










Combined Pelvic Ring and Transverse Acetabulum Fracture with Bladder Injury
Score and Comment on this Case
Clinical Details
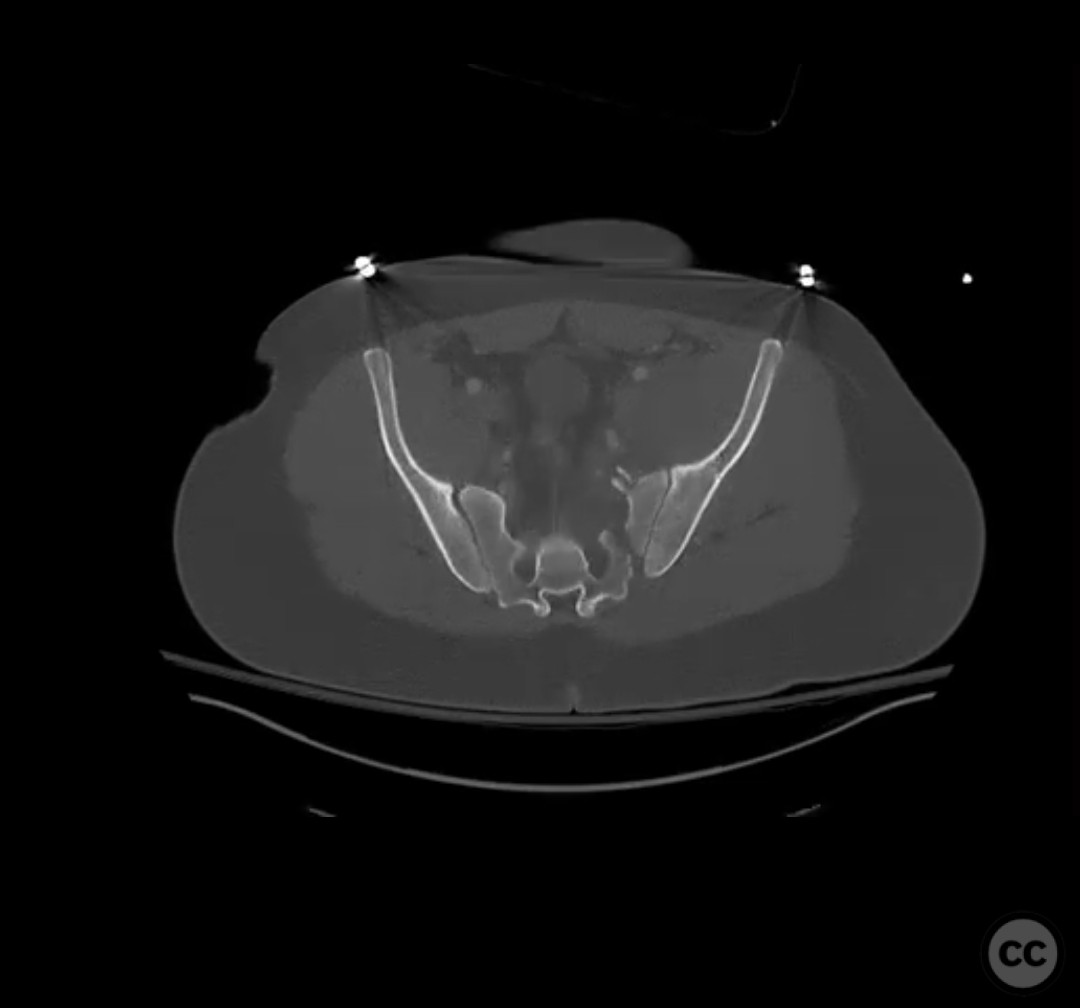
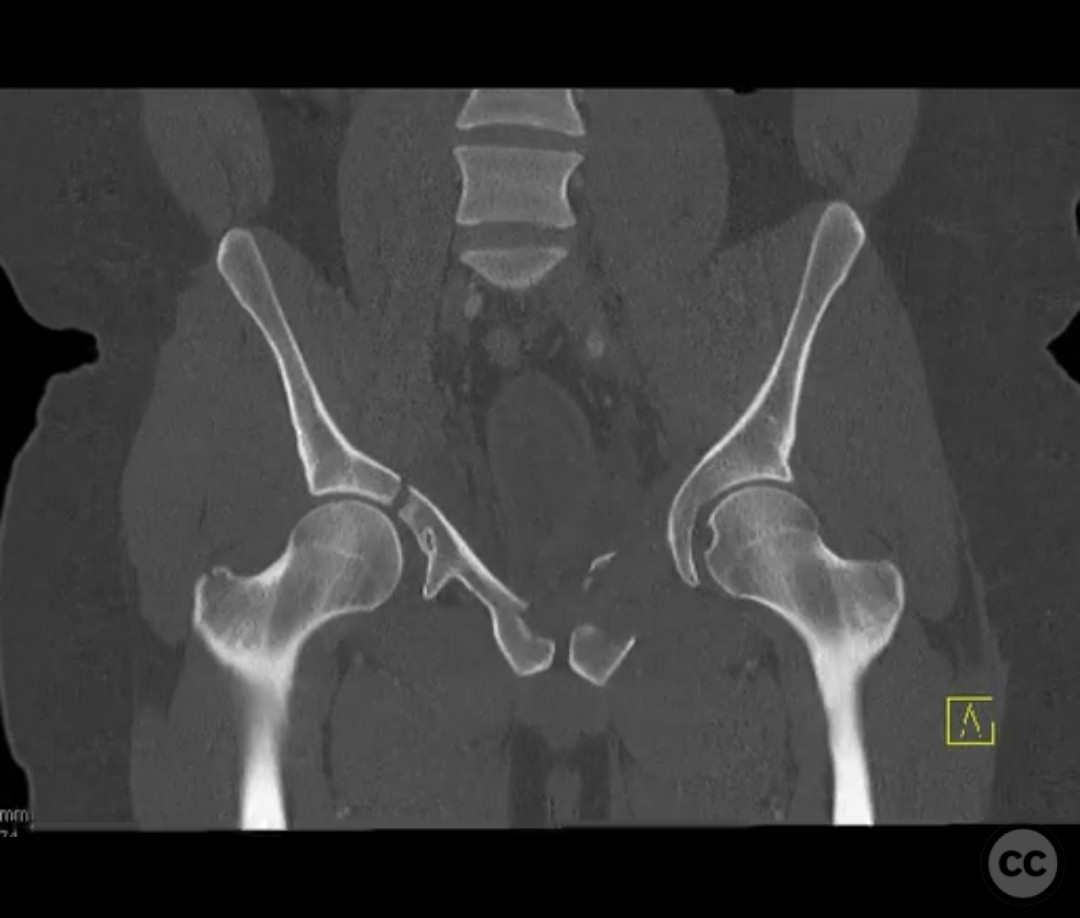
Clinical and radiological findings: The patient presented with a highly unstable pelvic ring injury and a transverse acetabulum fracture, accompanied by a bladder injury. The bladder injury was addressed emergently with a low vertical midline Pfannenstiel incision for repair, followed by the placement of a low right-sided suprapubic catheter. Radiological imaging confirmed the transverse acetabular fracture and disruption of the left sacroiliac joint, along with a displaced sacral fracture.
Preoperative Plan
Planning remarks: The preoperative plan involved a staged approach to address the combined injuries. Initially, the focus was on stabilizing the pelvic ring to provide a stable base for subsequent acetabular reconstruction. The left sacroiliac joint disruption was to be reduced and stabilized first, followed by lag screw fixation of the displaced sacral fracture. Additional screws were planned as anatomical corridors allowed. An external fixator was considered to support the posterior ring stabilization. The second stage involved open reduction and internal fixation (ORIF) of the acetabulum through a Kocher-Langenbeck approach, with potential anterior column fixation via the modified Stoppa approach if necessary.
Surgical Discussion
Patient positioning: The patient was positioned supine for the initial stage of pelvic ring stabilization.
Anatomical surgical approach: For the pelvic ring stabilization, a posterior approach was employed to access the left sacroiliac joint and sacral fracture. In the second stage, a Kocher-Langenbeck approach was planned for acetabular ORIF, with potential anterior column access through a modified Stoppa approach.
Operative remarks:The surgical team emphasized the importance of achieving an anatomical reduction of the acetabulum while ensuring stable fixation of the pelvic ring. The presence of the suprapubic catheter necessitated careful planning to avoid interference with surgical access and fixation. The decision to prioritize pelvic ring stabilization first was based on providing a stable segment for accurate acetabular reconstruction. Intraoperative challenges included ensuring precise screw trajectory for sacral fracture fixation and managing potential displacement during reduction maneuvers.
Postoperative protocol: Postoperative rehabilitation included initial non-weight bearing on the affected side, with gradual progression to partial weight bearing as tolerated. Range of motion exercises were initiated early to prevent joint stiffness, with emphasis on avoiding stress on the surgical repairs.
Follow up: Not specified
Orthopaedic implants used: Lag screws for sacroiliac joint and sacral fracture fixation, external fixator for posterior ring stabilization, potential plate and screw constructs for acetabular ORIF through Kocher-Langenbeck and modified Stoppa approaches.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 387 times
10 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Combined Pelvic Ring and Transverse Acetabulum Fracture with Bladder Injury. Journal of Orthopaedic Surgery and Traumatology. Case Report 46644504 Published Online Jul 10 2025.