







Peri-implant Both-Bone Forearm Fracture in a Patient with DRUJ Arthroplasty and a Concurrent Proximal Femoral Fracture
Score and Comment on this Case
Clinical Details
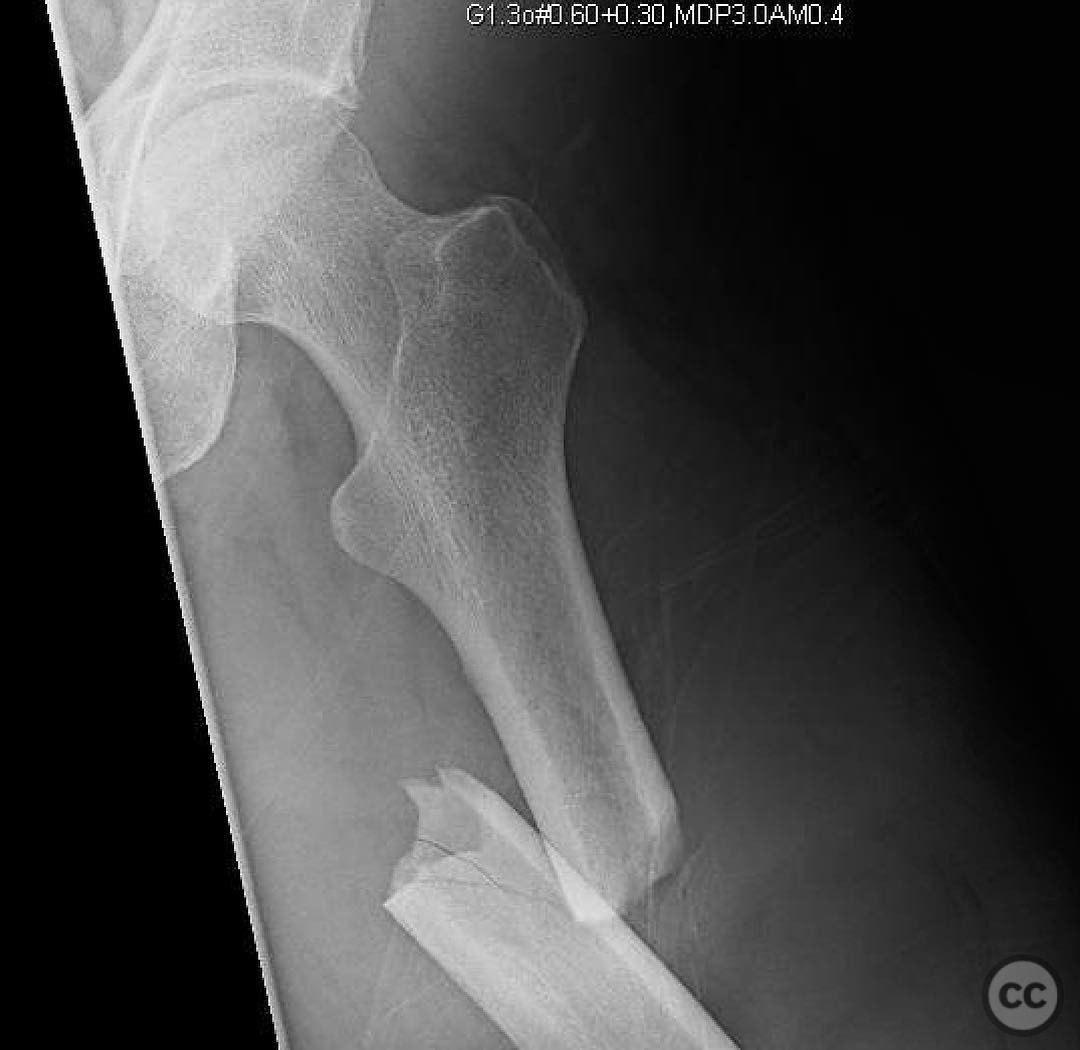
Clinical and radiological findings: A 52-year-old male involved in a motorcycle accident presented with a peri-implant both bone forearm fracture. The patient had a previous Shecker distal radioulnar joint (DRUJ) arthroplasty. Initial radiographs demonstrated a fracture of both the radius and ulna around the implant site. The fracture of the radius was straightforward, while the ulna fracture was complicated by its location, pattern, and the presence of the prosthetic stem, resulting in a significant stress concentration with limited bone stock.
Preoperative Plan
Planning remarks: The preoperative plan involved overlapping implants to avoid stress risers for the radius fixation. For the ulna, due to the complex fracture pattern and limited bone stock around the stem, a revision strategy was planned using a long 3.5 mm LCDC plate with cables and distal radius autograft.
Surgical Discussion
Patient positioning: Supine position with the affected arm placed on a radiolucent hand table to allow optimal access and imaging during the procedure.
Anatomical surgical approach: A longitudinal incision was made over the radial aspect of the forearm to expose the radius. Subperiosteal dissection was performed to visualize the fracture site. For the ulna, a separate incision was made along its subcutaneous border, carefully avoiding damage to the existing prosthetic components.
Operative remarks:The initial fixation of the ulna with a stiff 2.7 mm locking plate failed due to inadequate support around the prosthetic stem and stress concentration. The revision involved using a long 3.5 mm LCDC plate with cables to provide additional stability, supplemented by distal radius autograft to enhance bone stock and promote healing.
Postoperative protocol: Postoperative protocol included immobilization in a splint for 6 weeks, followed by gradual range of motion exercises. Weight-bearing activities were restricted until radiographic evidence of healing was observed.
Follow up: Not specified.
Orthopaedic implants used: Long 3.5 mm LCDC plate, cables, distal radius autograft.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 330 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Peri-implant Both-Bone Forearm Fracture in a Patient with DRUJ Arthroplasty and a Concurrent Proximal Femoral Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 38588914 Published Online Jul 21 2025.