

Complex Proximal Radius and Segmental Ulna Fracture Management
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A patient presented with a complex forearm injury involving a proximal radius fracture and a segmental ulna fracture. The injury films indicated the need for surgical intervention. The AO/OTA classification for the proximal radius fracture is 21-A2, and the segmental ulna fracture is classified as 22-B3. The clinical examination revealed no neurovascular compromise.
Preoperative Plan
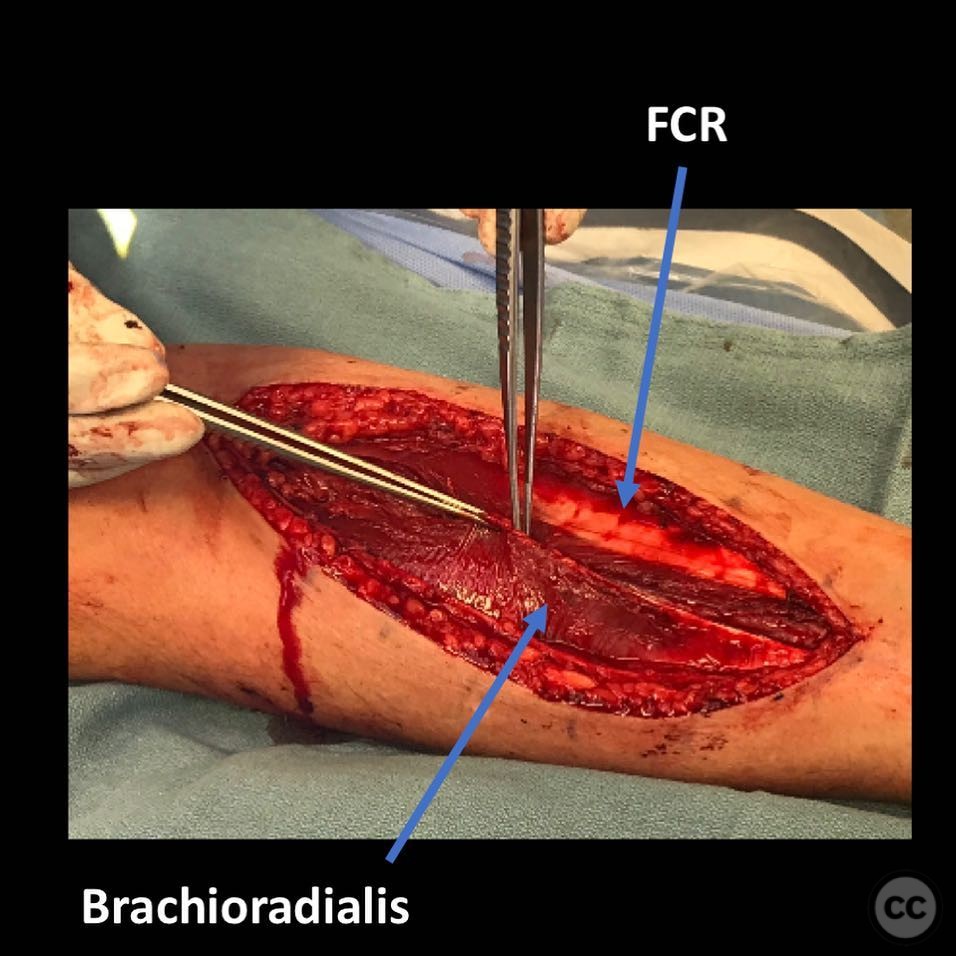
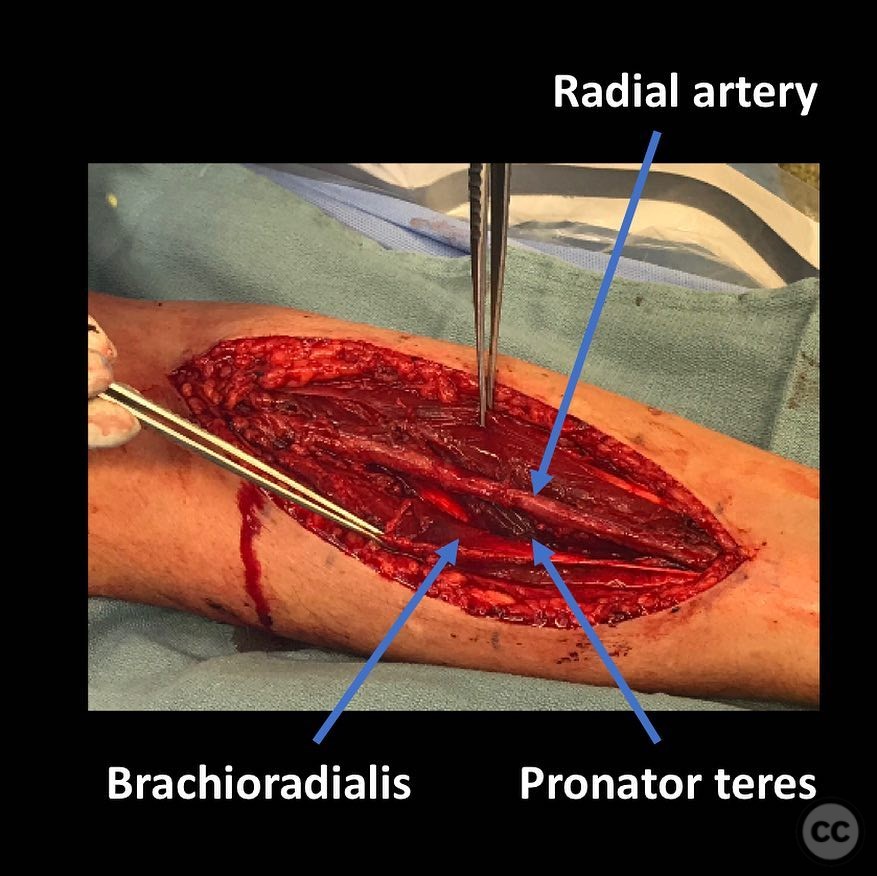
Planning remarks: The preoperative plan involved using the volar Henry approach for the proximal radius, exploiting the interval between the radial artery and brachioradialis. The plan included sparing the pronator teres and carefully elevating the supinator from the ulnar border of the radius with the proximal segment fully supinated to protect the posterior interosseous nerve (PIN). For the ulna, both proximal and distal segments were planned for surgical fixation.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the arm placed on an arm board to allow for optimal access to the forearm.
Anatomical surgical approach: A volar Henry approach was utilized, involving an incision along the radial aspect of the forearm. The interval between the radial artery and brachioradialis was exploited, with careful protection of the radial nerve. The supinator muscle was elevated from the ulnar border of the radius while maintaining full supination of the proximal segment to avoid injury to the PIN. The ulna was approached through a separate incision, allowing for direct access to both fracture sites.
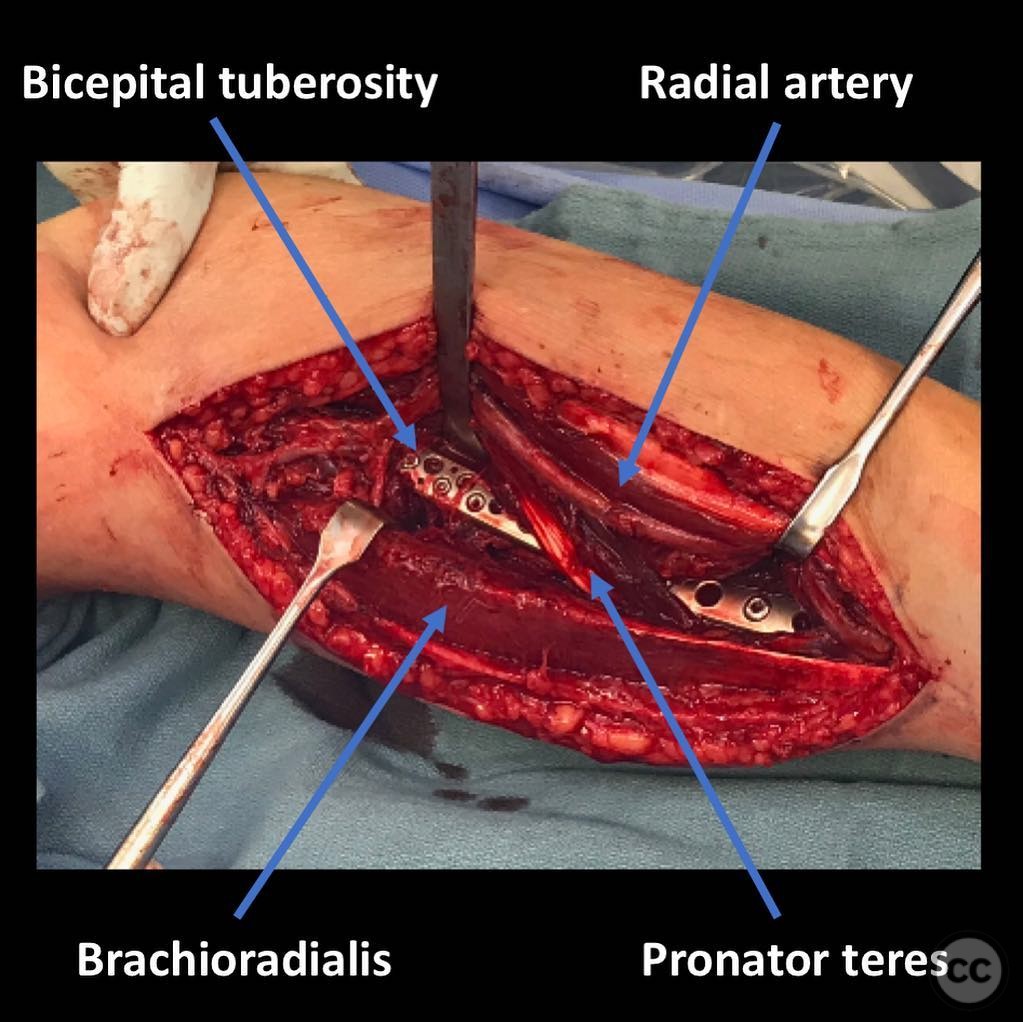
Operative remarks:Intraoperatively, it was noted that plating up to the bicipital tuberosity required precise anatomical knowledge to avoid complications. The segmental nature of the ulna fracture necessitated careful alignment and fixation of both segments to restore forearm stability.
Postoperative protocol: Postoperative rehabilitation included immobilization in a splint for 2 weeks, followed by gradual range of motion exercises. Weight-bearing activities were restricted for 6 weeks, with progressive strengthening exercises introduced thereafter.
Follow up: Not specified
Orthopaedic implants used: Volar locking plate for proximal radius, dual plating for segmental ulna fracture.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 403 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Proximal Radius and Segmental Ulna Fracture Management. Journal of Orthopaedic Surgery and Traumatology. Case Report 46366806 Published Online Jul 21 2025.