





Complex Elbow Trauma with Proximal Radius Fracture and Capitellum Involvement.
Score and Comment on this Case
Clinical Details
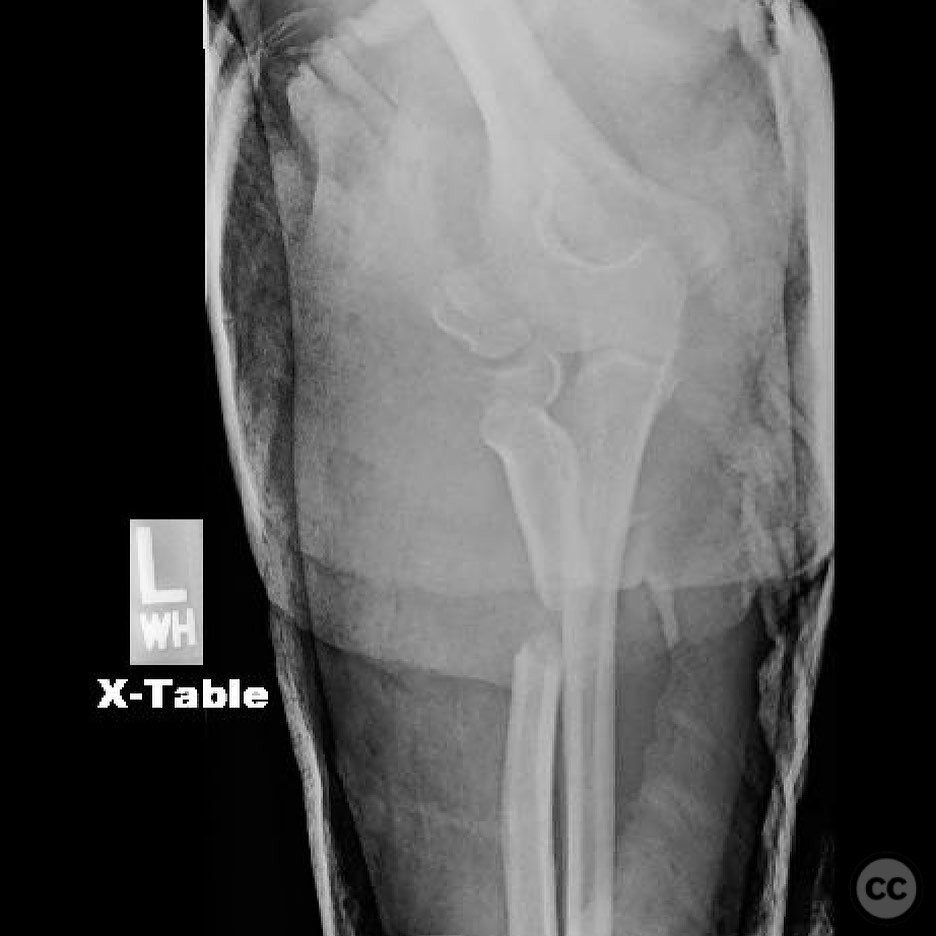
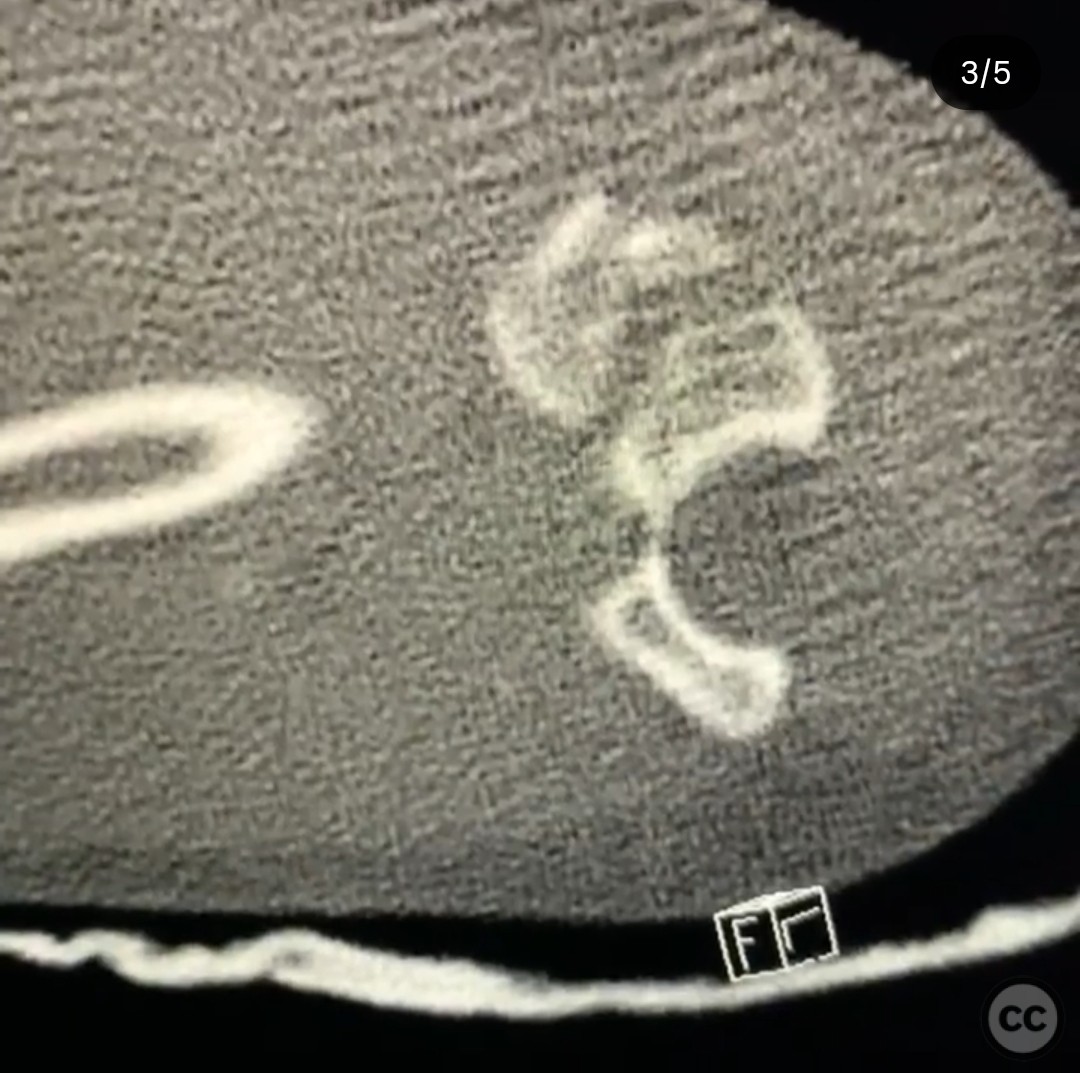
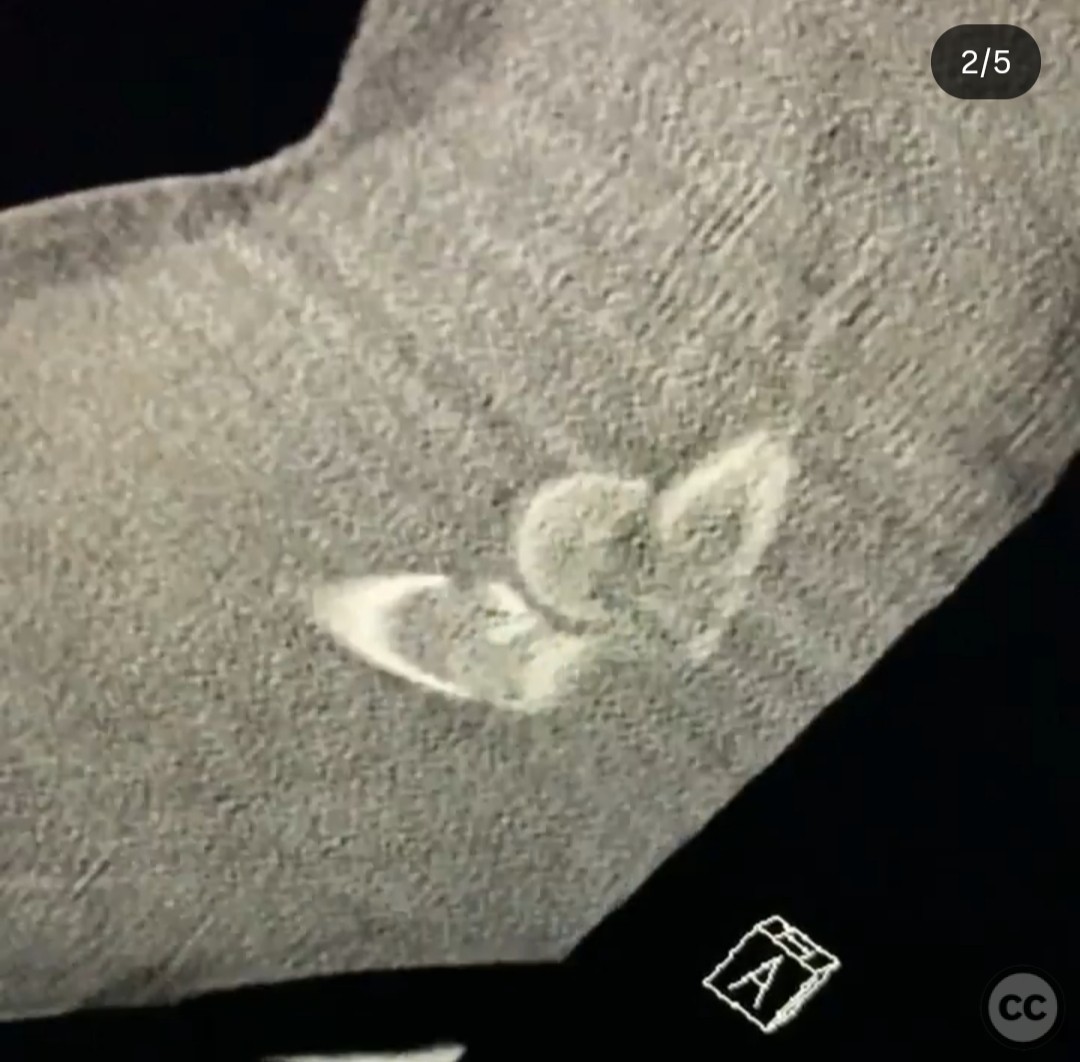
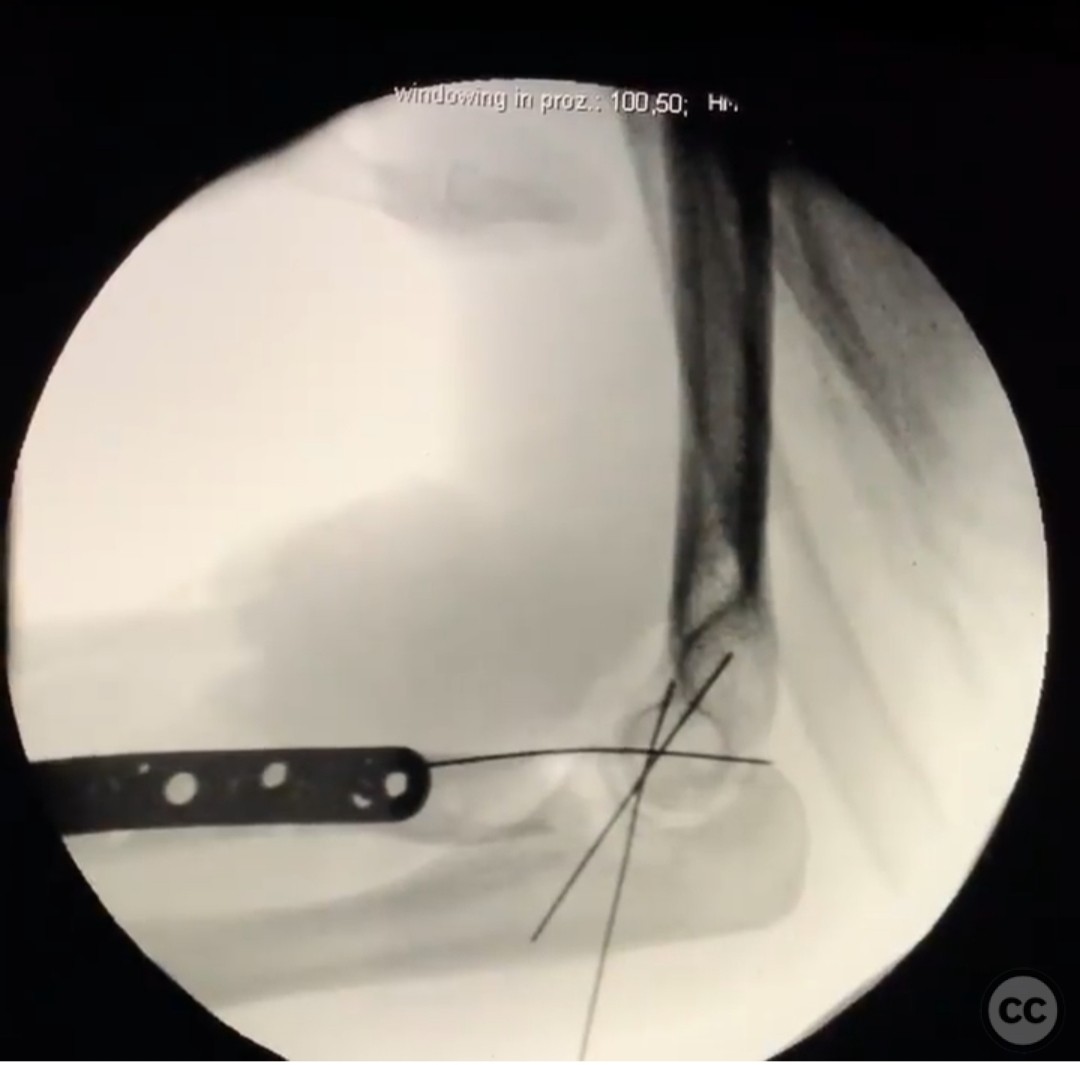
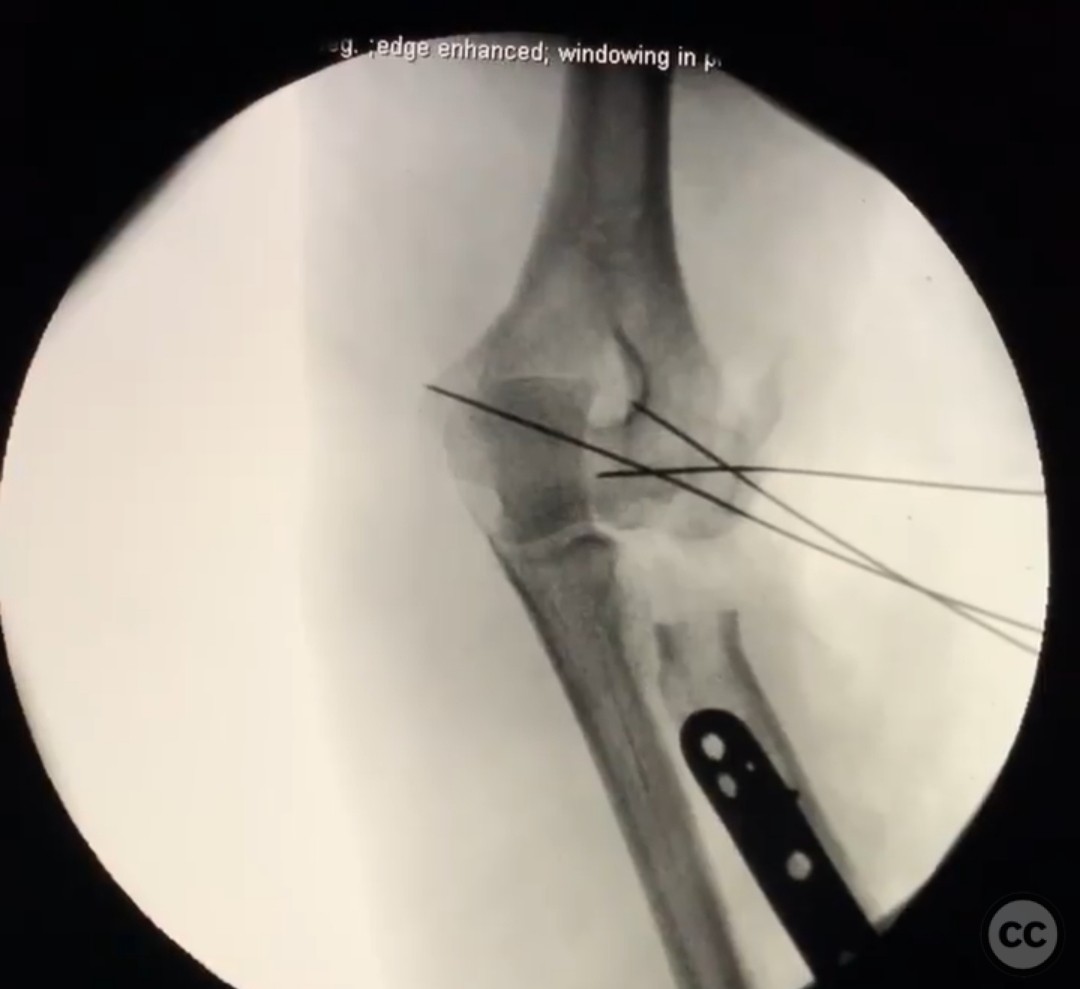
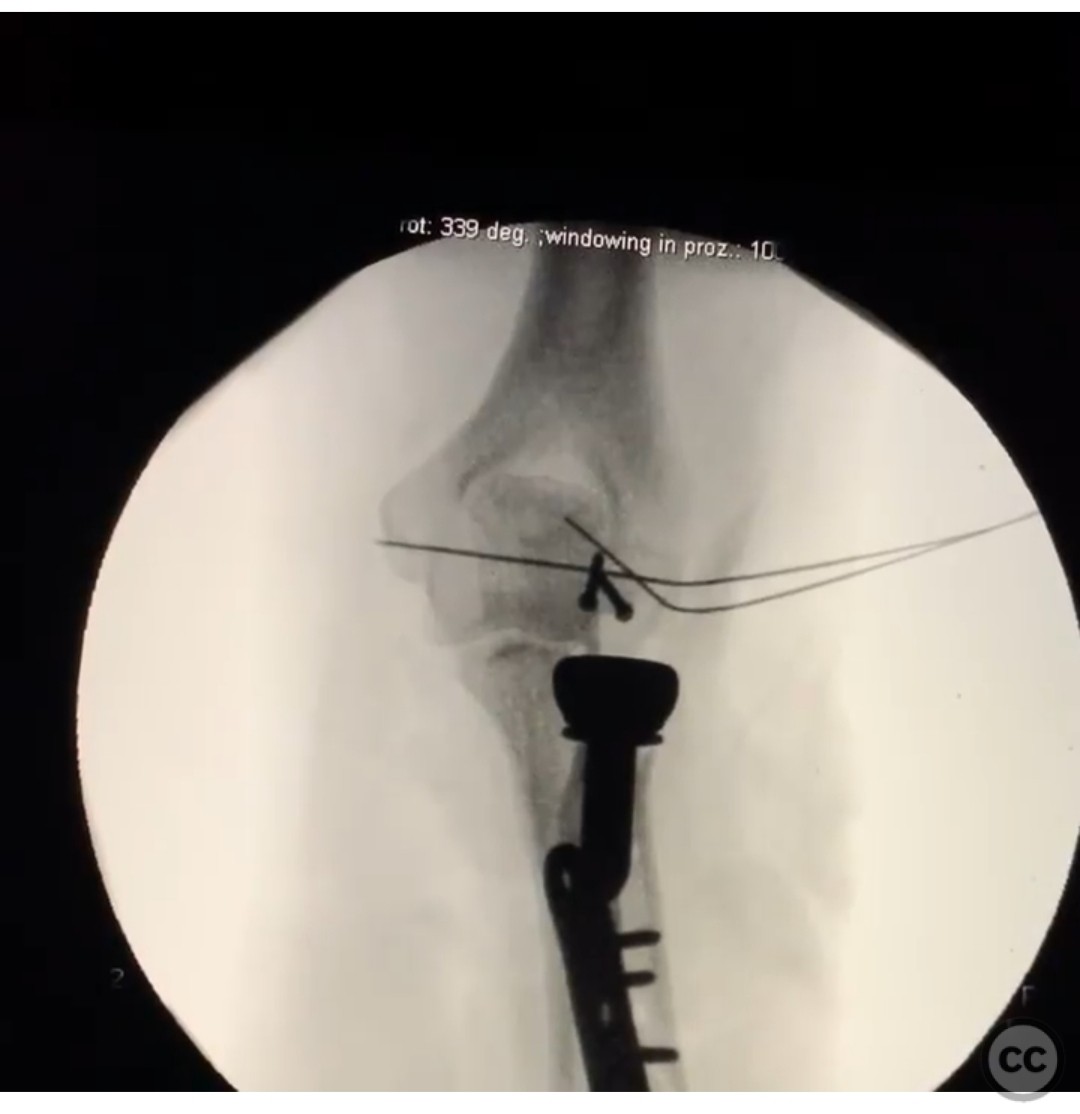
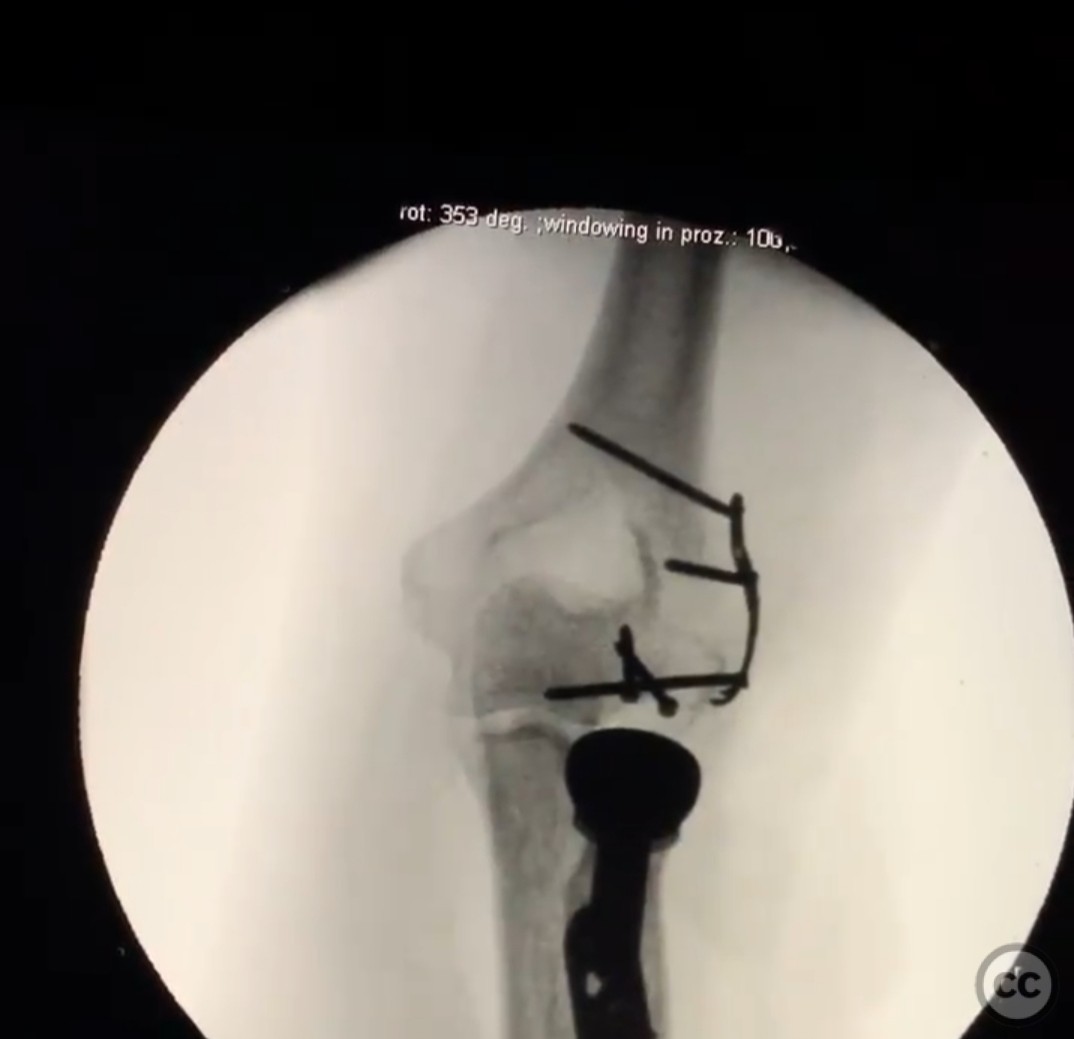
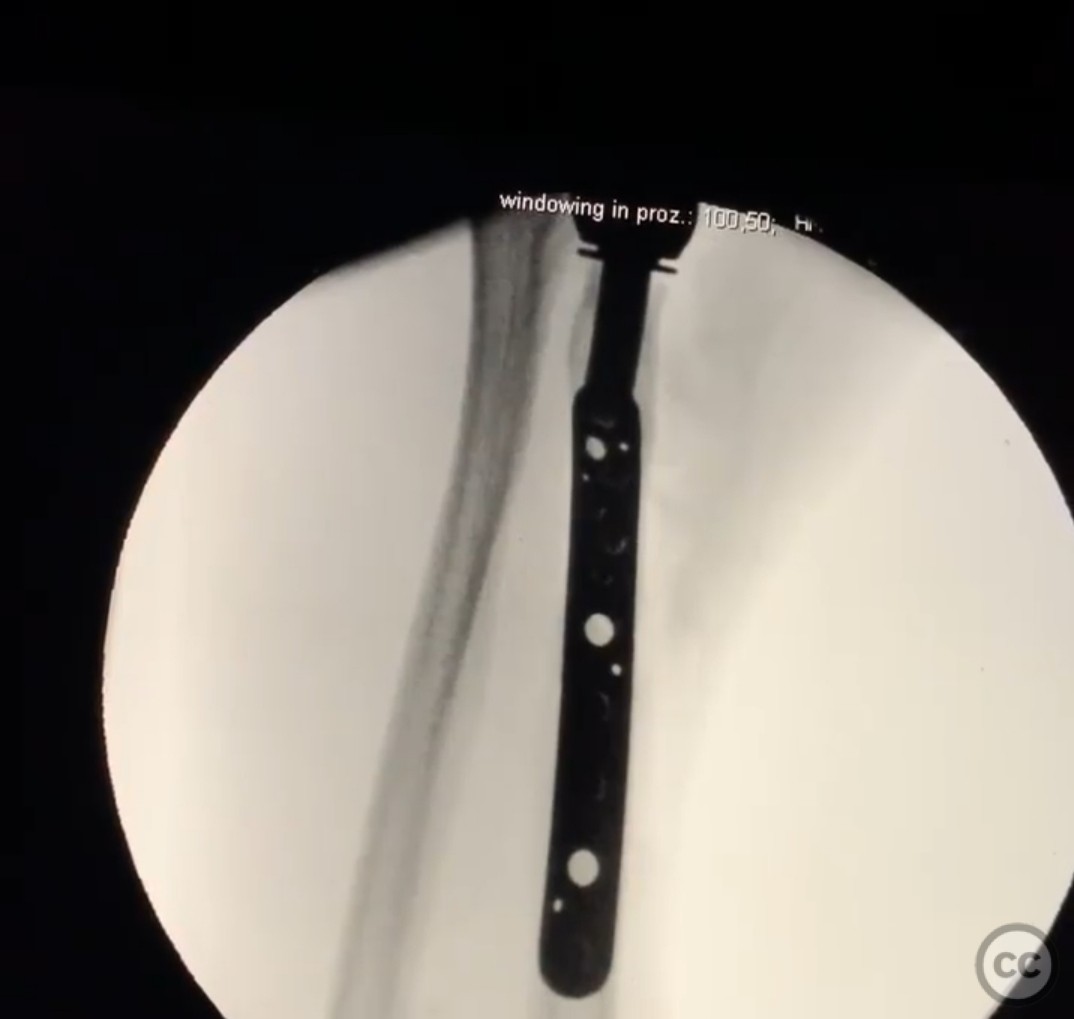
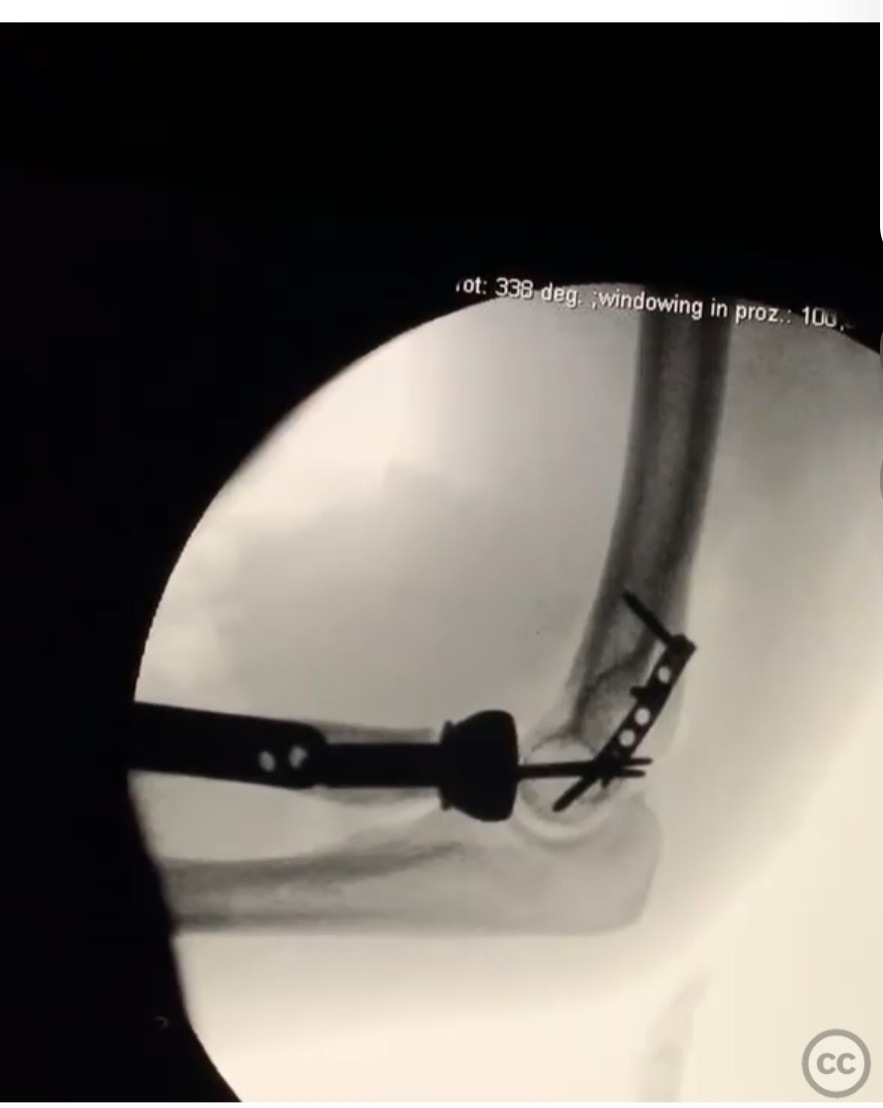
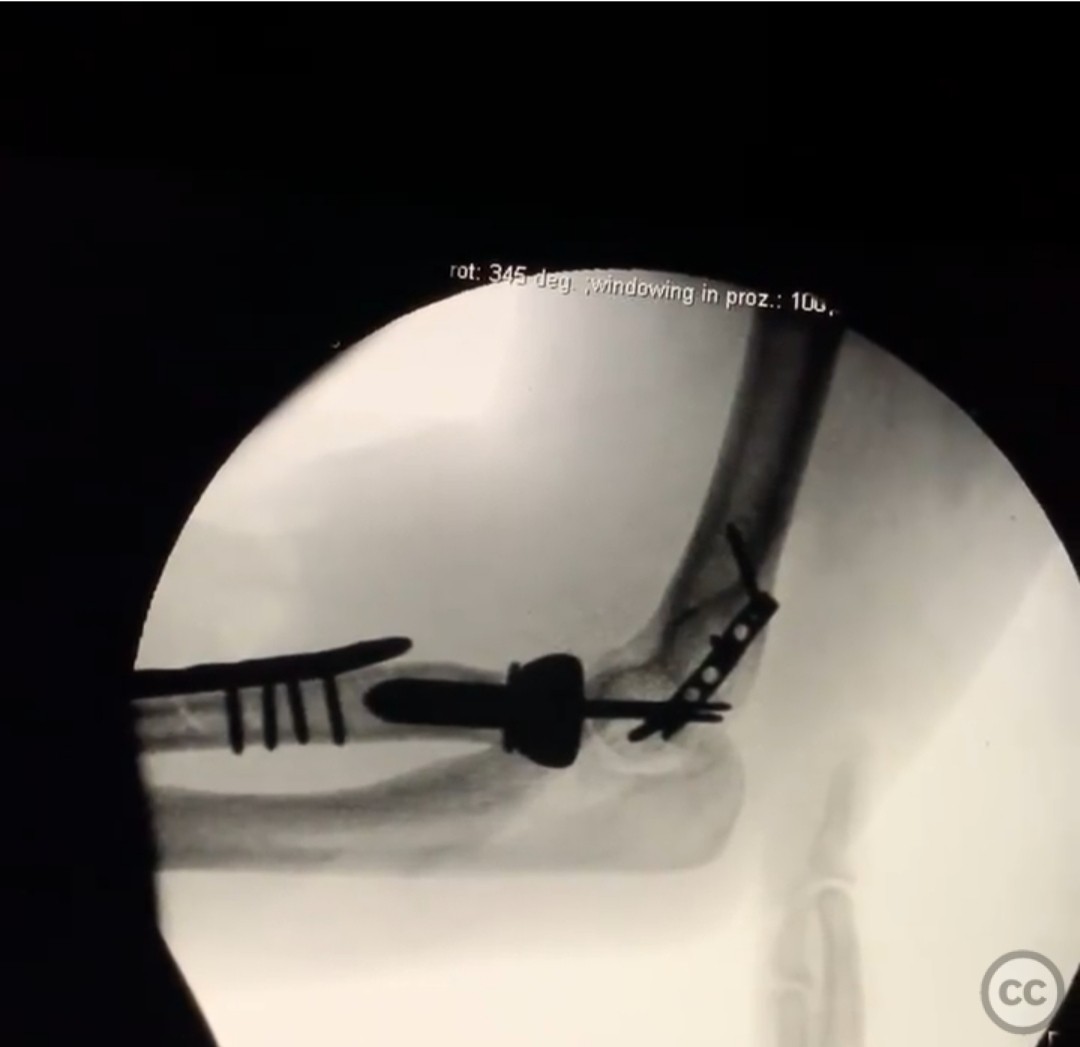
Clinical and radiological findings: A 28-year-old patient involved in a motor vehicle accident with a falling tree, presenting with a complex elbow injury. The injury is not isolated, but the patient is assumed ready for definitive surgical intervention. There is a 1 cm open wound on the distal dorsal forearm, with intact vascular status. The elbow trauma is complex, requiring debridement due to the open wound, compartment release due to tightness, and fixation of a proximal radius fracture with a simple pattern. Additionally, there is a capitellum fracture and considerations for radial head management and ligamentous stability.
Preoperative Plan
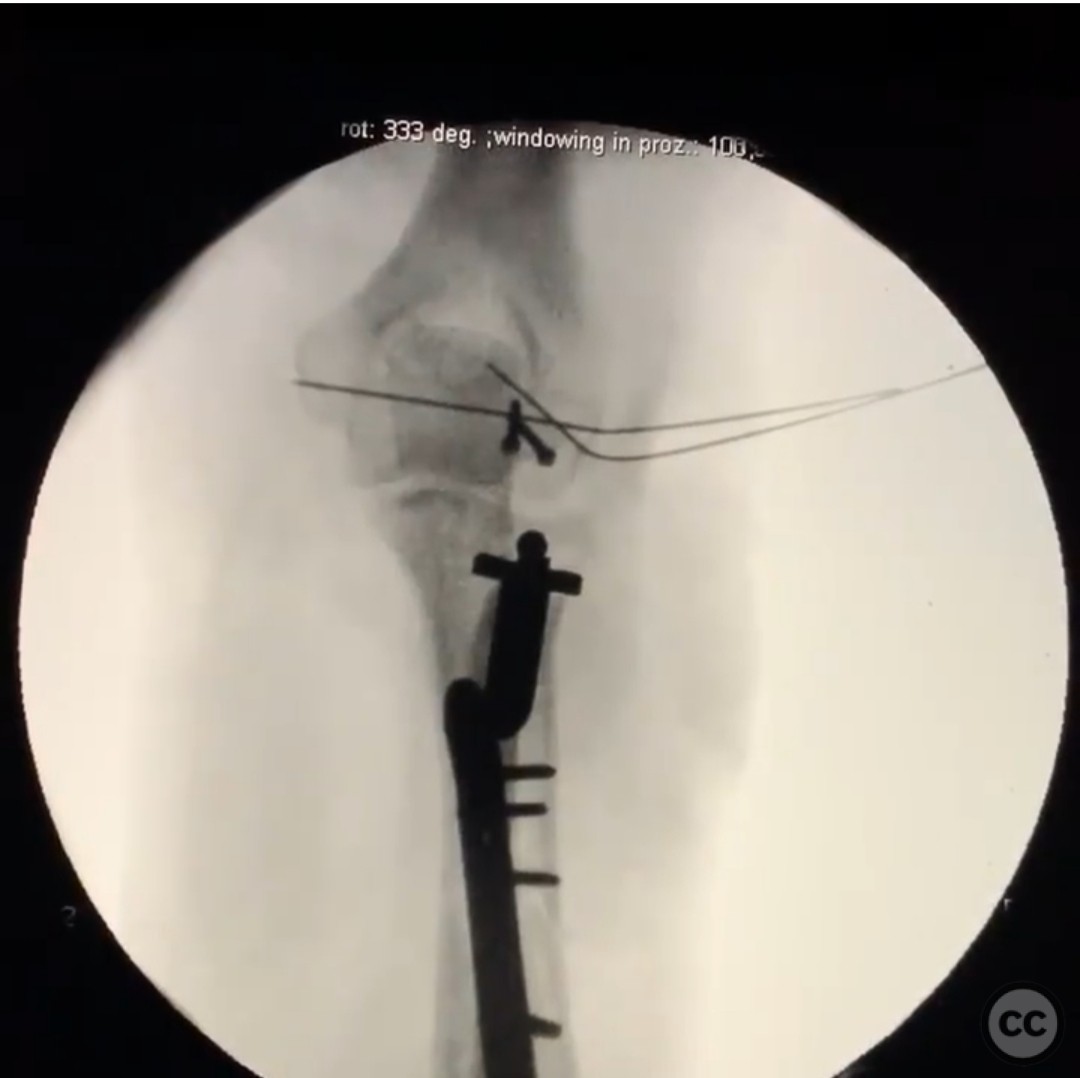
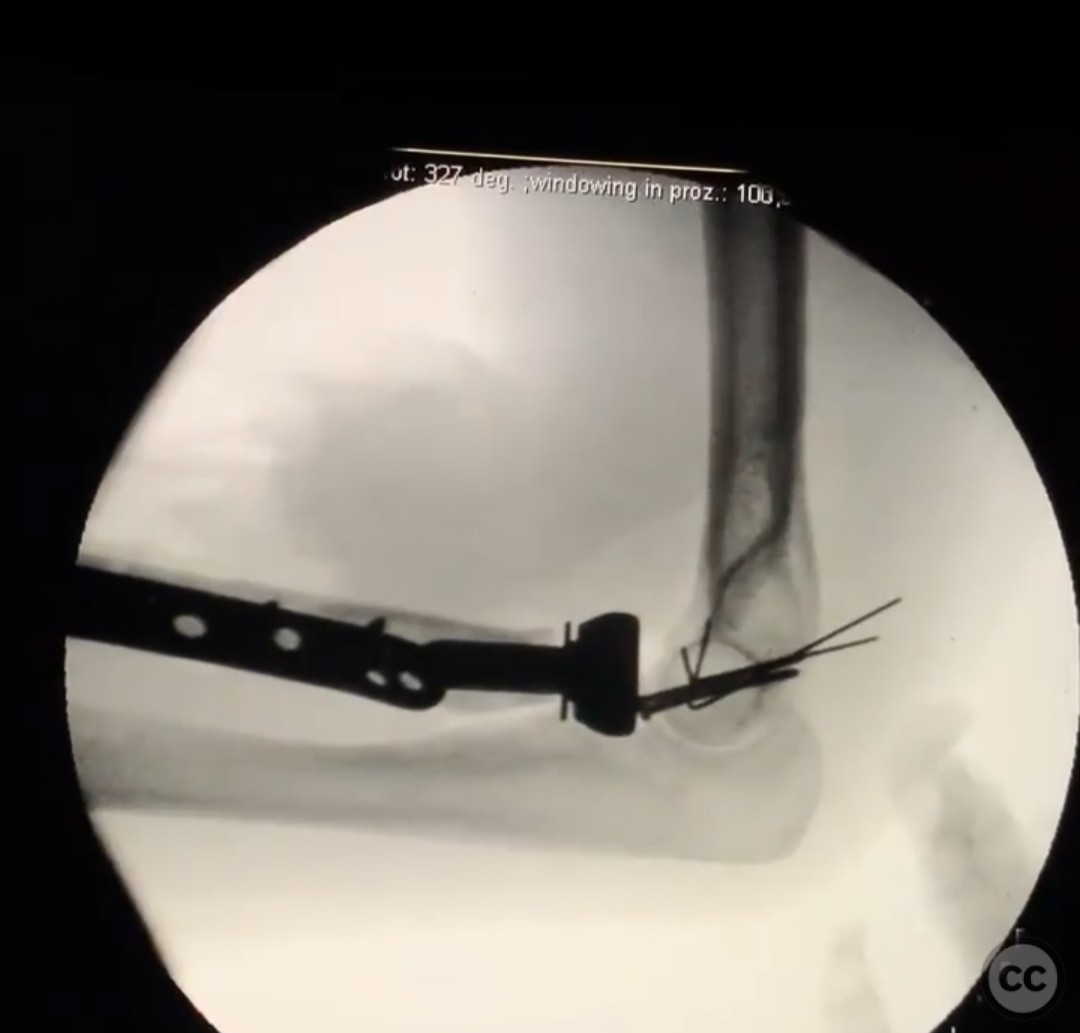
Planning remarks: The preoperative plan involves a volar Henry approach for the proximal radius fracture to achieve compression and absolute stability. For the capitellum fracture, an approach through Kaplan's interval was planned due to a traumatic fascial tent encountered intraoperatively. The radial head was considered for replacement, with careful attention to implant height and size to address multidirectional elbow instability.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the arm placed on an arm board to allow for optimal access to the volar and lateral aspects of the elbow.
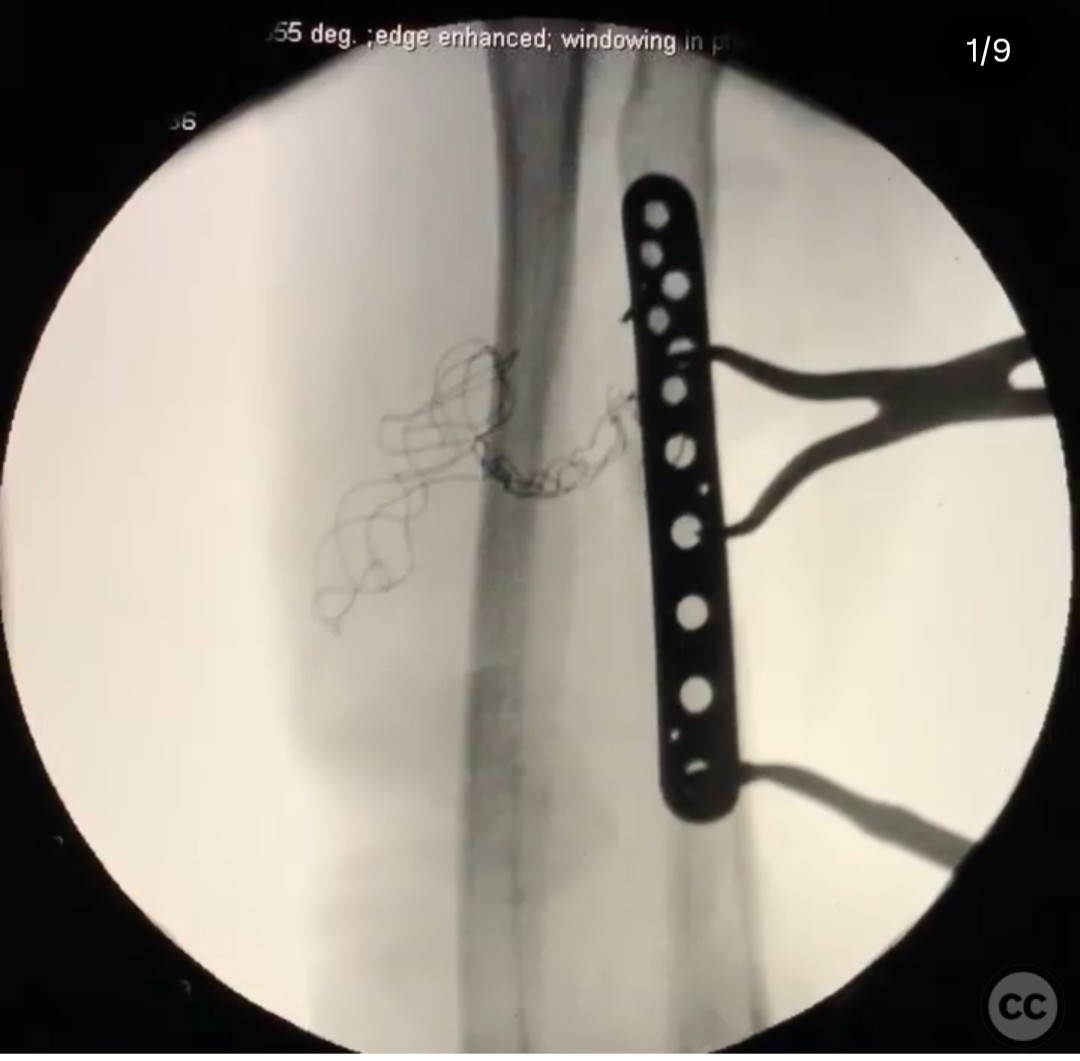
Anatomical surgical approach: The surgical approach commenced with a volar Henry approach to address the proximal radius fracture. This involved an incision along the volar aspect of the forearm, with careful dissection to expose the radius for fixation. Subsequently, Kaplan's interval was utilized for access to the capitellum fracture due to intraoperative findings of a fascial tent, allowing for direct visualization and fixation of the capitellum.
Operative remarks:The surgeon noted the complexity of the case due to the multiple components requiring precise execution for a stable outcome. The sequence of fixation was critical: first addressing the radius, followed by the capitellum, then managing the radial head, and finally addressing ligamentous stability. The radial head replacement posed challenges in terms of implant selection and positioning, particularly in conjunction with the capitellum fracture and elbow instability. The procedure concluded with a stable elbow in full pronation-supination and full extension, which was an unexpected positive outcome given the initial concerns.
Postoperative protocol: Postoperative rehabilitation included early mobilization with emphasis on maintaining range of motion. Weight-bearing restrictions were applied as necessary, with gradual progression based on clinical assessment.
Follow up: Not specified.
Orthopaedic implants used: Radial head prosthesis, internal fixation devices for proximal radius and capitellum fractures (specific implants not detailed).
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 335 times
18 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Elbow Trauma with Proximal Radius Fracture and Capitellum Involvement.. Journal of Orthopaedic Surgery and Traumatology. Case Report 47411002 Published Online Jul 18 2025.