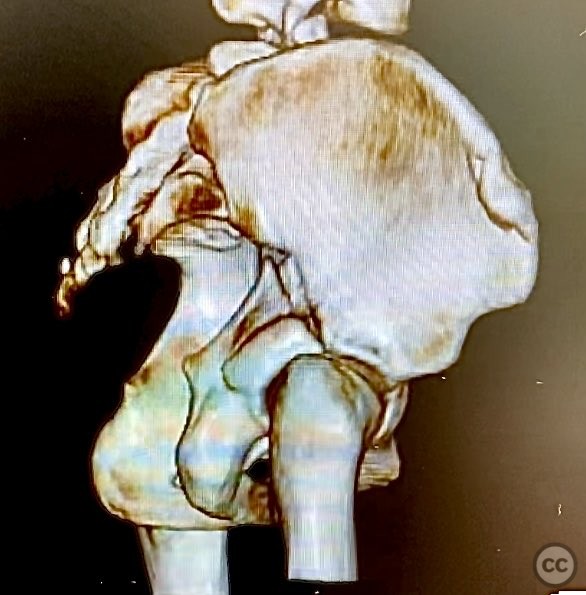
Clinical and radiological findings: The patient is morbidly obese and sustained an unstable, displaced posterior column/posterior wall (PC/PW) acetabular fracture. Axial computed tomography images revealed a 2x2x1.5 cm pyramidal chondrocancellous articular fragment wedged in the fracture plane near the incisura ischiadica major (greater sciatic notch). Surface-rendered reconstructions further delineated the fracture morphology and fragment position. Obesity was noted to complicate all aspects of management, including anatomical localization, intraoperative imaging, and soft tissue handling.
Preoperative Plan
Planning remarks: The preoperative plan involved open reduction and internal fixation of the posterior column and posterior wall fragments, with retrieval and anatomic reduction of the intra-articular chondrocancellous fragment. A Kocher-Langenbeck approach was selected for direct access to the posterior acetabulum. Contoured plates and screws were prepared for definitive fixation.
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position. Due to body habitus, a 2mm Steinmann pin was placed under fluoroscopic guidance to accurately identify the femoral shaft and facilitate correct limb alignment intraoperatively.
Anatomical surgical approach: A standard Kocher-Langenbeck approach was performed. The incision was made along the posterior aspect of the coxa, centered over the greater trochanter and extending distally along the femoral shaft. Subcutaneous adipose tissue was dissected to expose the fascia lata, which was incised in line with the skin incision. The gluteus maximus was split in line with its fibers, and the short external rotators (piriformis, obturator internus, gemelli) were identified and retracted or released as necessary to expose the posterior column and wall of the acetabulum. The sciatic nerve was identified and protected throughout. The fracture site was exposed, and the wedged chondrocancellous fragment was retrieved from the region adjacent to the incisura ischiadica major. Anatomic reduction of the articular fragment, posterior column, and posterior wall was achieved, followed by fixation with contoured plates and screws.
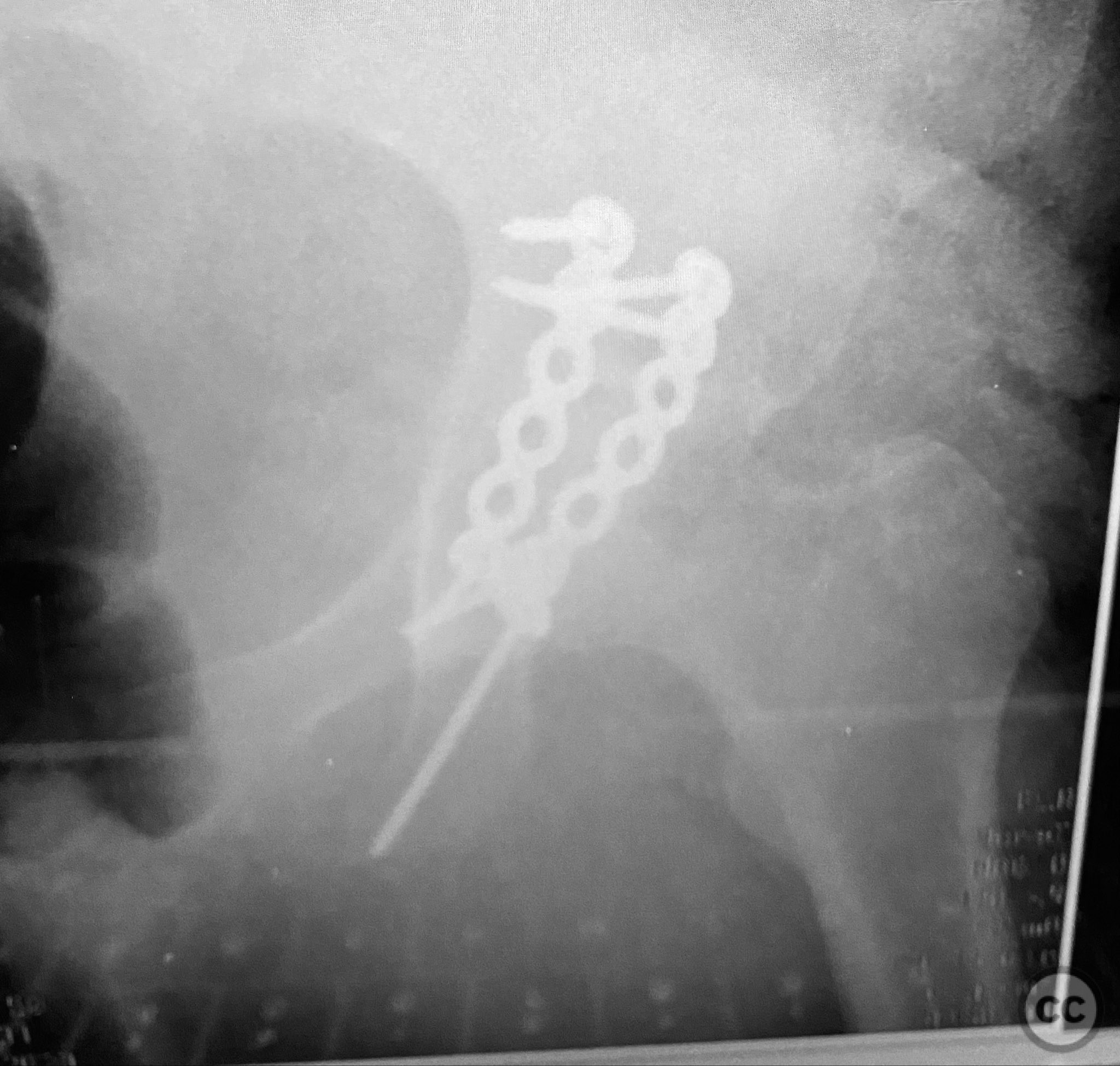
Operative remarks:Morbid obesity significantly complicated intraoperative exposure, anatomical landmark identification, retraction, and fluoroscopic imaging. A 2mm pin placed under C-arm guidance facilitated accurate identification of the femoral shaft for limb positioning. Retrieval of the intra-articular chondrocancellous fragment required careful dissection near the greater sciatic notch. After reduction of all fragments, contoured plates and screws were applied to maintain stability. Postoperative imaging confirmed accurate reduction and appropriate implant placement. Wound management strategies were employed to mitigate increased risk of complications associated with obesity.
Postoperative protocol: Early passive range of motion exercises were initiated postoperatively. Toe-touch weight bearing was maintained for 8-12 weeks, with progression to partial and then full weight bearing as radiographic healing permitted. Wound care protocols were intensified due to increased risk of dehiscence and infection in morbid obesity.
Follow up: Not specified
Orthopaedic implants used: Contoured reconstruction plates; cortical screws
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 242 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Unstable Displaced Posterior Column/Posterior Wall Acetabular Fracture with Intra-articular Chondrocancellous Fragment in Morbid Obesity. Journal of Orthopaedic Surgery and Traumatology. Case Report 47764860 Published Online Sep 12 2025.