










Proximal Femoral Fracture Dislocation with Posterior Wall Acetabular Fracture in a High-Energy Trauma.
Score and Comment on this Case
Clinical Details
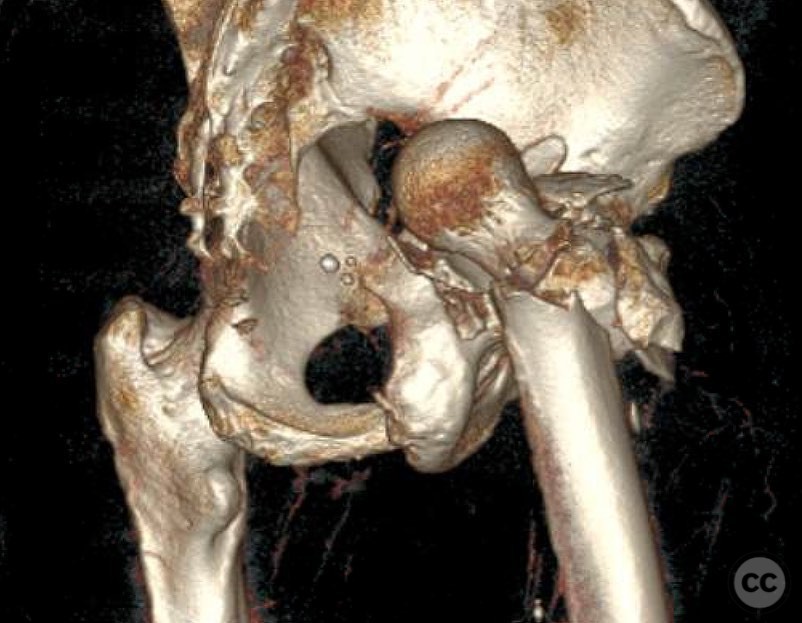
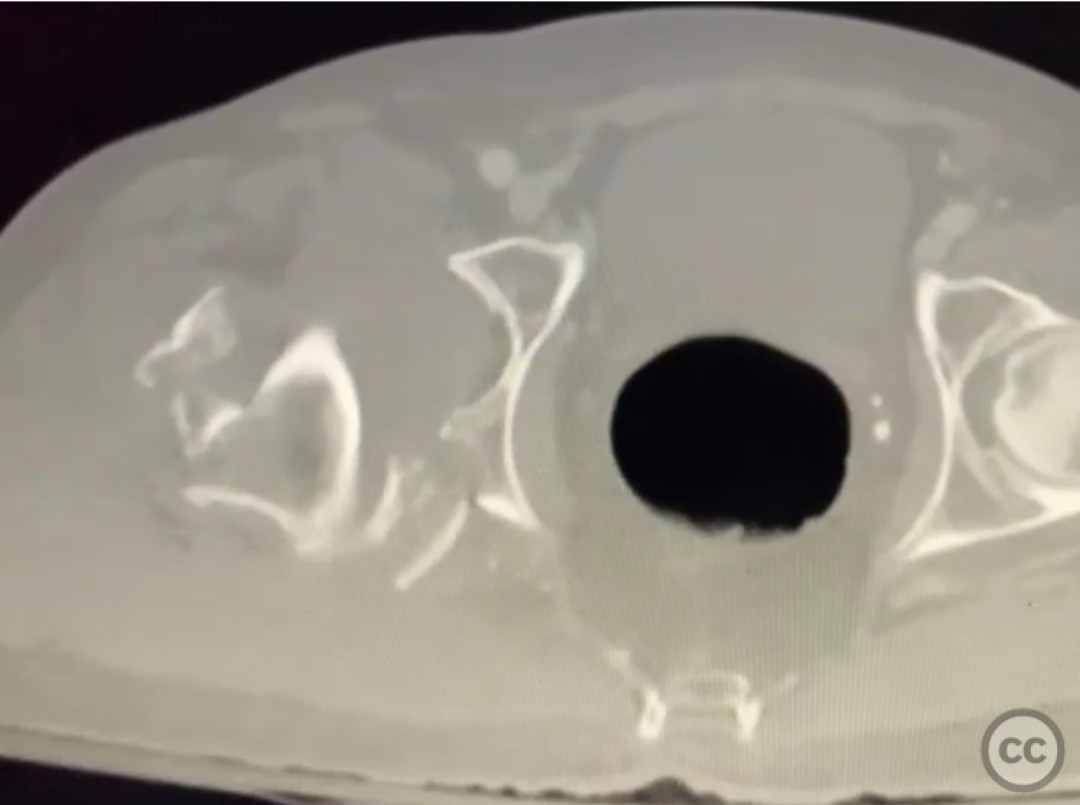
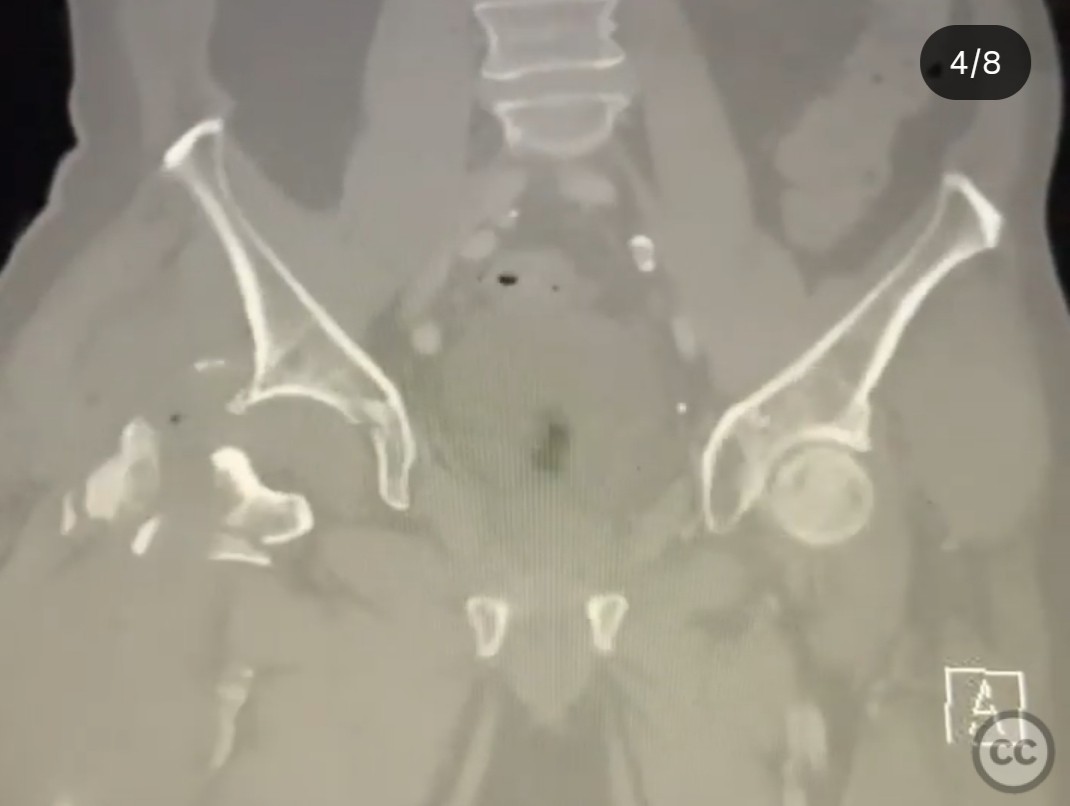
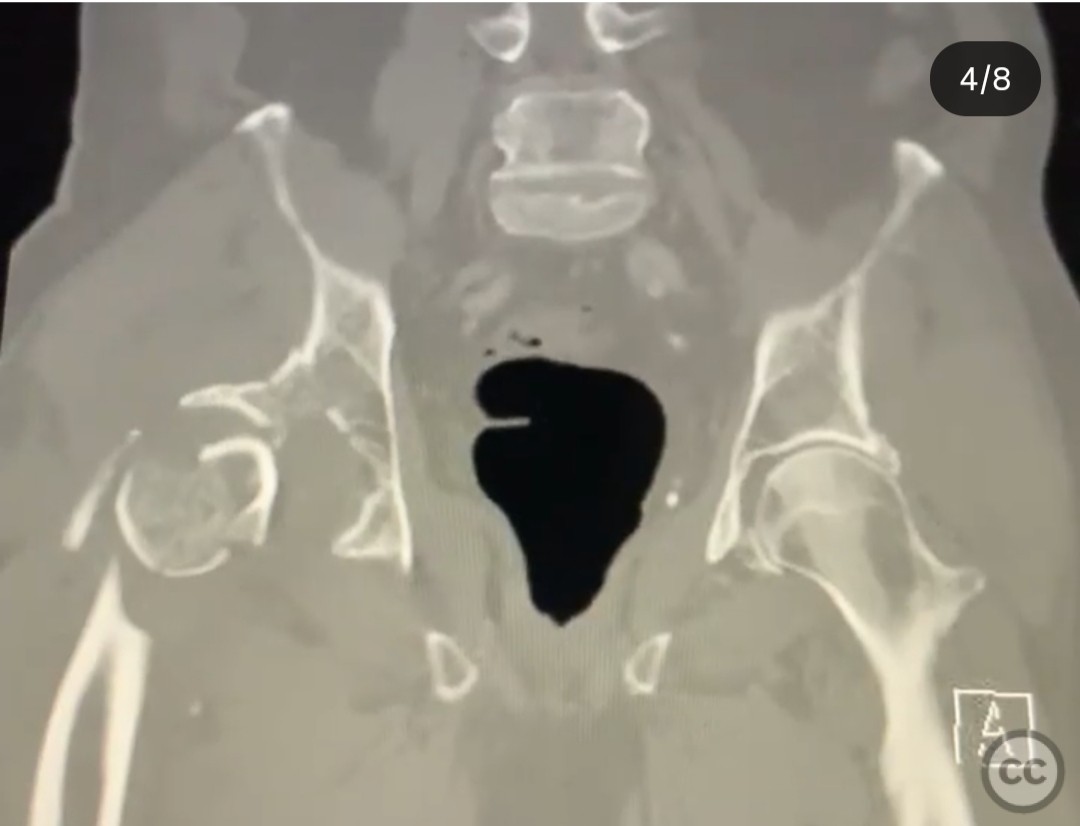
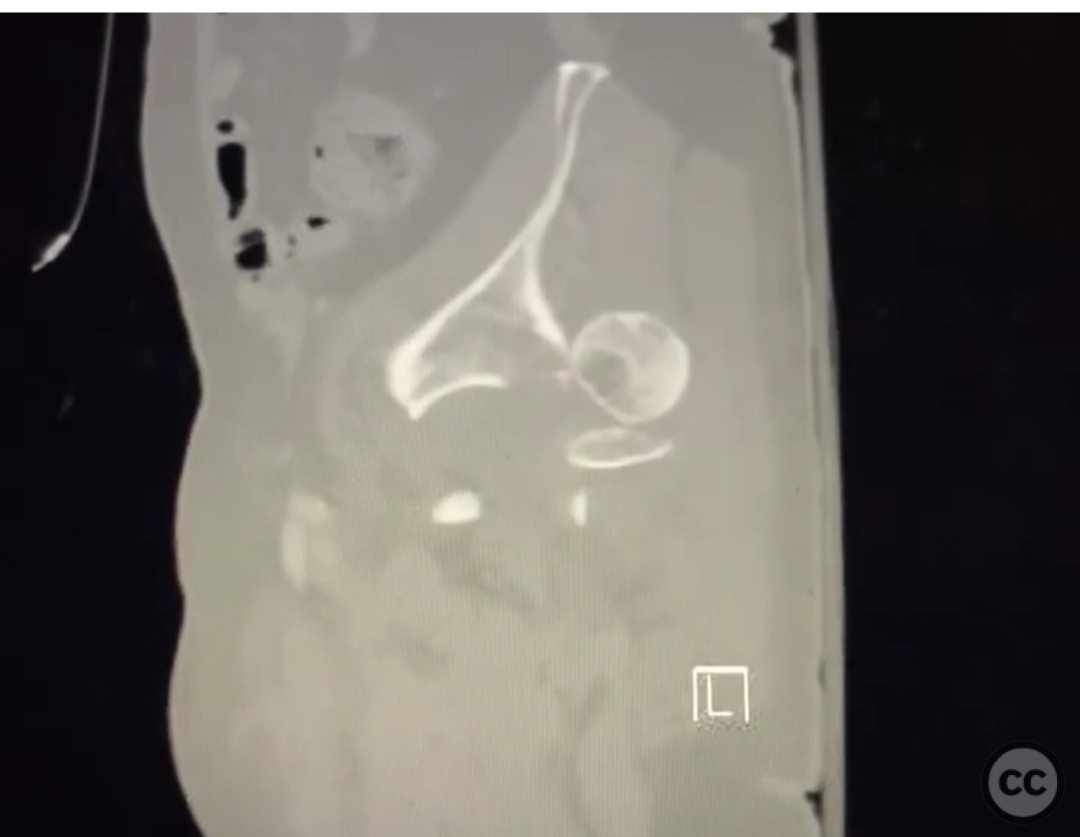
Clinical and radiological findings: A 71-year-old male involved in a high-speed motor vehicle collision presented with multiple rib fractures and a hemopneumothorax requiring bilateral chest tubes. Initially hemodynamically unstable, the patient was resuscitated successfully. Radiological assessment revealed a proximal femoral fracture dislocation involving the pertrochanteric region and a posterior wall acetabular fracture. The patient was placed in 20 lbs of distal femoral traction on an AP pelvis radiograph.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction through a Kocher-Langenbeck (KL) approach to address the irreducible proximal femoral fracture dislocation and posterior wall acetabular fracture. The decision was made to perform an open reduction of the hip and ORIF of the posterior wall first, followed by addressing the femoral fracture at a later stage.
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position to facilitate the Kocher-Langenbeck approach.
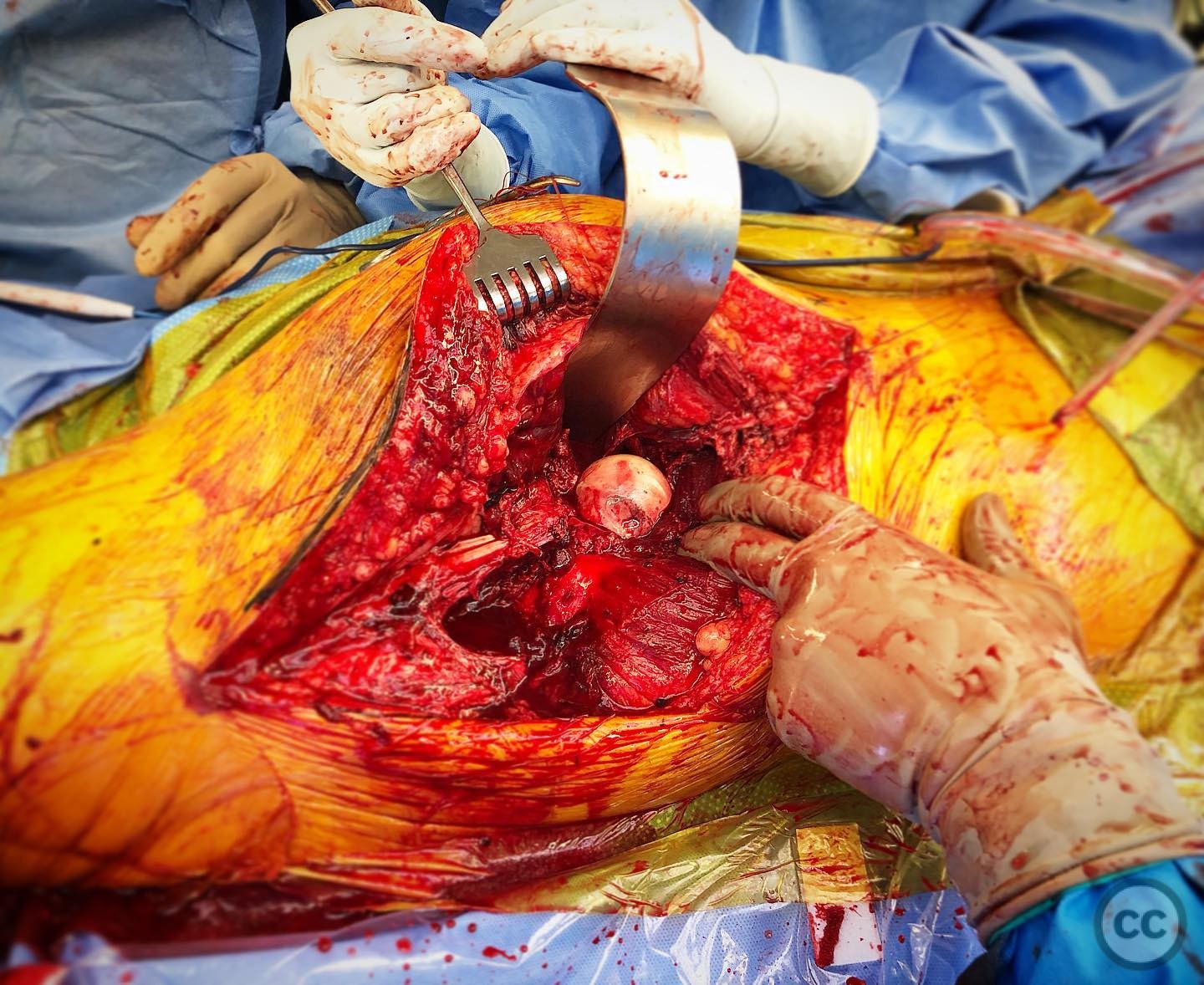
Anatomical surgical approach: The Kocher-Langenbeck approach was utilized, involving an incision over the greater trochanter extending distally along the femoral shaft. Subperiosteal dissection was performed to expose the posterior aspect of the acetabulum and proximal femur. Careful identification and protection of the sciatic nerve were paramount, with attention to distorted anatomical landmarks due to dislocation.
Operative remarks:The surgeon emphasized the importance of anatomical knowledge due to significant distortion caused by the dislocation. Key considerations included identifying the sciatic nerve, piriformis, conjoined tendon, and quadratus femoris. The surgical strategy prioritized restoring hip joint stability and congruity, addressing the posterior wall fracture first due to concerns about persistent instability. The proximal femoral morphology was subsequently restored using a static tension band plate technique with a 1/3 tubular plate for trochanteric fixation.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with gradual progression as tolerated, focusing on maintaining hip joint stability and monitoring for potential avascular necrosis.
Follow up: Not specified.
Orthopaedic implants used: 1/3 tubular plate for static tension band fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 270 times
19 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Proximal Femoral Fracture Dislocation with Posterior Wall Acetabular Fracture in a High-Energy Trauma.. Journal of Orthopaedic Surgery and Traumatology. Case Report 42777369 Published Online Jul 19 2025.