








Vertical Displaced Femoral Neck Fracture in a Young Male: Open Reduction and Internal Fixation
Score and Comment on this Case
Clinical Details
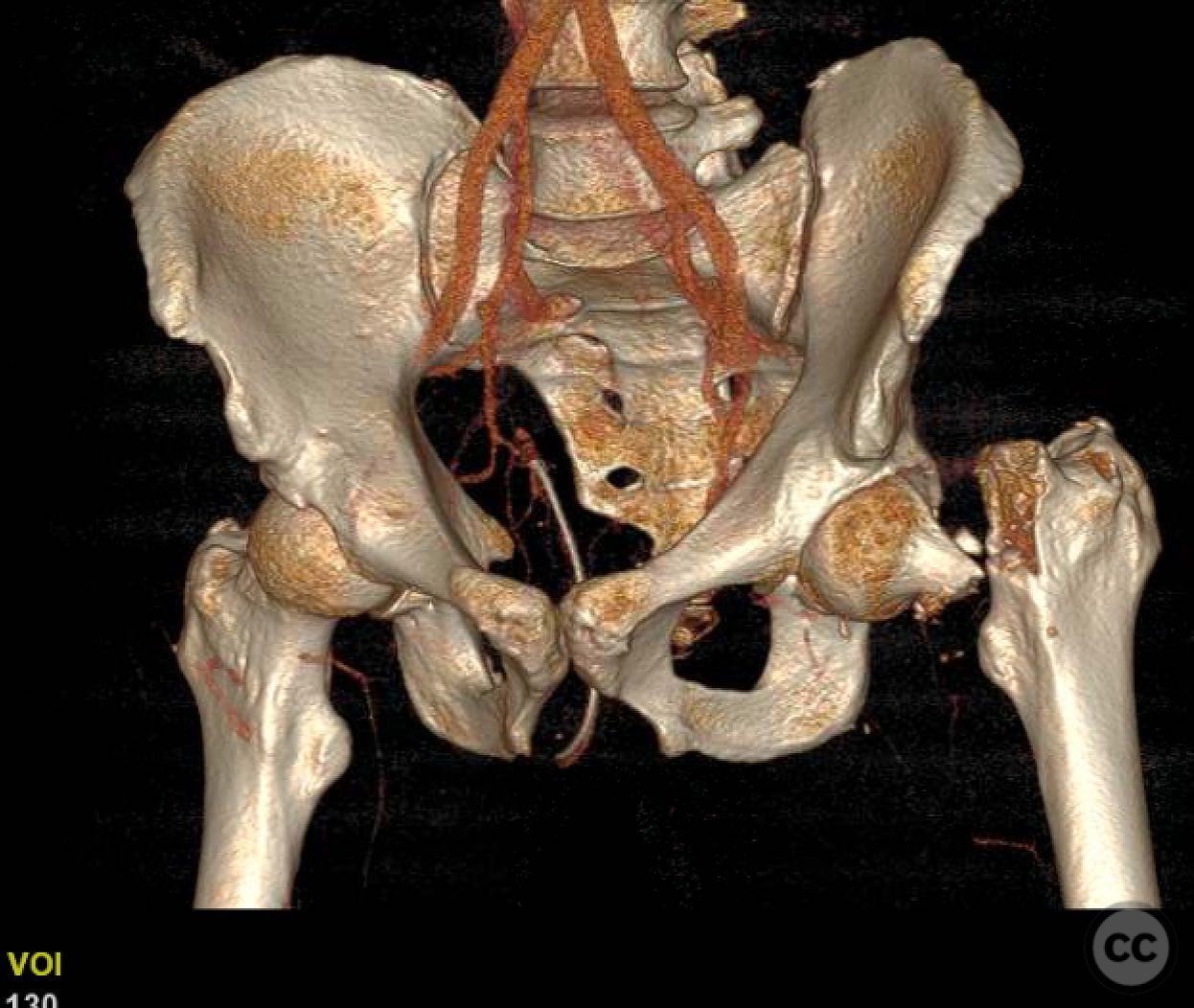
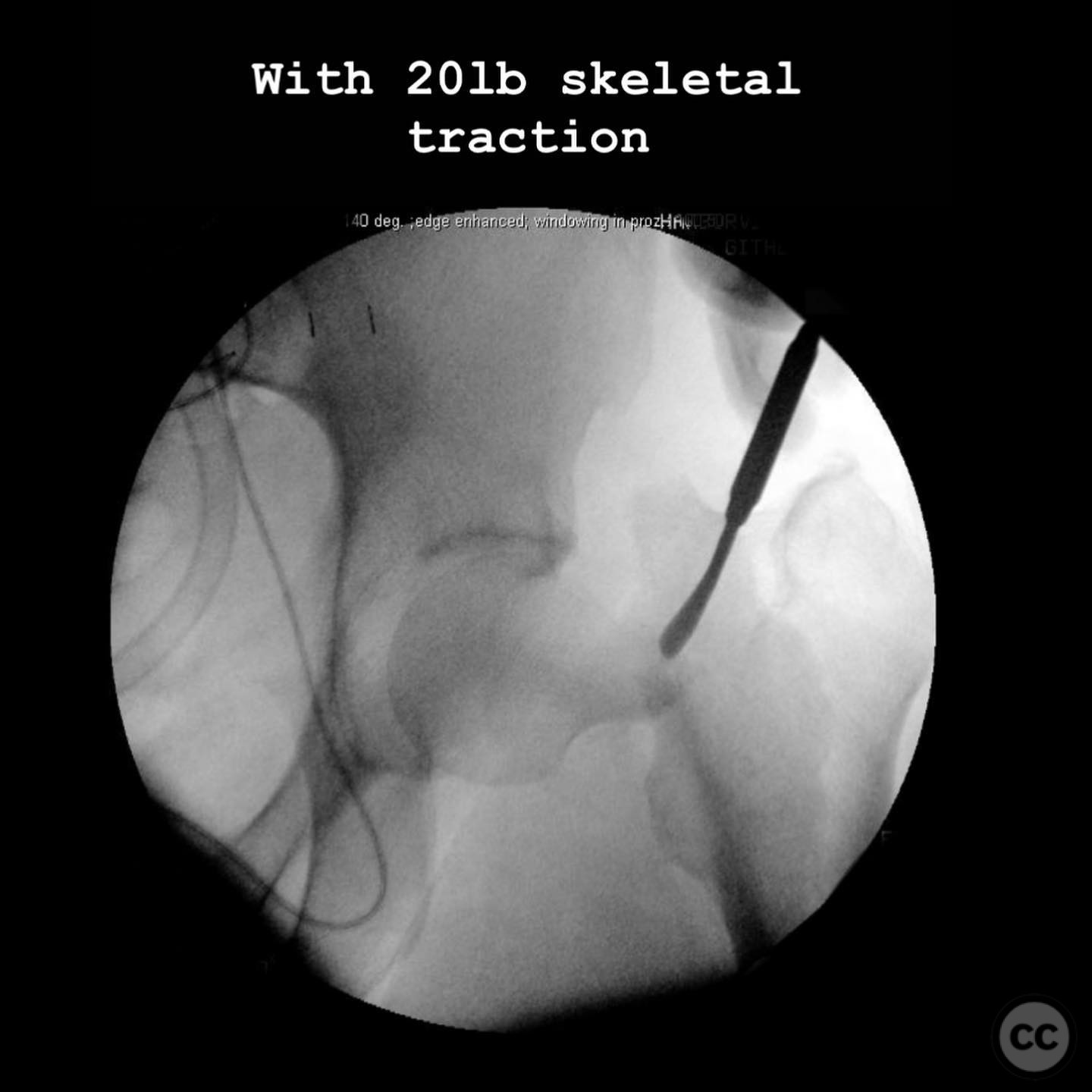
Clinical and radiological findings: A 41-year-old male sustained a high-energy vertical displaced femoral neck fracture following a high-speed motorcycle accident. The injury is characterized by significant displacement with unusual shortening, varus, and retroversion, but with fragments not in contact. Initial radiographs and traction views showed no improvement in alignment, indicating the necessity for open reduction. The risk of avascular necrosis (AVN) is elevated due to the displacement pattern.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction via the Heuter approach for fracture exposure and reduction, followed by a subvastus approach for implant placement. The surgical strategy was to achieve anatomical reduction and stable fixation to preserve the native hip joint, considering the patient's young age and the potential risks of AVN.
Surgical Discussion
Patient positioning: The patient was positioned supine on a traction table, although traction was not effective in improving fracture alignment preoperatively.
Anatomical surgical approach: The surgical approach commenced with the Heuter approach, involving an incision over the anterior aspect of the hip joint. Due to significant deformity and muscular build, a rectus femoris tenotomy was performed to facilitate exposure of the cranially displaced fracture. Following reduction, a subvastus approach was utilized for lateral access to the femur, allowing for precise placement of fixation devices.
Operative remarks:The surgeon noted that the degree of displacement made the Heuter approach less straightforward, necessitating a rectus tenotomy for adequate exposure. Preloading 2.0 and 2.4mm wires facilitated immediate fixation post-reduction, minimizing the risk of losing reduction during lateral approach preparation. The decision to fix rather than replace was based on preserving native joint function in this young patient, despite the elevated AVN risk.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing (NWB) status initially, progressing to partial weight bearing (PWB) as tolerated over 6-8 weeks, with gradual increase to full weight bearing (FWB) by 12 weeks post-surgery. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: 2.0mm and 2.4mm Kirschner wires for provisional fixation; definitive fixation details not specified.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 267 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Vertical Displaced Femoral Neck Fracture in a Young Male: Open Reduction and Internal Fixation. Journal of Orthopaedic Surgery and Traumatology. Case Report 36646305 Published Online Jul 14 2025.