











Bipolar Clavicle Fracture with Medial Multifragmentary Displacement
Score and Comment on this Case
Clinical Details
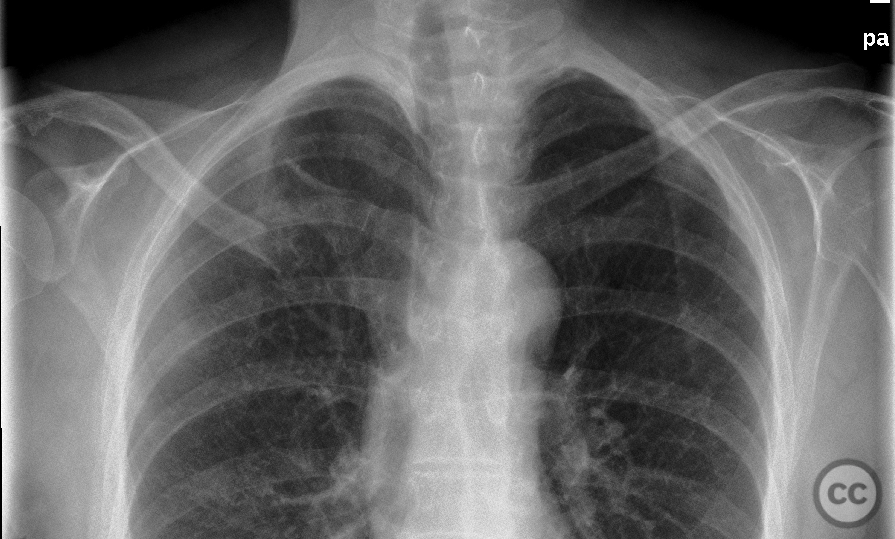
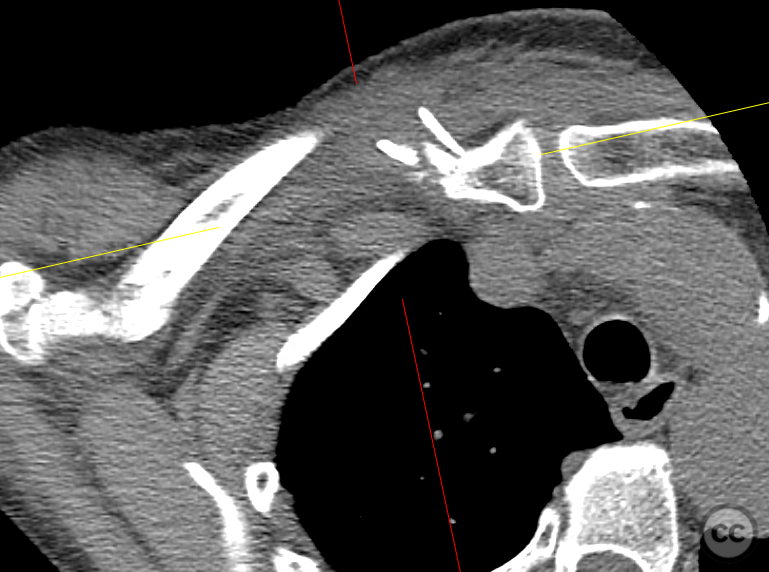
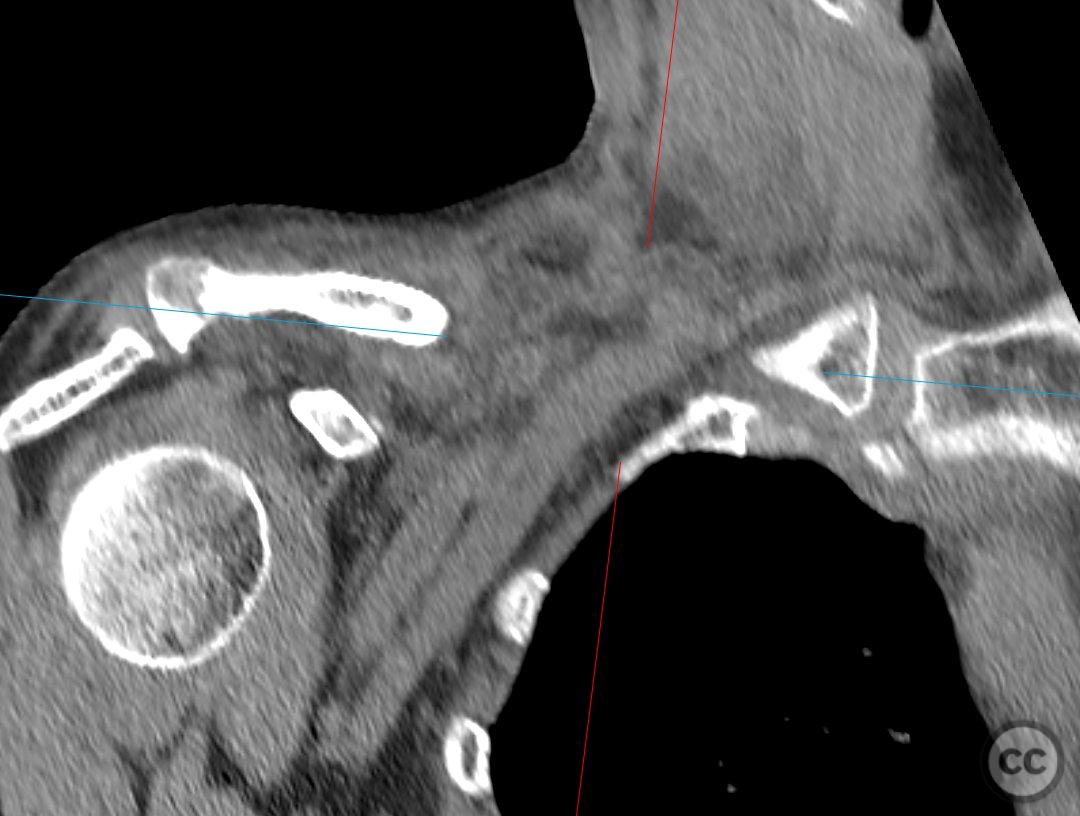
Clinical and radiological findings: A 65-year-old female presented after sustaining a moderate energy, awkward mechanism injury with direct impact to the right clavicle, resulting in a bipolar clavicle fracture. The lateral fracture was minimally displaced, classified as Neer type 1, while the medial clavicle fracture was grossly displaced and multifragmentary. The medial diaphysis was notably buried in the pectoralis muscle, with vascular structures closely associated with the medial fragment and fracture zone.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction and internal fixation, with a focus on carefully managing the proximity of vascular structures to the medial fracture zone. A direct approach over the medial clavicle was planned for surgical access.
Surgical Discussion
Patient positioning: The patient was positioned supine, avoiding a beach chair or upright torso position due to concerns regarding potential air embolism risks.
Anatomical surgical approach: A direct surgical approach was executed over the medial clavicle, incising the fascia overlying the clavicle and subperiosteal release of the pectoralis major and sternocleidomastoid muscles. Dissection was extended medially to the sternoclavicular joint, identifying the vertical fibers of the distal sternocleidomastoid for careful mobilization of the fracture fragments.
Operative remarks:During surgery, careful mobilization of the fracture facilitated reduction without undue tension on surrounding soft tissues. Although some residual impaction was noted upon reduction, it was deemed clinically irrelevant. A medial clavicle plate from Synthes was placed under fluoroscopic guidance, with monocortical fixation using 2.7mm screws medially to prevent posterior perforation, and bicortical diaphyseal screw placement laterally, again utilising careful drilling technique to avoid far cortex perforation.
Postoperative protocol: Postoperative management included symptomatic immobilization in a shoulder sling, with non-weight bearing range of motion exercises up to 90 degrees of flexion/abduction encouraged for up to 6 weeks.
Follow up: Not specified
Orthopaedic implants used: 2.7mm medial clavicle plate from Synthes
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Juan Varela
Great case So unusual