






 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_2.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_5.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_4.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_3.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior an(.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_9.jpg)
 wrap-up. If just joining_ check back to the previous post for injury details._._._._This was a badly open bifocal direct posterior a_1.jpg)
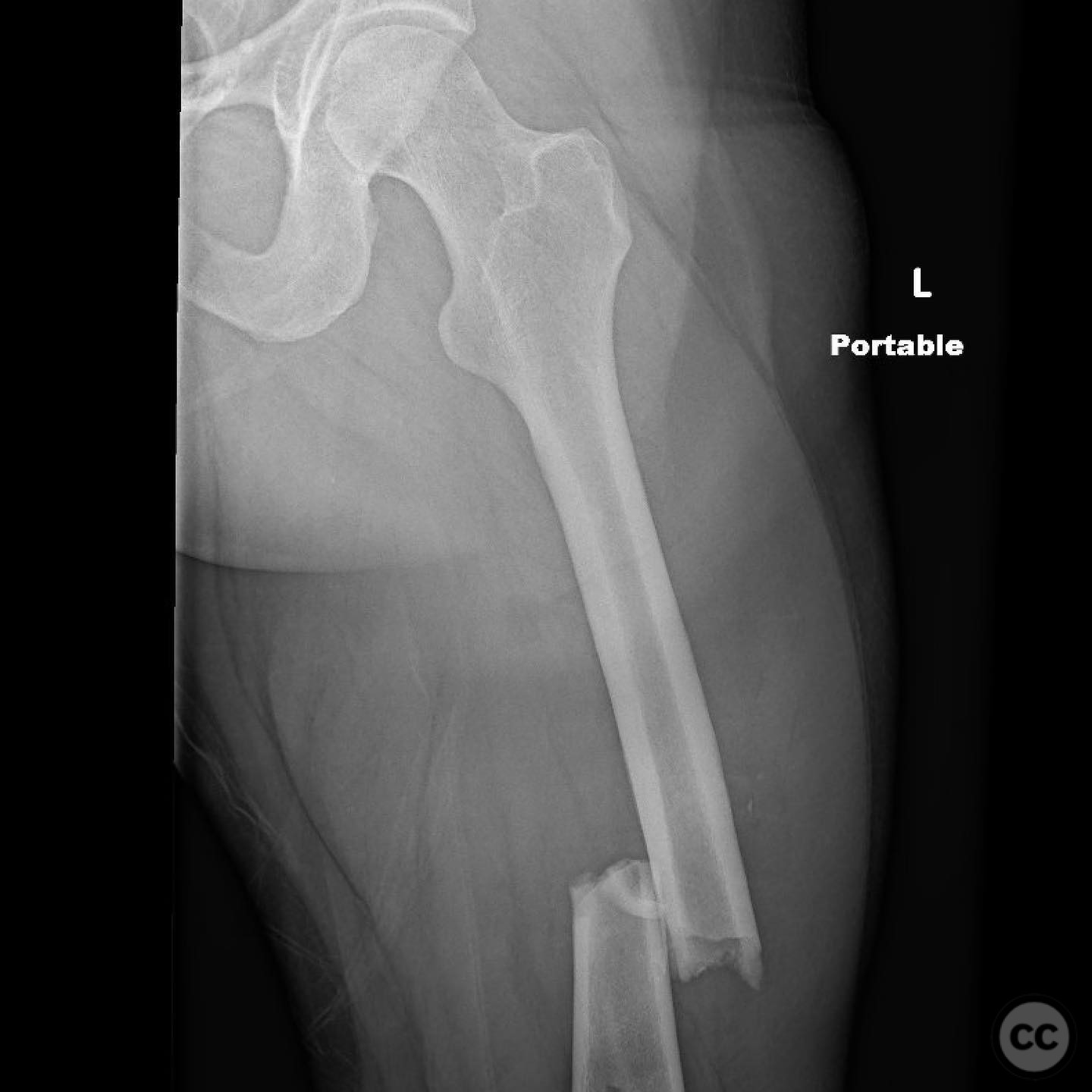
Complex Floating Knee Injury with Open Bifocal Tibial Fracture and Ipsilateral Femoral Fractures
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 23-year-old male involved in a motorcycle versus car collision presented with a closed diaphyseal femur fracture, a Gustilo-Anderson type 3a open distal femur fracture, and a complex open diaphyseal tibia fracture with both direct anterior (3 cm) and direct posterior (10x12 cm) wounds. Additionally, there was an ipsilateral closed ankle injury. The patient had no head or abdominal injuries but did have a hemopneumothorax managed with a chest tube. Initial lactate levels were elevated at 7 mmol/L, decreasing to 3 mmol/L with normal saline and two units of packed red blood cells. Coagulation profile was normal, platelets were 250 x 10^9/L, and hematocrit was 27%. The patient required light vasopressor support and was intubated with normal ventilatory requirements.
Preoperative Plan
Planning remarks: The preoperative plan focused on debridement, irrigation, and stabilization of the open bifocal tibial fracture. A formal arthrotomy was planned to reduce the distal femur fracture. Intramedullary nailing of the tibia was prioritized, with subsequent reduction and stabilization of the distal femur fracture using lag screws and a buttress plate.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent table to facilitate access to both the femur and tibia for intramedullary nailing and open reduction internal fixation procedures.
Anatomical surgical approach: A formal arthrotomy was performed to address the distal femur fracture. For the tibial fracture, an anteromedial approach was utilized for debridement and irrigation, followed by intramedullary nailing through a standard entry point. The fibula was addressed through a lateral approach for open reduction and internal fixation to restore length, rotation, and alignment.
Operative remarks:Intraoperatively, after nailing the tibia, pulmonary concerns necessitated a temporary halt in the procedure. The distal femur fracture was reduced and stabilized with lag screws and a buttress plate, avoiding interference with the planned femoral nail. The patient was placed in traction and transferred to the ICU for stabilization. On the following day, the patient underwent antegrade femoral nailing, ORIF of the fibula, medial malleolus, proximal tibiofibular joint, and syndesmosis. Emphasis was placed on achieving correct fibular alignment to ensure proper joint reduction.
Postoperative protocol: Postoperatively, the anterior wound was closed on day one, with plans for potential grafting if healing around the cement was inadequate. The posterior wound was treated with split-thickness skin grafting (STSG). The rehabilitation protocol included non-weight bearing on the affected limb initially, with gradual progression based on clinical and radiological assessments.
Follow up: Not specified.
Orthopaedic implants used: Intramedullary nail for tibia, lag screws, buttress plate for distal femur, ORIF hardware for fibula, medial malleolus, proximal tibiofibular joint, and syndesmosis fixation devices.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 293 times
11 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Floating Knee Injury with Open Bifocal Tibial Fracture and Ipsilateral Femoral Fractures. Journal of Orthopaedic Surgery and Traumatology. Case Report 41513593 Published Online Jul 11 2025.