




Bicondylar Tibial Plateau Fracture with Pre-existing Knee Arthritis
Score and Comment on this Case
Clinical Details
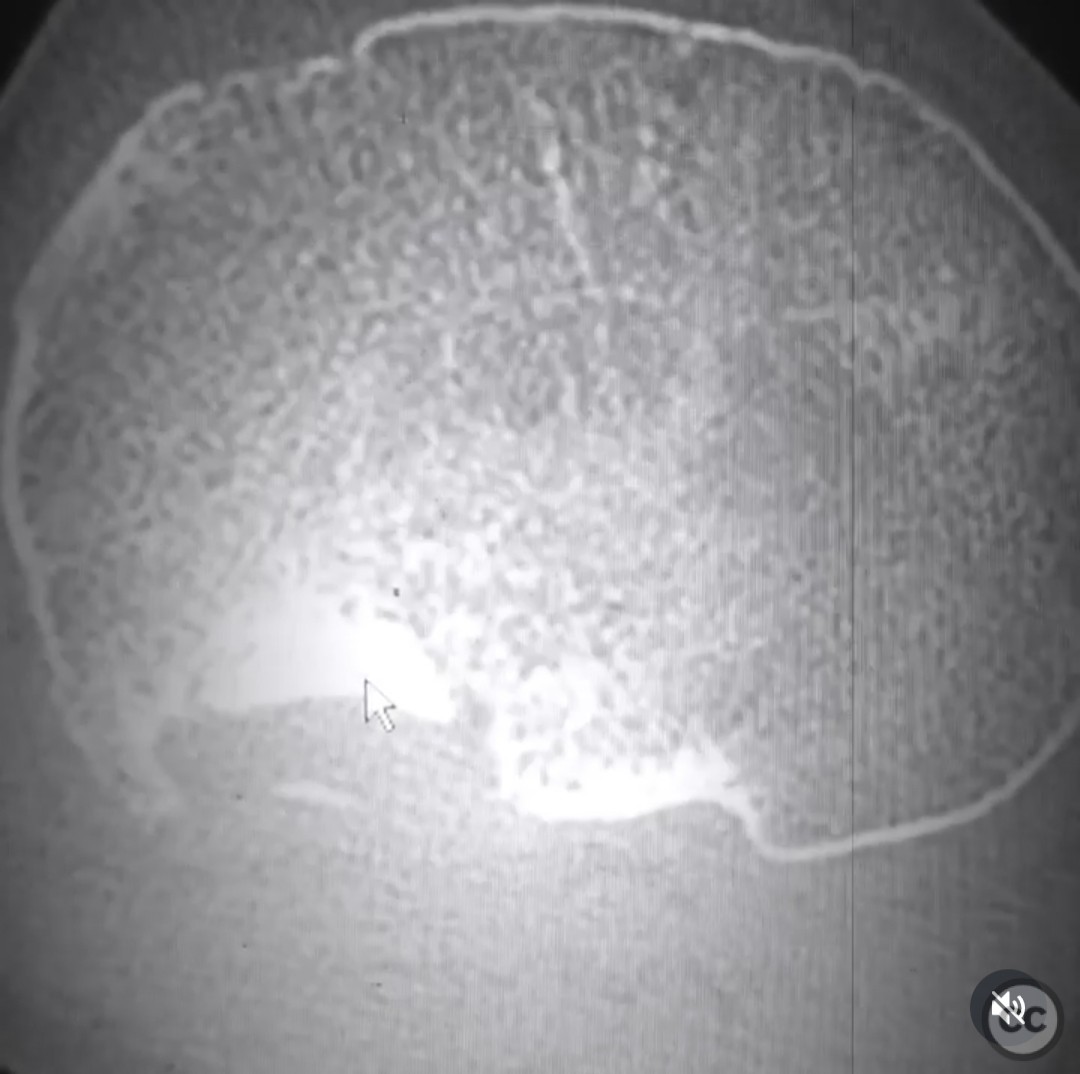
Clinical and radiological findings: A 48-year-old male with a history of knee arthritis sustained a bicondylar tibial plateau fracture while skiing. Initial CT imaging revealed significant articular impaction, particularly involving the posterior lateral tibial plateau. The patient exhibited pre-existing arthritic changes in the knee joint. Intraoperative fluoroscopic guidance was utilized to achieve radiographic reduction of the articular fragments.
Preoperative Plan
Planning remarks: The preoperative plan involved a dual approach to address both the articular and metaphyseal components of the fracture. The articular fragments were to be anatomically reduced and stabilized using subchondral wires and raft screws. For the metaphyseal fracture, an intramedullary (IM) nail was considered to provide relative stability and promote secondary bone healing.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected leg draped freely to allow for intraoperative manipulation and fluoroscopic imaging.
Anatomical surgical approach: A combined anterolateral and posteromedial approach was utilized to access the tibial plateau. The anterolateral approach involved a longitudinal incision over the lateral aspect of the knee, with careful dissection to expose the lateral tibial plateau. The posteromedial approach provided access to the medial plateau, allowing for comprehensive management of the bicondylar fracture.
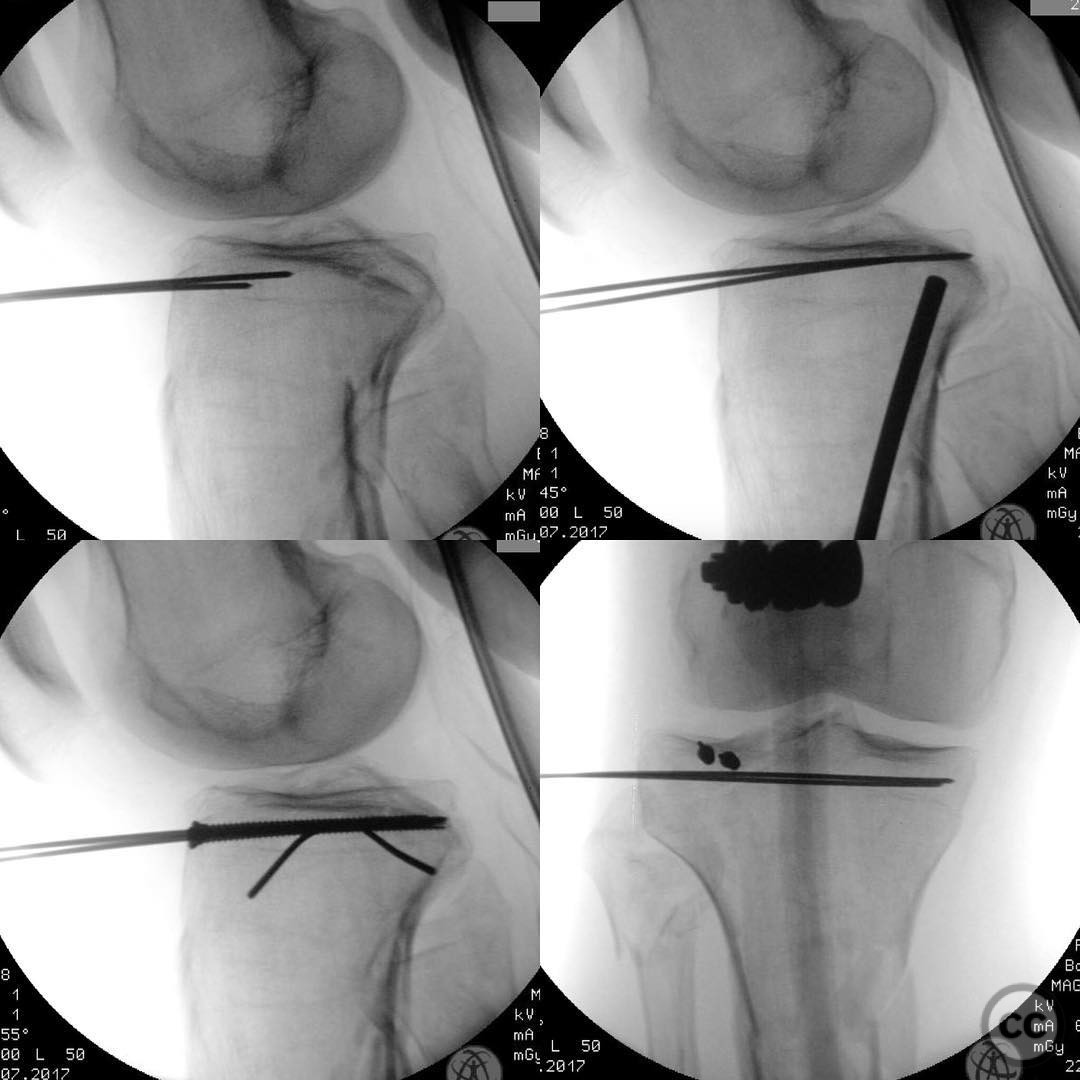
Operative remarks:Intraoperative reduction of the posterior lateral tibial plateau was achieved using a tamp under fluoroscopic guidance. Subchondral wires were pre-positioned to provisionally fix the elevated fragments, followed by placement of raft screws for definitive fixation. The metaphyseal component was managed with an IM nail, chosen for its biomechanical equivalence to dual column plating and its advantage in preserving soft tissue integrity.
Postoperative protocol: Postoperatively, immediate knee range of motion exercises were initiated. Partial weight-bearing was commenced at 4 weeks, with progressive weight-bearing as tolerated, adhering to AO principle 4 of early motion.
Follow up: Not specified.
Orthopaedic implants used: Subchondral wires, raft screws, intramedullary nail.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 321 times
28 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Bicondylar Tibial Plateau Fracture with Pre-existing Knee Arthritis. Journal of Orthopaedic Surgery and Traumatology. Case Report 43014461 Published Online Jul 28 2025.