







Rotational Ankle Fracture Dislocation with Medial Skin Compromise
Score and Comment on this Case
Clinical Details
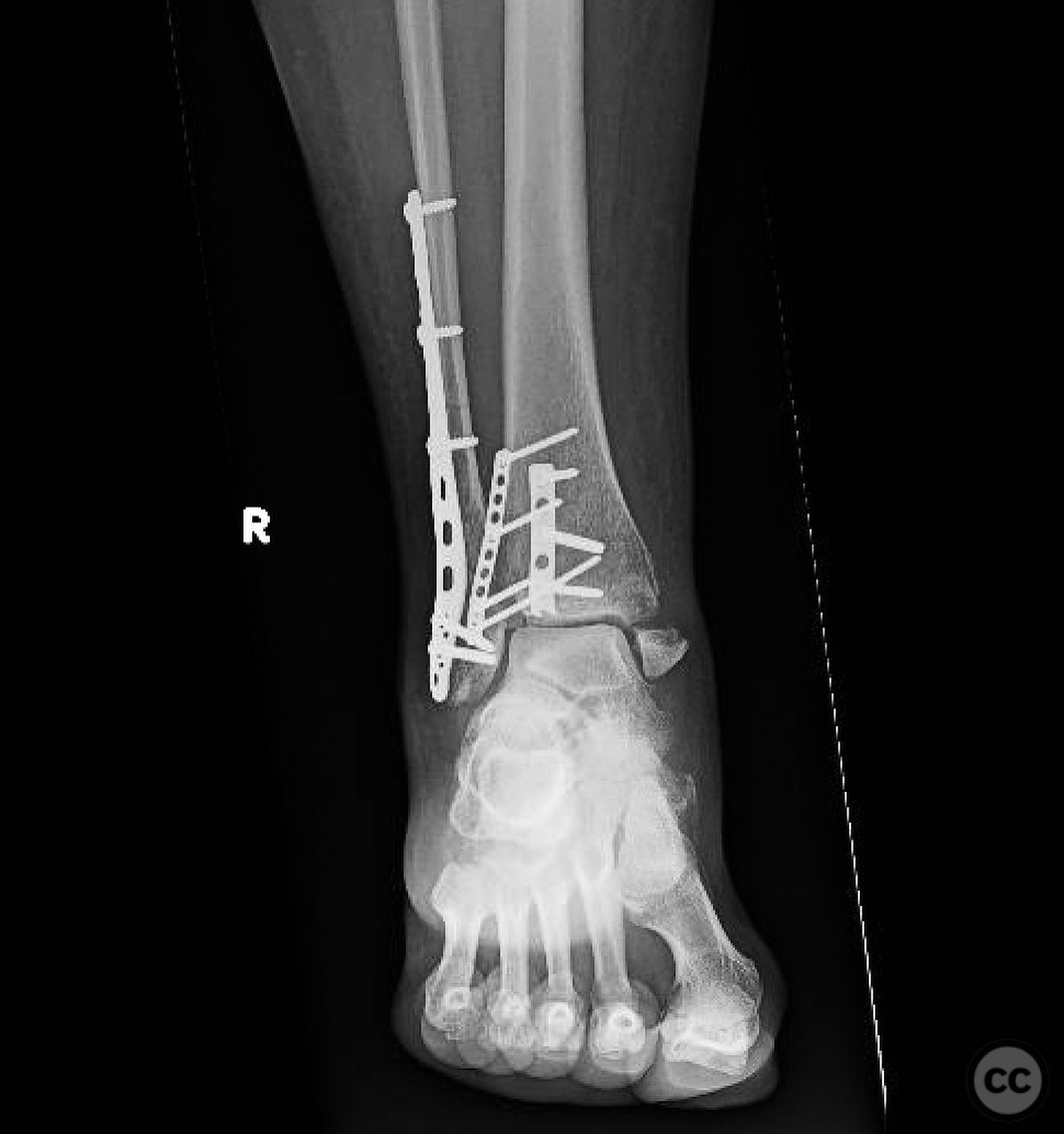
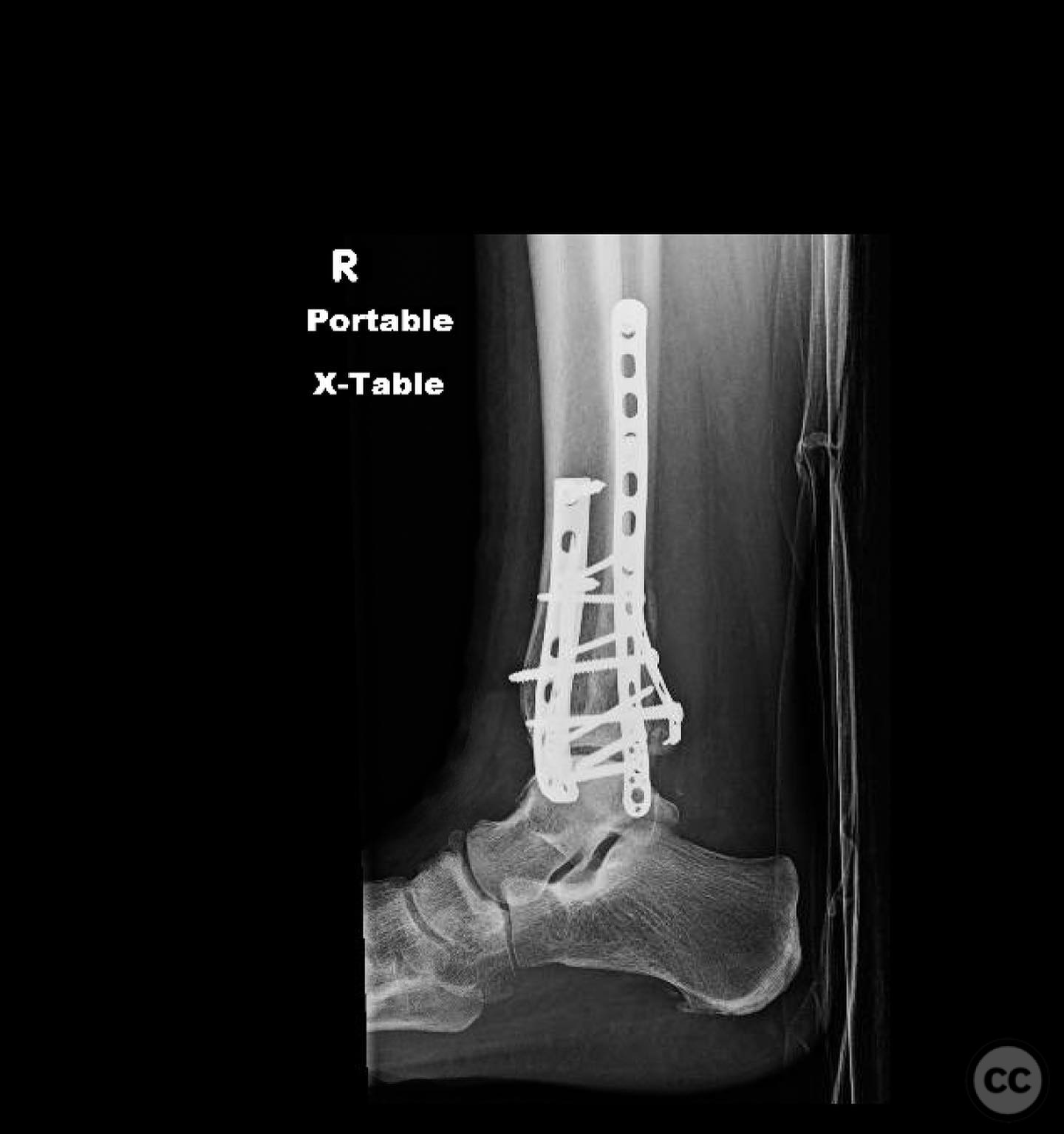
Clinical and radiological findings: A patient presented with a closed ankle fracture dislocation, initially managed with three unsuccessful reduction attempts at an outside facility. On presentation, four days post-injury, the ankle remained dislocated. The medial skin exhibited significant compromise, with hemorrhagic blistering indicative of full-thickness dermal injury, while the lateral skin was intact. Radiological assessment, including CT imaging, revealed a rotational ankle fracture dislocation with a large Chaput fragment, a gross posterior malleolus fracture, a standard distal fibula fracture, and a medial malleolus fracture, alongside syndesmotic disruption.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction and internal fixation (ORIF) of the lateral structures due to the healthy lateral skin, avoiding immediate intervention on the compromised medial side. The surgical approach was planned to address the fibula, posterior malleolus, and Chaput fragment acutely, with consideration for delayed medial malleolus intervention if necessary.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table to facilitate access to the lateral aspect of the ankle.
Anatomical surgical approach: A lateral approach to the ankle was performed via an incision centered over the fibula, allowing for open reduction and internal fixation of the distal fibula fracture. Through this approach, the posterior malleolus and Chaput fragments were also addressed and stabilized, while avoiding any medial dissection to preserve the integrity of the compromised medial soft tissues.
Operative remarks:The surgeon opted against external fixation due to the healthy lateral skin and the instability of rotational patterns in a delta frame. Immediate fixation of the lateral side was prioritized to provide stability without compromising the vulnerable medial skin. The decision was made to delay intervention on the medial malleolus until soft tissue conditions improved, acknowledging that a symptomatic nonunion could be addressed later if necessary.
Postoperative protocol: Postoperatively, the patient was placed in a splint to maintain stability while allowing for soft tissue recovery. Weight-bearing was restricted until adequate healing of the medial skin was observed.
Follow up: Not specified.
Orthopaedic implants used: Orthopaedic implants used included internal fixation devices for the fibula, posterior malleolus, and Chaput fragment.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 329 times
18 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Rotational Ankle Fracture Dislocation with Medial Skin Compromise. Journal of Orthopaedic Surgery and Traumatology. Case Report 39933678 Published Online Jul 18 2025.