










Combined Bilateral Sacroiliac Disruption and Transtectal Transverse Acetabular Fracture with Ipsilateral Femoral Shaft Fracture
Score and Comment on this Case
Clinical Details
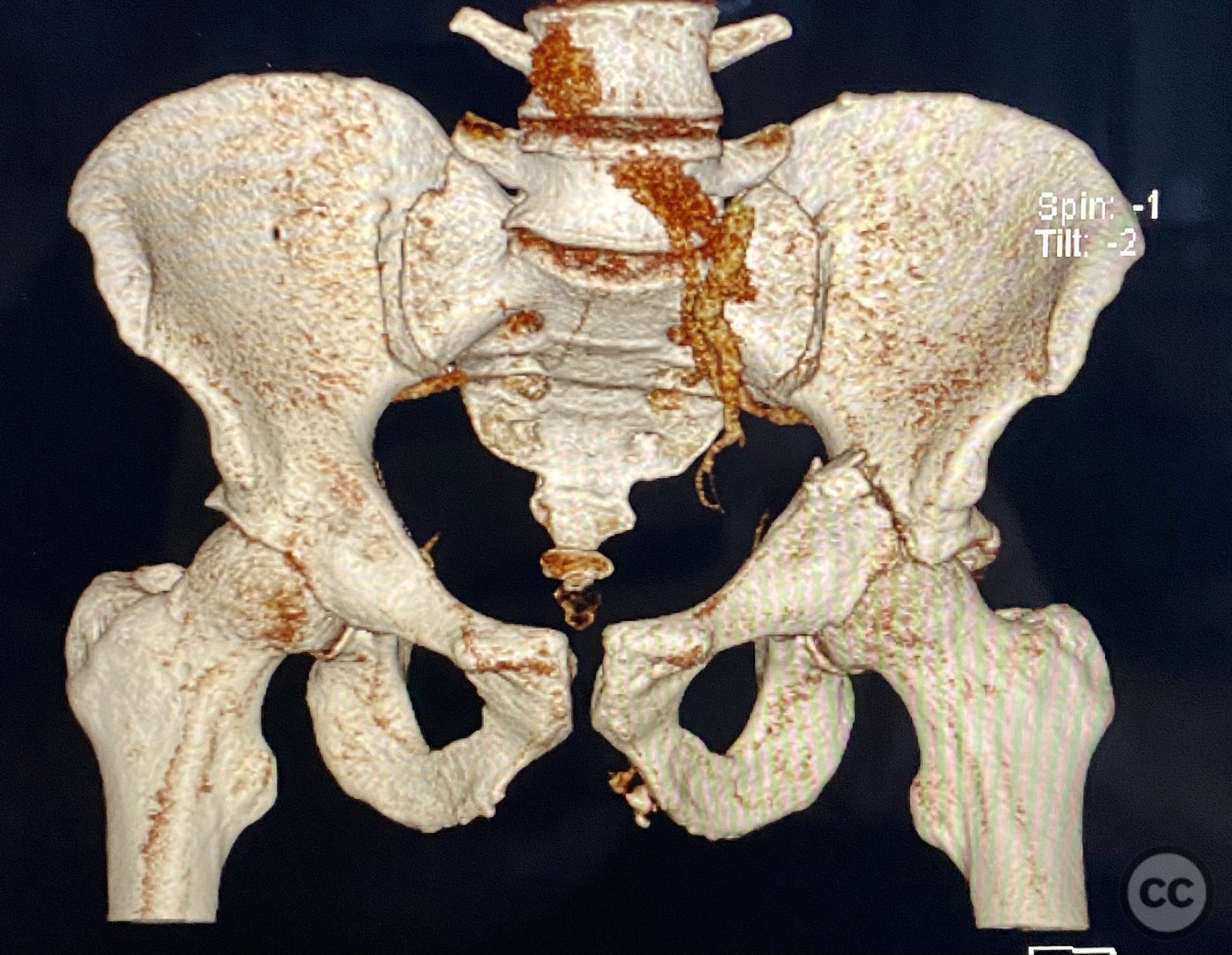
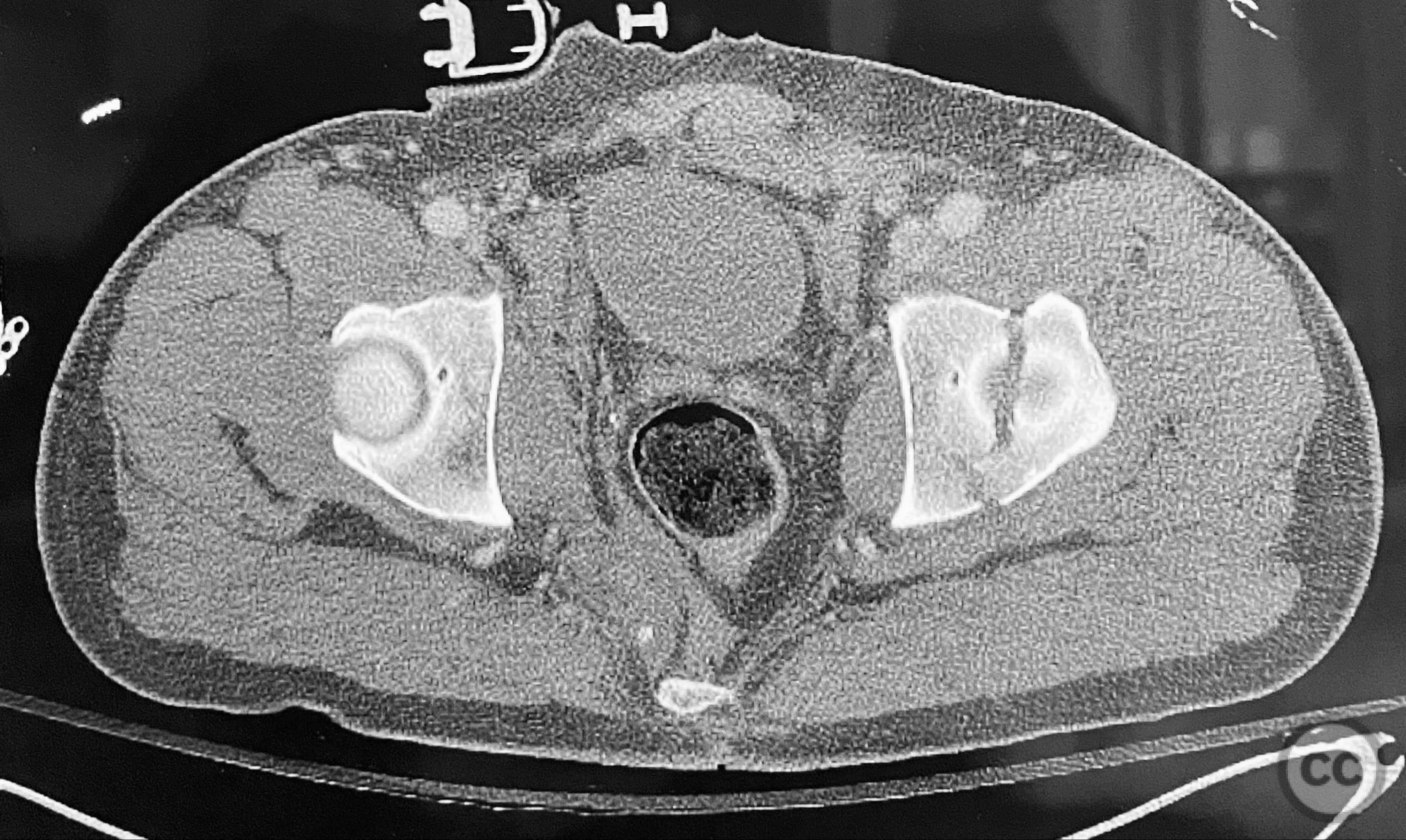
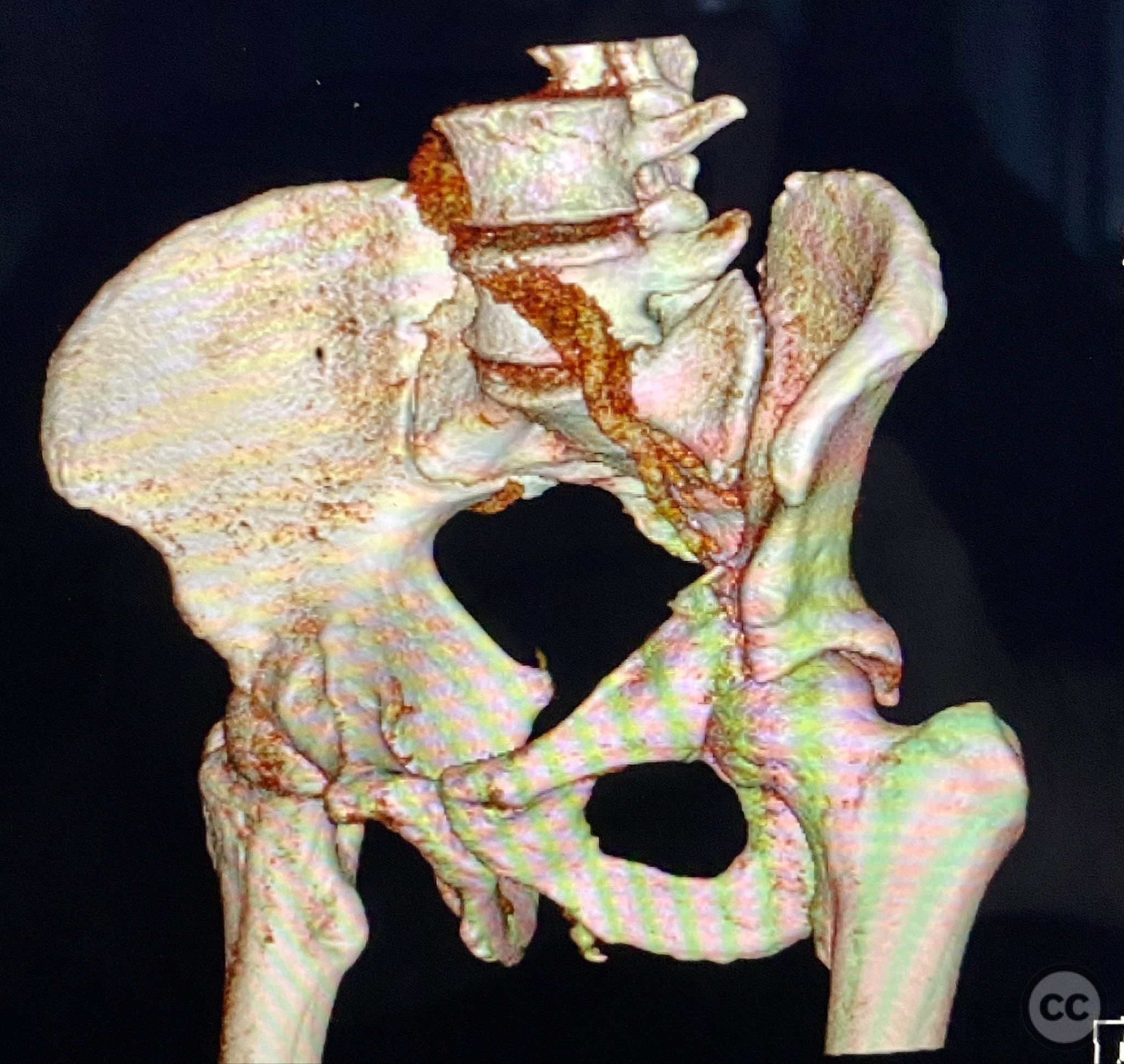
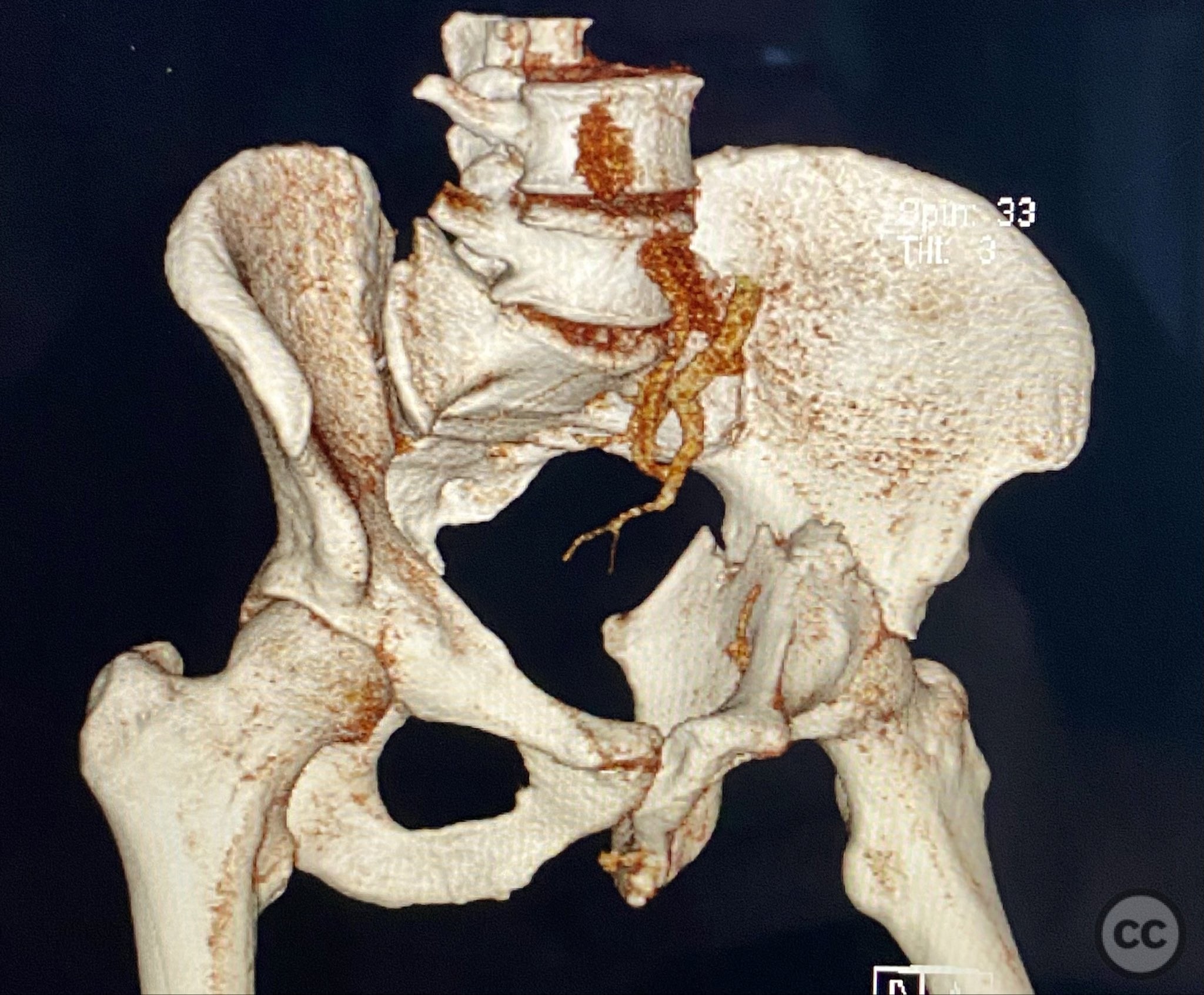
Clinical and radiological findings: Adult male with a closed, comminuted left femoral shaft fracture and complex pelvic ring injury. Initial imaging demonstrated bilateral sacroiliac (SI) joint disruptions and a left-sided transtectal transverse acetabular fracture (Letournel-Judet: transverse type), with the fracture line exiting through the posterior wall region but without a discrete posterior wall fragment. The femoral head was displaced caudally, following the unstable distal acetabular segment, resulting in loss of congruency with the intact acetabular dome. There was also a symphyseal disruption. No associated abdominal, visceral, thoracic, cranial, or other injuries were present. Application of a circumferential pelvic binder resulted in visible changes in pelvic alignment on imaging. AO/OTA Classification: - Pelvic ring: 61-C1.3 (bilateral SI joint disruption, complete instability) - Acetabulum: 62-B1 (transverse fracture) - Femur: 32-C3 (comminuted diaphyseal fracture)
Preoperative Plan
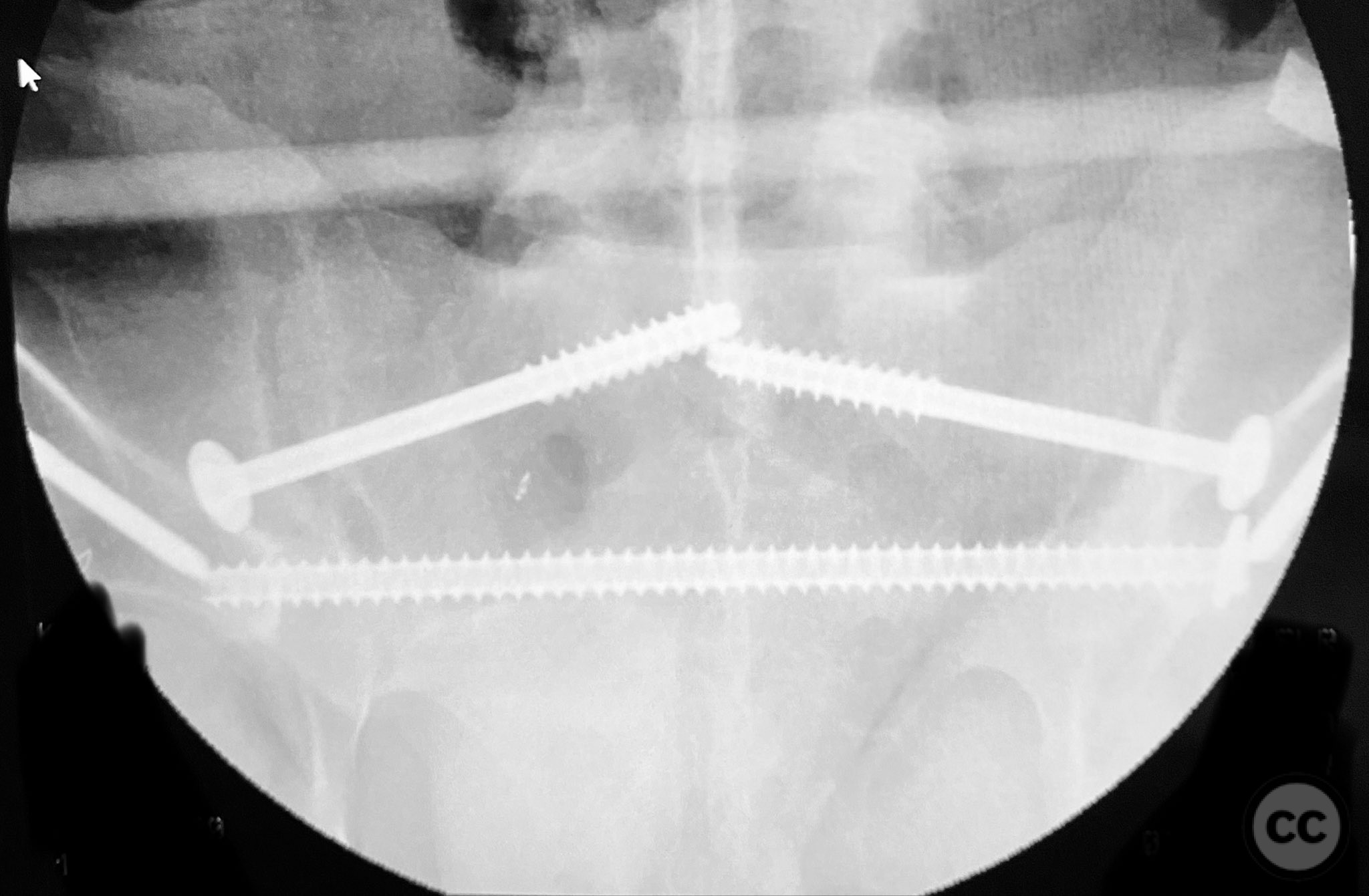
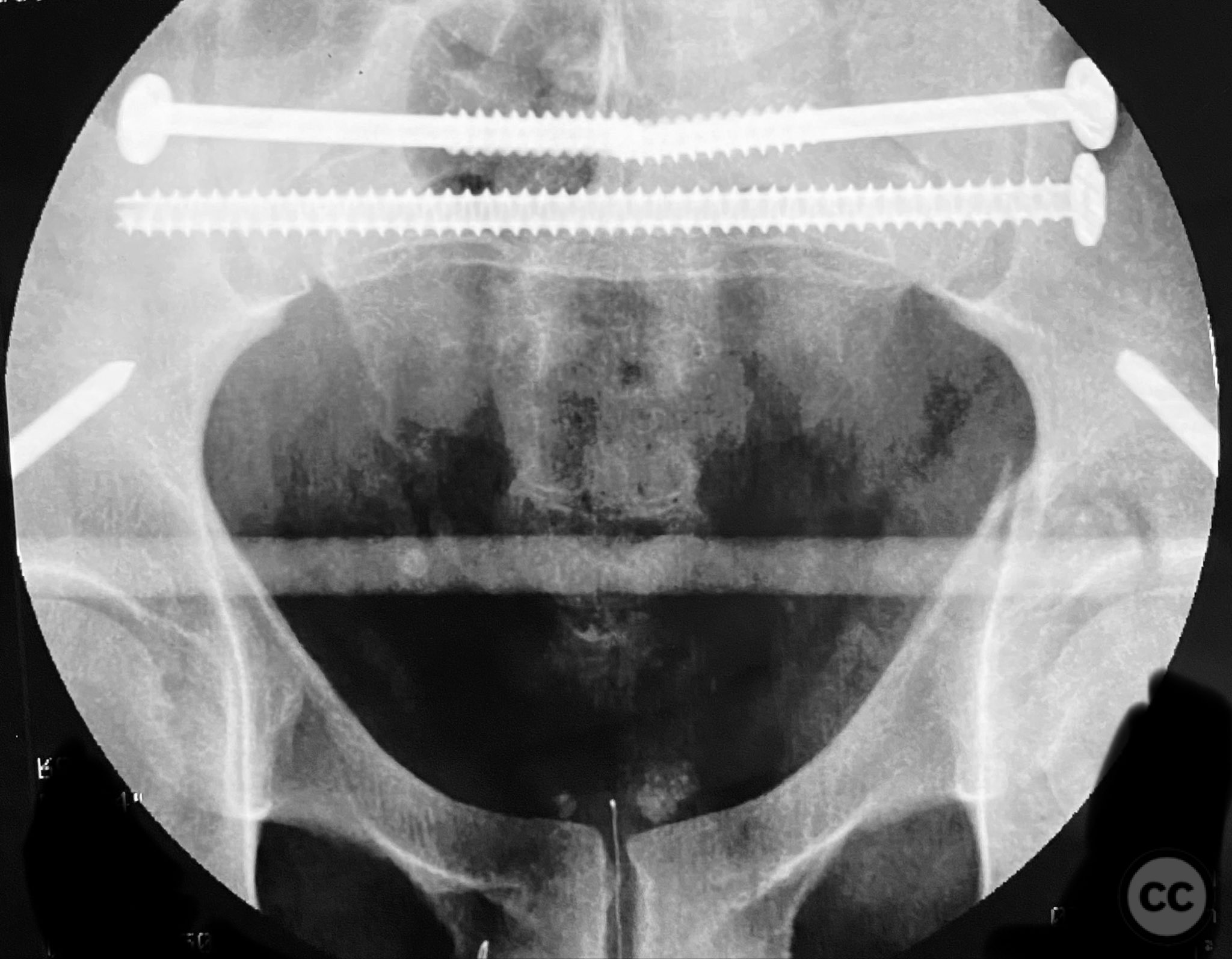
Planning remarks: The preoperative plan involved staged management: initial resuscitation and provisional stabilization with a circumferential pelvic binder, followed by operative reduction and fixation of the pelvic ring using an anterior two-pin external fixator for SI joint compression and reduction, percutaneous iliosacral (IS) and transsacral (TS) screw fixation, and subsequent intramedullary nailing of the femur. Definitive acetabular fixation was planned via a posterior Kocher-Langenbeck approach in the prone position.
Surgical Discussion
Patient positioning: For pelvic and femoral fixation, the patient was positioned supine to facilitate access for external fixation, percutaneous SI/TS screw placement, and femoral nailing. For acetabular fixation, the patient was repositioned prone for the Kocher-Langenbeck a
Anatomical surgical approach: The Kocher-Langenbeck approach was performed with the patient in the prone position. A longitudinal incision was made centered over the greater trochanter, extending distally along the femoral shaft and proximally toward the posterior superior iliac spine. The gluteus maximus was split in line with its fibers, and the short external rotators (piriformis, obturator internus, gemelli) were identified and retracted or released as necessary to expose the posterior column and wall of the acetabulum. The sciatic nerve was identified and protected throughout. Direct visualization of the posterior column fracture allowed for clamp-assisted reduction.
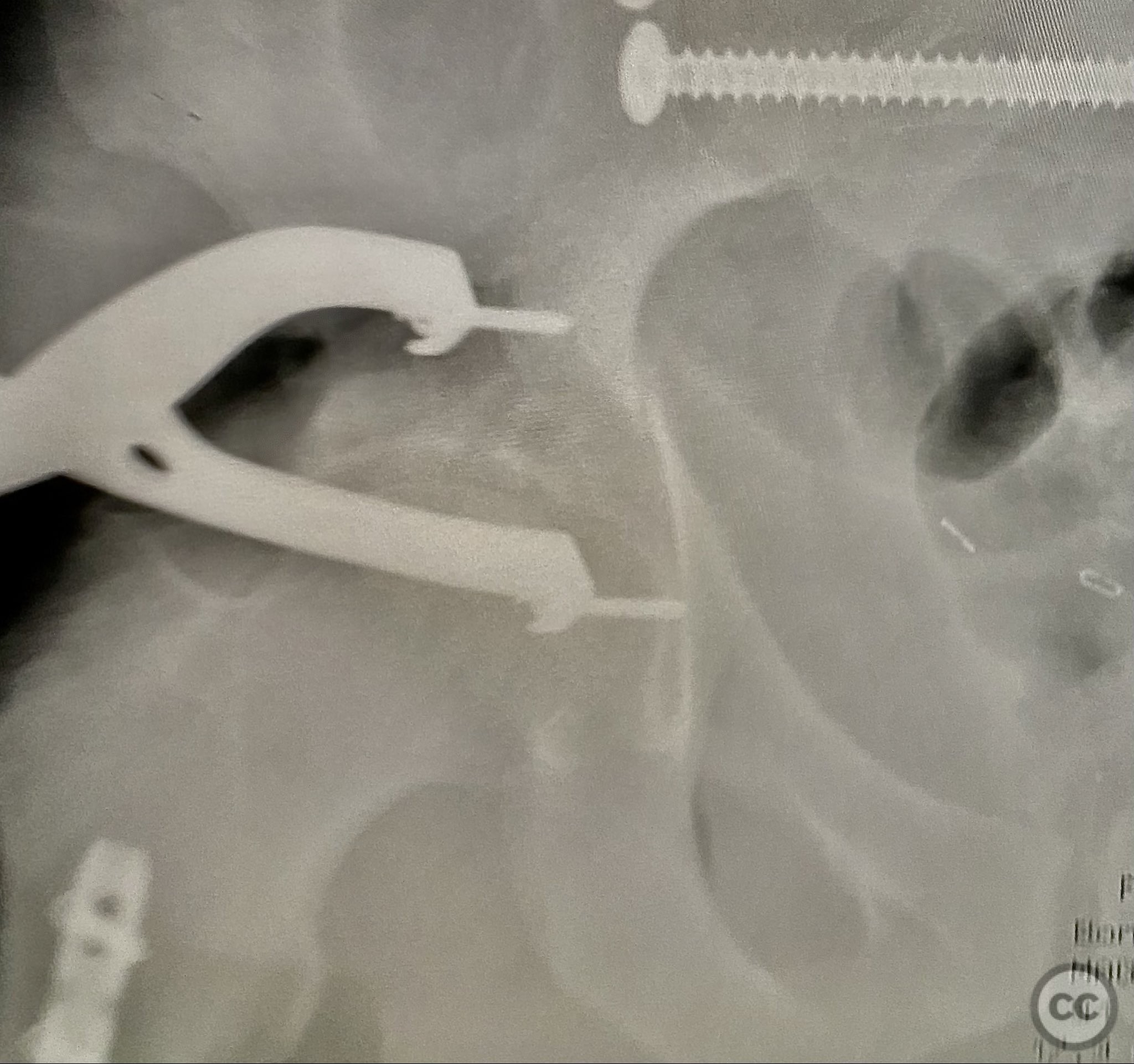
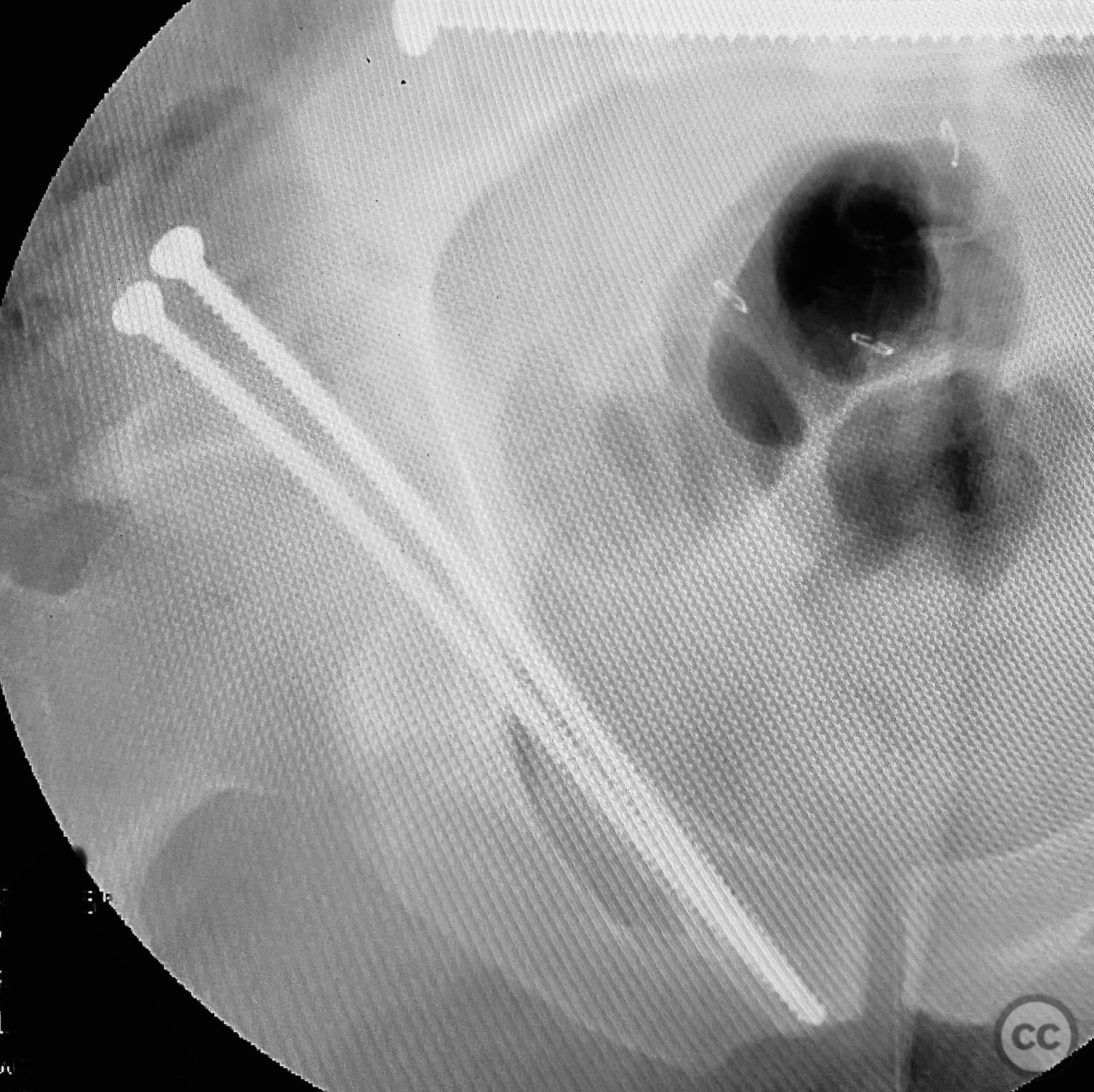
Operative remarks:Initial reduction of the posterior column was attempted using a Jungbluth clamp; however, intraoperative fluoroscopy revealed suboptimal reduction despite satisfactory direct visualization. A perpendicular reduction clamp was then applied, resulting in improved alignment as confirmed by fluoroscopy. The transverse acetabular fracture was stabilized with two 4.5 mm cortical screws placed across the fracture line, followed by application of posterior column plates for additional stability. The symphyseal disruption was managed non-operatively without direct stabilization.
Postoperative protocol: Postoperative rehabilitation included protected weight bearing on the affected side for a minimum of 8–12 weeks, with early initiation of passive and active-assisted range of motion exercises for the hip and knee. Progression to partial and then full weight bearing was guided by radiographic evidence of healing and clinical assessment.
Follow up: Not specified
Orthopaedic implants used: - Anterior two-pin external fixator - Percutaneous iliosacral screw(s) - Percutaneous transsacral screw(s) - Intramedullary femoral nail - 4.5 mm cortical screws (acetabular fixation) - Posterior column reconstruction plate(s)
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 846 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Combined Bilateral Sacroiliac Disruption and Transtectal Transverse Acetabular Fracture with Ipsilateral Femoral Shaft Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 38340598 Published Online Sep 12 2025.