._._._(.jpg)
._._._1.jpg)
























Management of Distal Femur Nonunion with Retrograde Nailing and Plate Retention
Score and Comment on this Case
Clinical Details
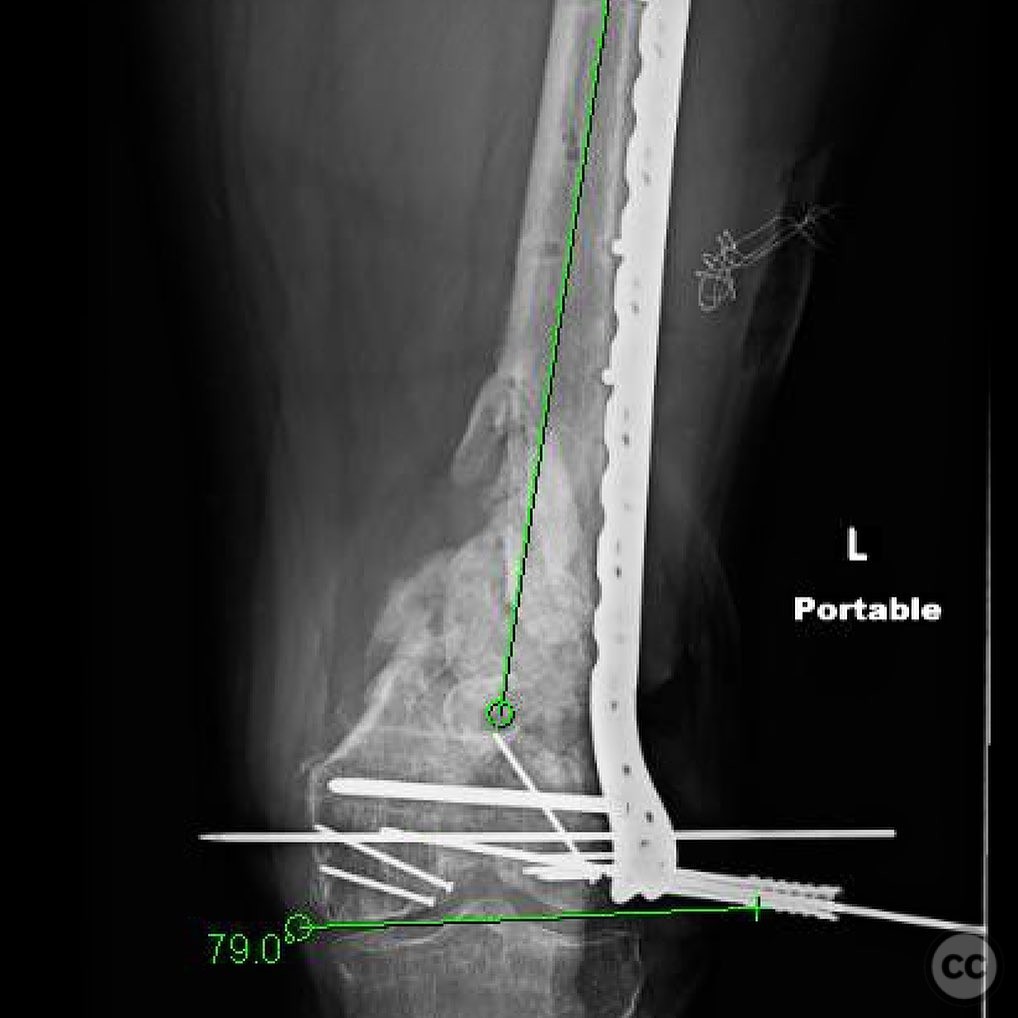
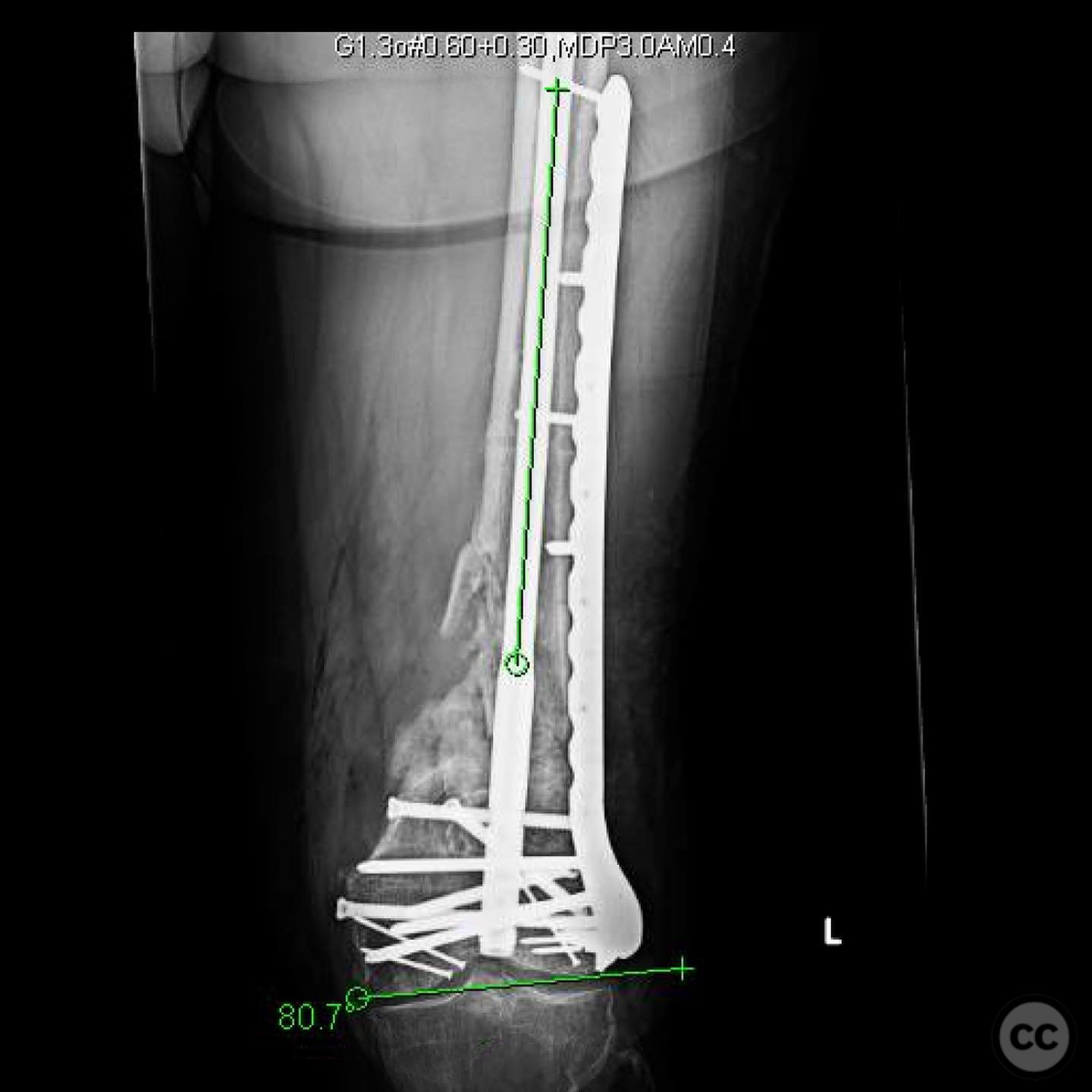
Clinical and radiological findings: A 42-year-old male sustained a Type IIIA open 33C3 distal femur fracture with segmental bone loss after a motorcycle crash. He underwent initial debridement, external fixation, and wound closure. ORIF was performed via lateral arthrotomy with fragment-specific fixation and a cement spacer. At 8 weeks, stage two of the Masquelet technique was done using autograft and allograft. Five months later, he reported mild knee and thigh pain. Imaging showed a broken screw and minimal healing. Labs and cultures were negative. CT confirmed aseptic nonunion with 15° varus and 2.5 cm shortening, necessitating surgical intervention to correct the deformity and achieve union.
Preoperative Plan
Planning remarks: Preoperative planning focused on articular reconstruction through the existing anterolateral wound using a lateral arthrotomy. Key objectives included anatomic reduction of the joint surface, restoration of length, alignment, and rotation (LAR), and preparation for staged reconstruction of the metaphyseal bone defect using the Masquelet technique. Radiographs of the contralateral limb were reviewed preoperatively to guide length restoration. Implant selection included a lateral distal femur locking plate for stabilization, with plans for fragment-specific fixation of small intra-articular pieces and a cement spacer to maintain space and induce membrane formation for later bone grafting.
Surgical Discussion
Patient positioning: Supine position on a radiolucent table, with the affected limb draped freely to allow manipulation and intraoperative imaging.
Anatomical surgical approach: A lateral approach to the distal femur was utilized, involving exposure of the existing plate. The distal screws were removed to facilitate deformity correction. The femoral canal was accessed retrograde through the intercondylar notch for nail insertion.
Operative remarks:The plan was to remove the distal screws and assess whether the deformity could be corrected without fully removing the plate. Upon removal, alignment was restored with relative ease. The plate was temporarily secured with wires, and proximal screws were exchanged for uniaxial screws to optimize fixation. Intraoperative imaging confirmed satisfactory alignment. Short locking screws were placed distally, and a retrograde nail was inserted. The central bone graft mass was drilled using a DHS drill, followed by RIA reaming to harvest autograft, which was then packed medially
Postoperative protocol: Postoperative protocol included weight-bearing as tolerated with progressive mobilization. Emphasis was placed on early range of motion exercises to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Retrograde femoral nail, uniaxial screws, locking screws, Reamer-Irrigator-Aspirator (RIA) system for autograft harvesting.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 370 times
19 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Management of Distal Femur Nonunion with Retrograde Nailing and Plate Retention. Journal of Orthopaedic Surgery and Traumatology. Case Report 46874248 Published Online Jul 19 2025.