

Percutaneous Screw Fixation for Pelvic Ring Instability in an Elderly Female
Score and Comment on this Case
Clinical Details
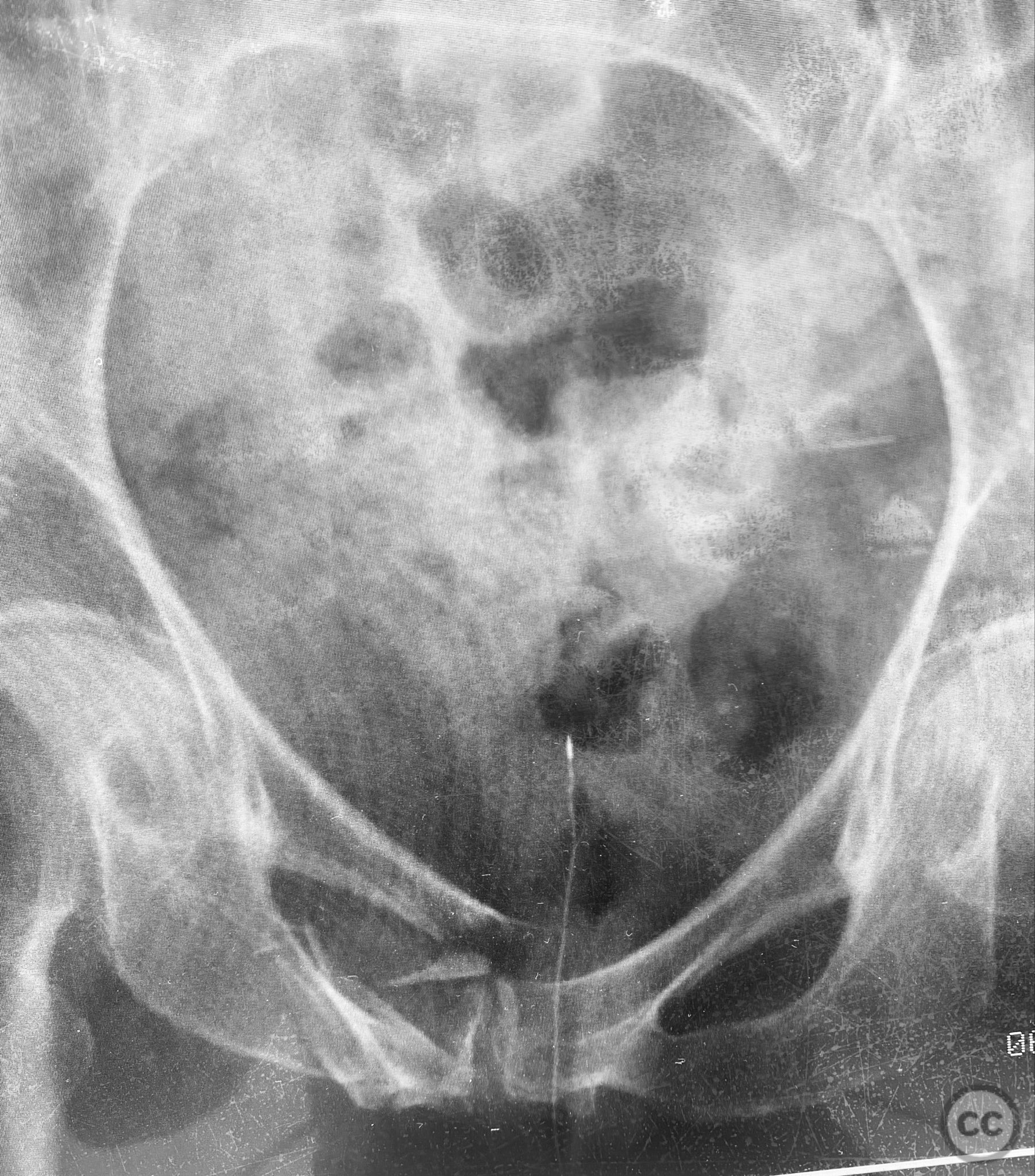
Clinical and radiological findings: An 83-year-old previously healthy and active female sustained a fall resulting in severe pelvic pain and inability to mobilize. Clinical examination revealed marked pelvic tenderness and functional impairment. Radiological assessment, including examination under anesthesia with fluoroscopy (EUAF), demonstrated pelvic ring instability with minimal compression revealing the sites of instability, and rebound reduction upon release of compression. The injury is classified as an AO/OTA 61-B2.1 (lateral compression type I, incomplete posterior disruption).
Preoperative Plan
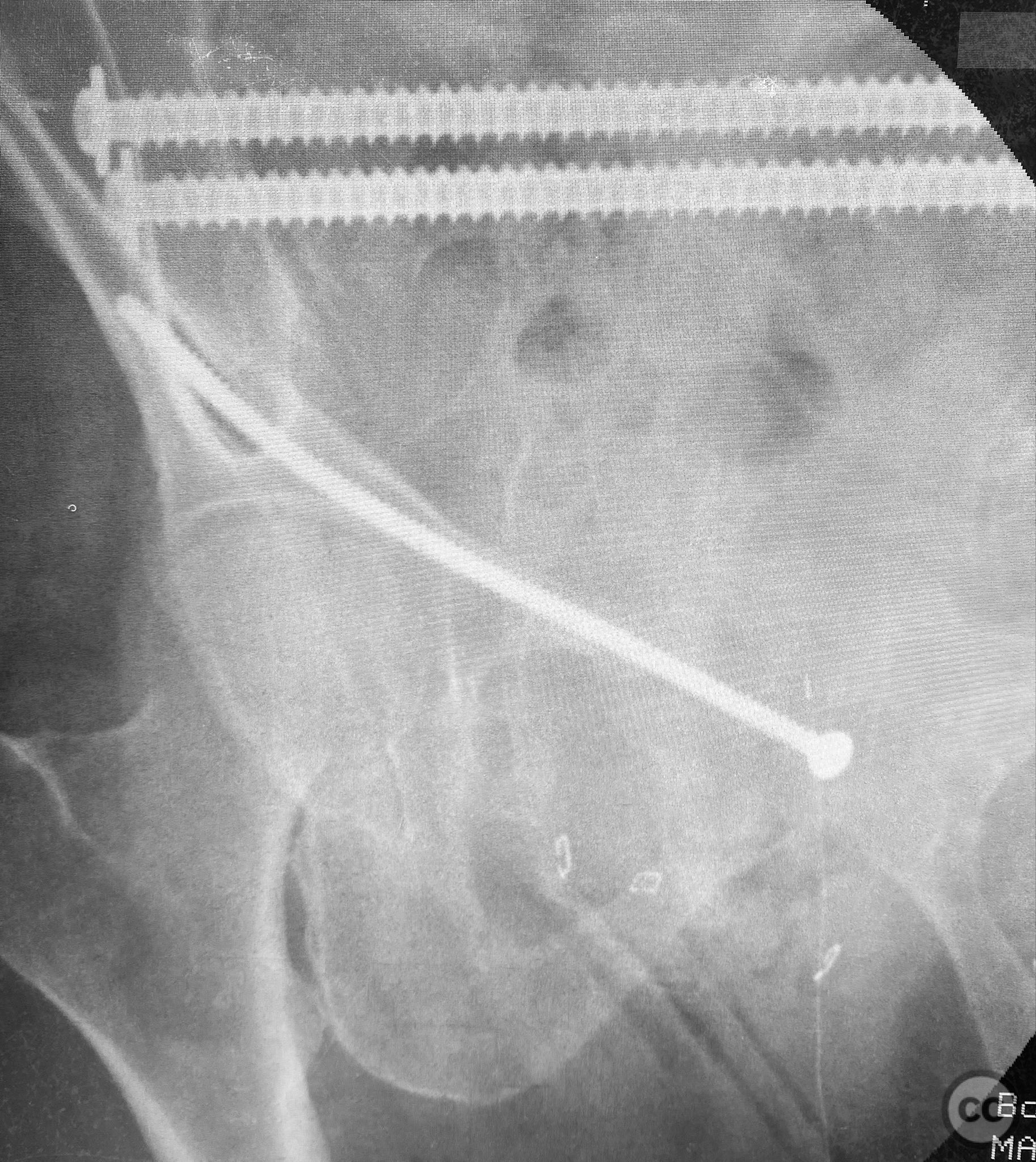
Planning remarks: The preoperative plan included percutaneous stabilization of the posterior pelvic ring using iliosacral (IS) screws placed in the upper sacral corridor. For anterior ring stabilization, a retrograde 4.5mm cortical blunt tip screw was planned for insertion along the superior pubic ramus isthmus, with implant size determined by the available bone corridor.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table to facilitate fluoroscopic imaging in multiple planes.
Anatomical surgical approach: For the posterior fixation, a percutaneous approach was utilized targeting the upper sacral ala, with stab incisions made over the posterior superior iliac spine and blunt dissection to bone. Under fluoroscopic guidance, guidewires were advanced across the sacroiliac joint into the S1 body, followed by cannulated IS screw insertion. For anterior fixation, a small incision was made over the pubic tubercle, and a 4.5mm blunt tip cortical screw was introduced retrograde along the superior pubic ramus isthmus under fluoroscopic control, advanced by screwdriver along the dense lateral iliac bone.
Operative remarks:Intraoperatively, EUAF confirmed instability sites and allowed dynamic assessment of reduction. IS screws were placed in the upper sacral path for posterior stabilization. The anterior ring was stabilized with a retrograde 4.5mm blunt tip cortical screw, advanced by turning with a screwdriver, utilizing the variable width of the ramus isthmus for optimal implant fit and stability. The technique permitted percutaneous fixation with minimal soft tissue disruption.
Postoperative protocol: Postoperatively, the patient was mobilized with walker assistance and reported comfortable ambulation following percutaneous screw fixation.
Follow up: Not specified
Orthopaedic implants used: 7.0mm cannulated iliosacral screws; 4.5mm blunt tip cortical threaded screw
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 305 times
11 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Percutaneous Screw Fixation for Pelvic Ring Instability in an Elderly Female. Journal of Orthopaedic Surgery and Traumatology. Case Report 42824576 Published Online Sep 11 2025.