 ☠️ Lets go _bread and butte_3.jpg)
 ☠️ Lets go _bread and butte_4.jpg)
 ☠️ Lets go _bread and butte_2.jpg)
 ☠️ Lets go _bread and butte_1.jpg)
 ☠️ Lets go _bread and butter(.jpg)




Forearm Fractures of Necessity: A Triad of Instability in Adults
Score and Comment on this Case
Clinical Details
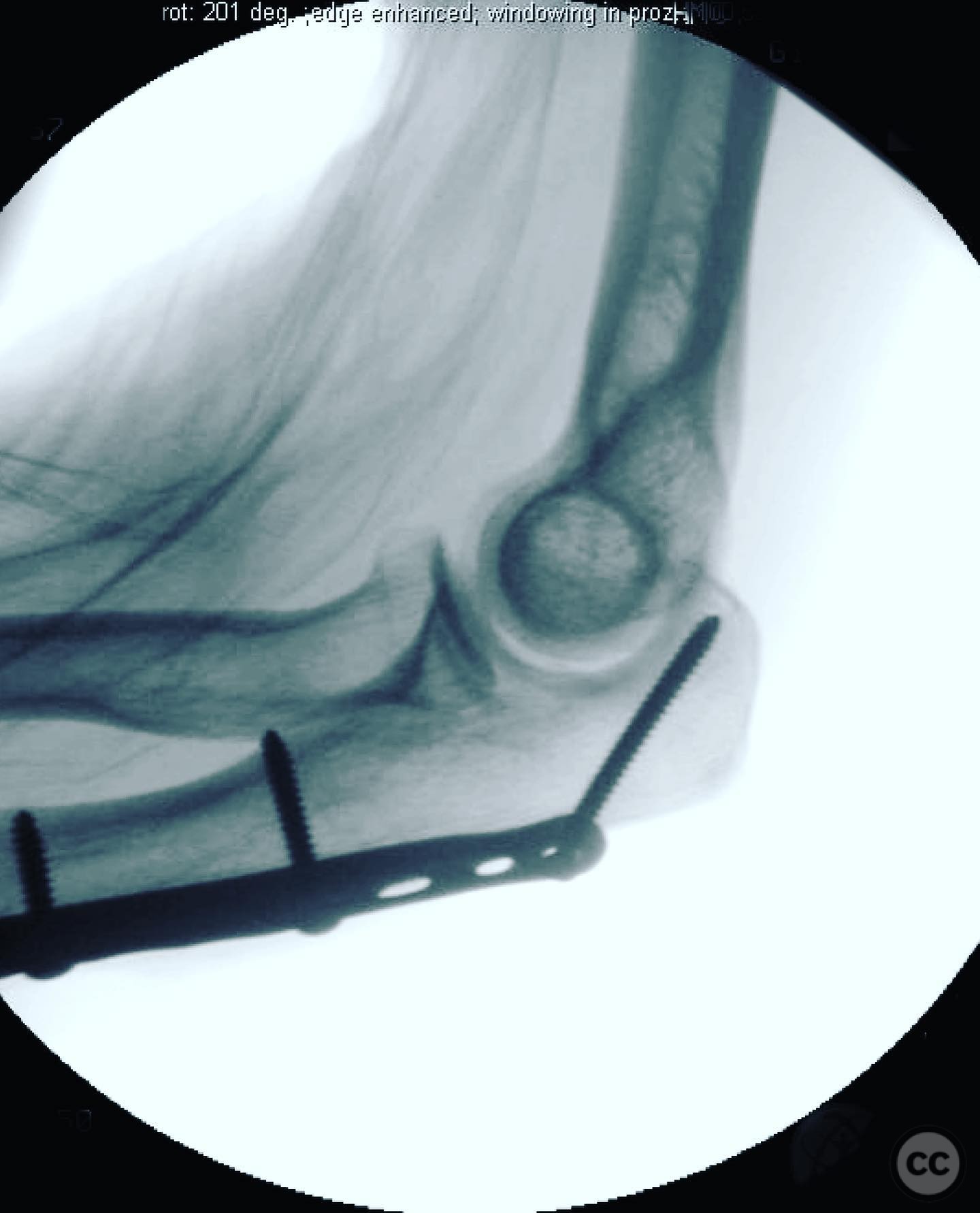
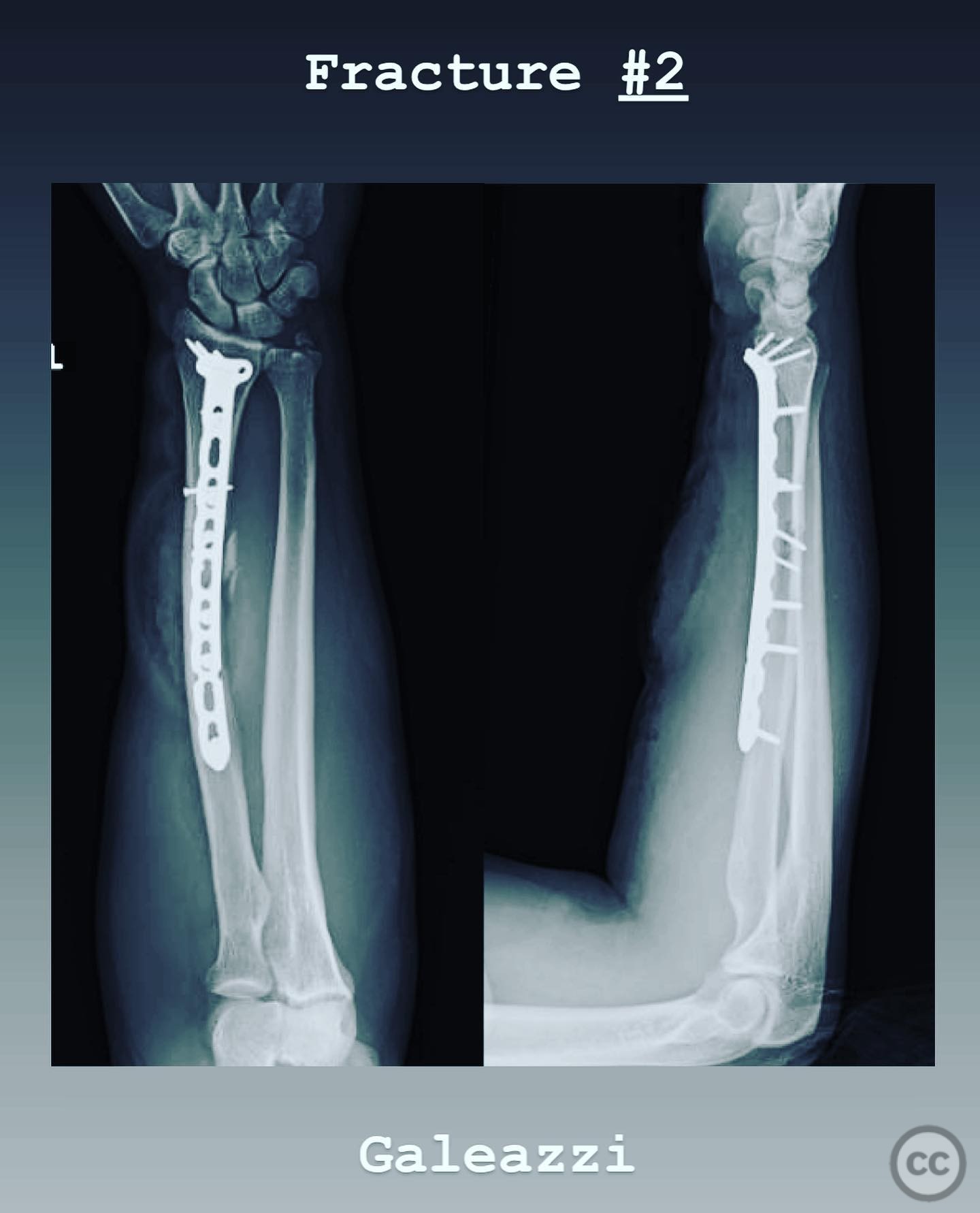
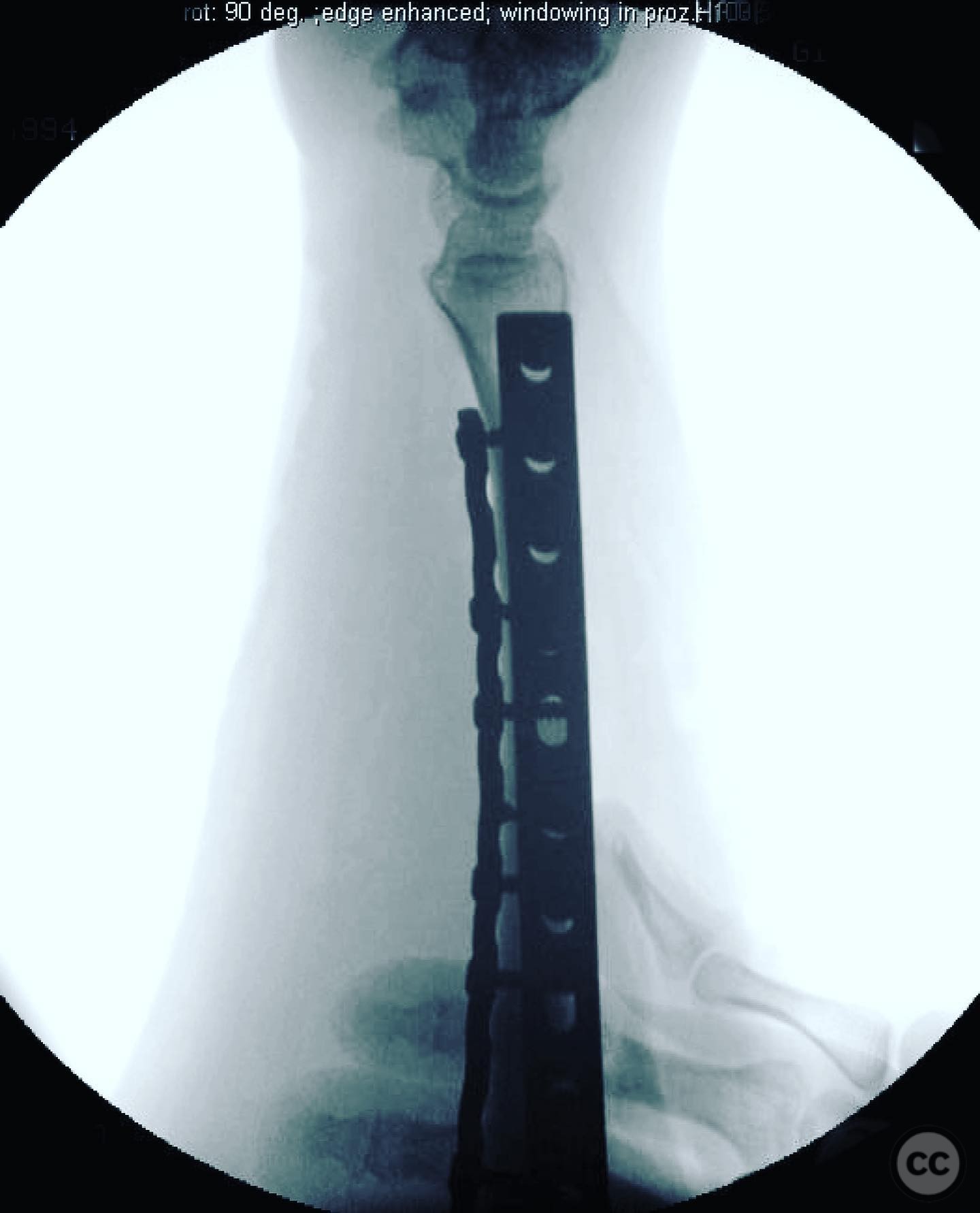
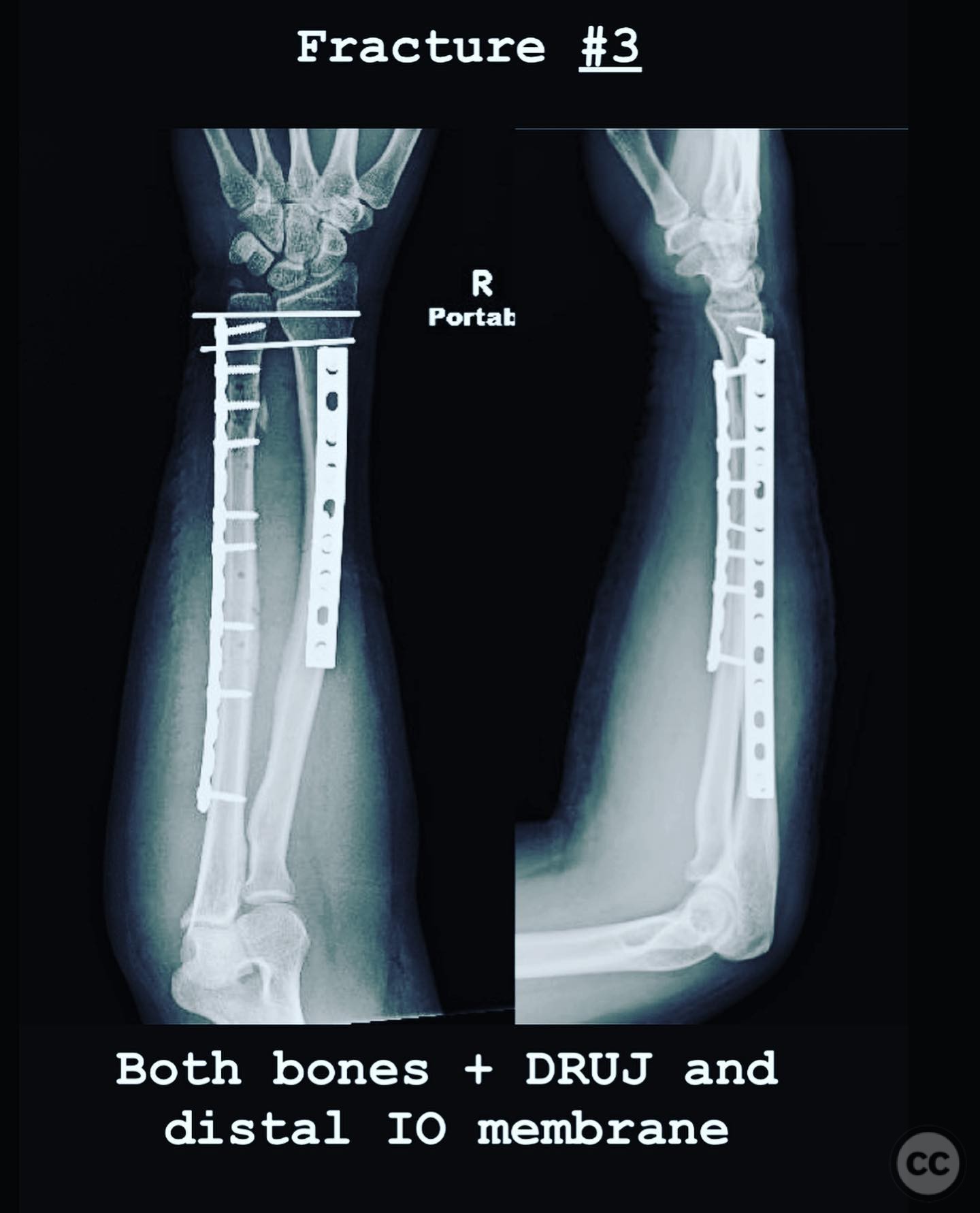
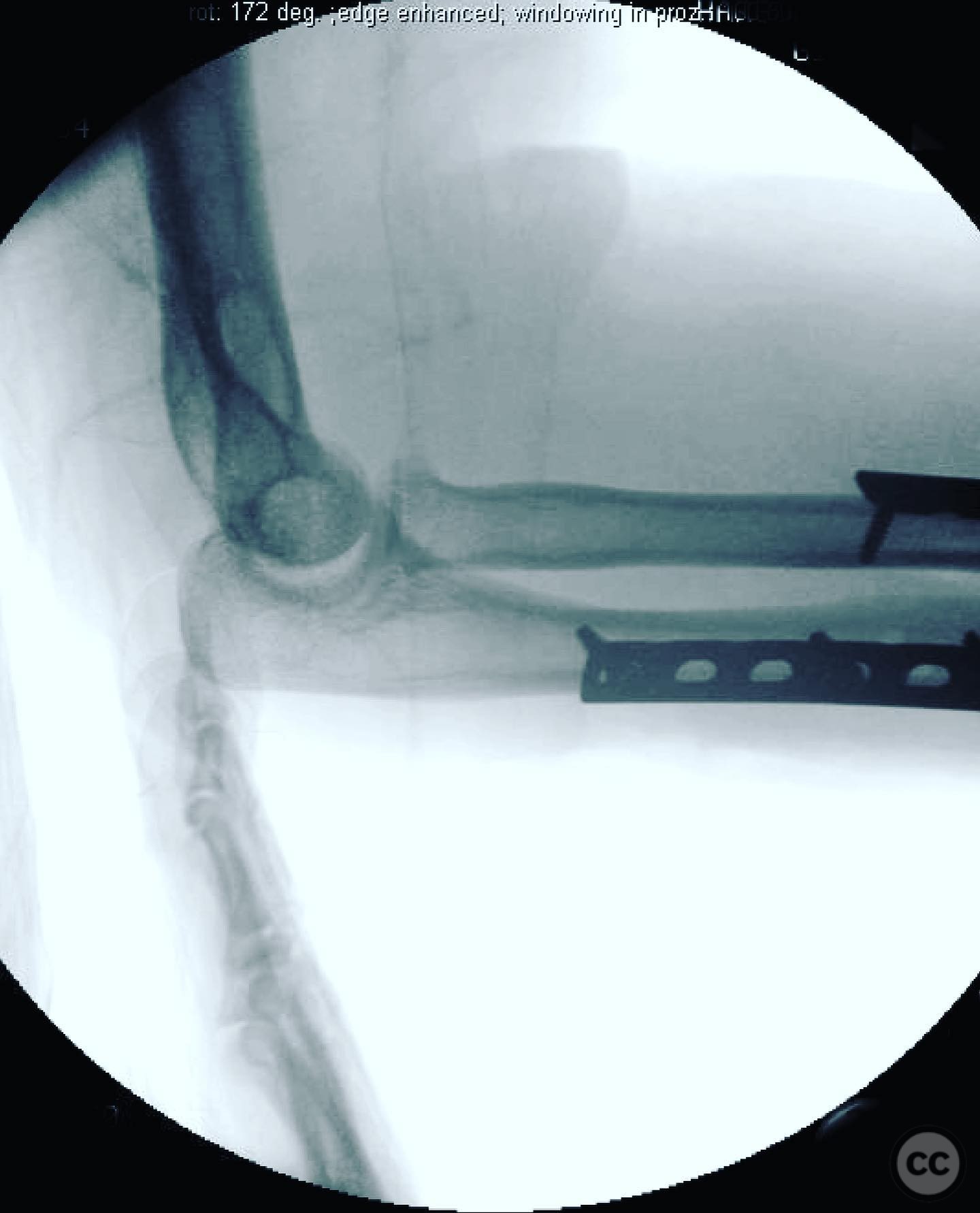
Clinical and radiological findings: Three adult patients presented with forearm injuries, each demonstrating instability akin to a "ring" failure. Case 1 involved a proximal ulna fracture with radiocapitellar joint dislocation and proximal radioulnar joint (PRUJ) disruption, classified as Bado Type I. Case 2 presented with a distal one-third radius fracture and distal radioulnar joint (DRUJ) instability. Case 3 was a high-energy injury with both forearm bones fractured, including a displaced ulnar segment and styloid fracture, raising suspicion for an Essex-Lopresti injury. Radiological assessment confirmed the respective fracture patterns and joint instabilities.
Preoperative Plan
Planning remarks: For Case 1, the plan involved anatomical reduction of the ulna to achieve radiocapitellar joint reduction, with potential repair of the lateral ulnar collateral ligament (LUCL) if required. Case 2 required anatomical fixation of the radius to assess DRUJ stability post-fixation. In Case 3, anatomical fixation of both bones was planned, with cross pinning of the DRUJ due to instability.
Surgical Discussion
Patient positioning: Supine positioning was utilized for all cases, with the affected arm placed on a radiolucent arm table to facilitate intraoperative imaging and manipulation.
Anatomical surgical approach: For Case 1, a posterior approach to the elbow was employed, allowing access to the proximal ulna and radiocapitellar joint. Case 2 involved a volar approach to the distal radius. In Case 3, a dual approach was necessary: a volar approach for the radius and a separate incision for the ulna.
Operative remarks:In Case 1, despite anatomical reduction of the ulna, persistent instability necessitated LUCL repair to stabilize the elbow. Case 2's DRUJ remained stable post-radius fixation, negating further intervention. In Case 3, significant DRUJ instability post-fixation required cross pinning in neutral pronation/supination using 2.0mm K-wires, left proud for easy retrieval if breakage occurred.
Postoperative protocol: Postoperative rehabilitation for Case 1 included early mobilization with elbow range of motion exercises while protecting the LUCL repair. Case 2 involved splinting in full supination for six weeks to maintain DRUJ stability. Case 3 required immobilization in neutral rotation with gradual range of motion exercises initiated after wire removal.
Follow up: Not specified.
Orthopaedic implants used: Orthopaedic implants used included: - Case 1: Plates and screws for ulna fixation, suture anchors for LUCL repair. - Case 2: Volar locking plate for radius fixation. - Case 3: Plates and screws for both bones, 2.0mm K-wires for DRUJ stabilization.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 391 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Forearm Fractures of Necessity: A Triad of Instability in Adults. Journal of Orthopaedic Surgery and Traumatology. Case Report 45307508 Published Online Jul 14 2025.