












Low Velocity Ballistic Proximal Ulnar and Distal Humeral Fractures
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A young male patient sustained a low velocity ballistic injury resulting in fractures of the proximal ulna, trochlea, and capitellum. The entry wound was located on the dorsal proximal ulna, with an exit wound on the anterior brachium. There were no associated neurological or vascular injuries.
Preoperative Plan
Planning remarks: The preoperative plan involved a staged surgical approach. Initially, a posterior approach was planned to address the proximal ulna, including both the anteromedial facet and olecranon. Due to the complexity of the fracture pattern and the need for accurate reduction of the coronoid process, a second stage using a direct anterior approach was planned to access the anterior distal humeral articular surface and coronoid.
Surgical Discussion
Patient positioning: The patient was positioned prone for the initial posterior approach to the proximal ulna. For the second stage, the patient was repositioned supine to facilitate the direct anterior approach to the distal humerus.
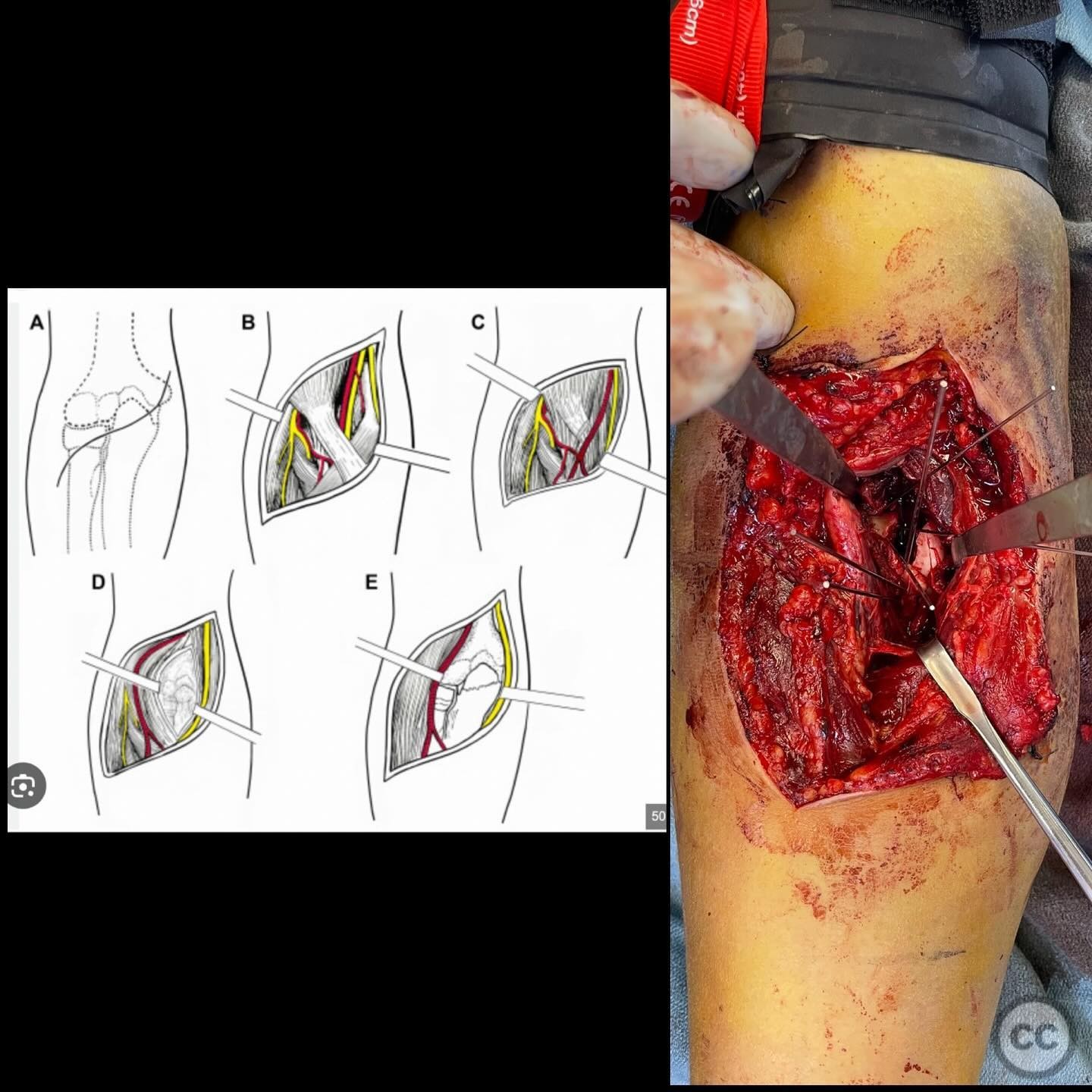
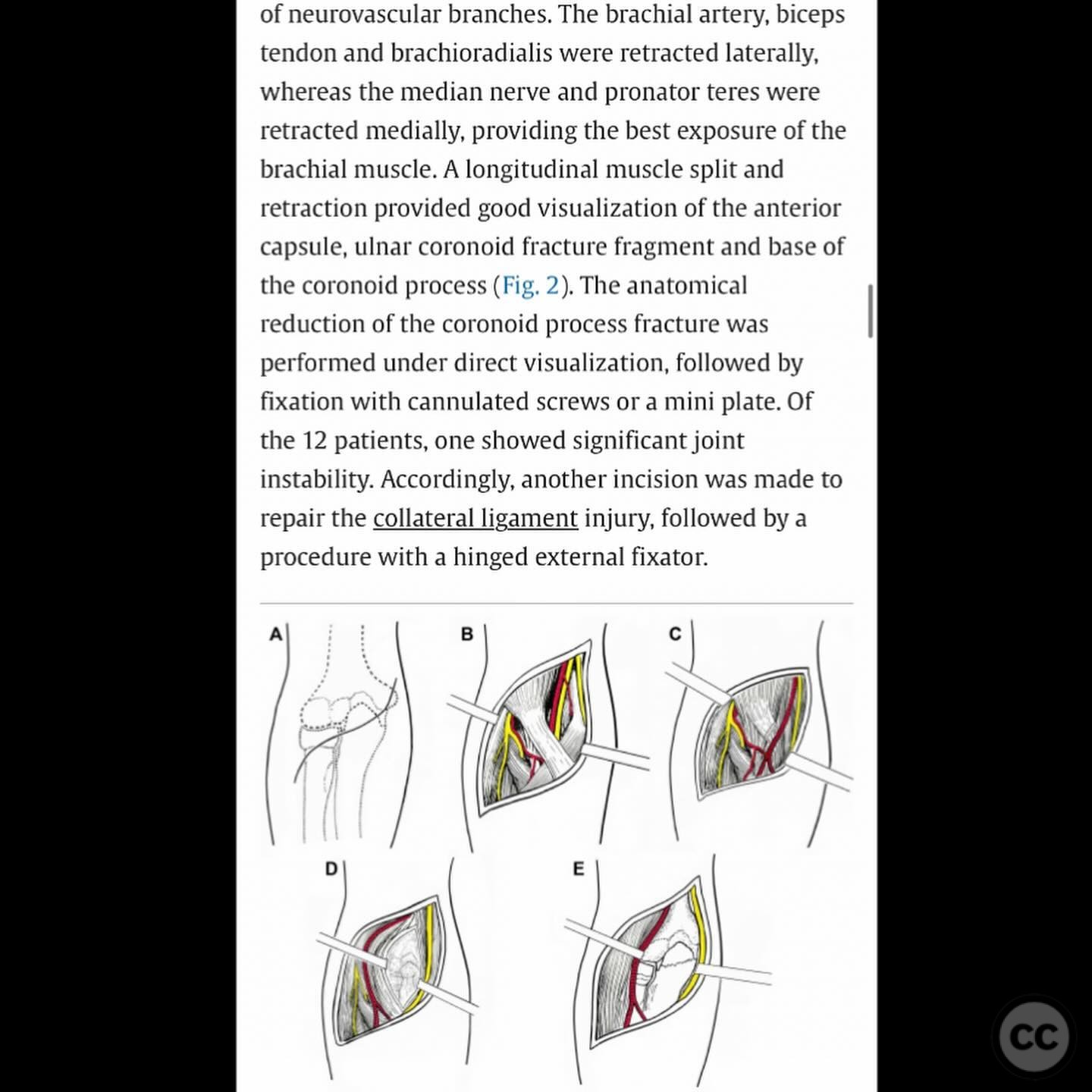
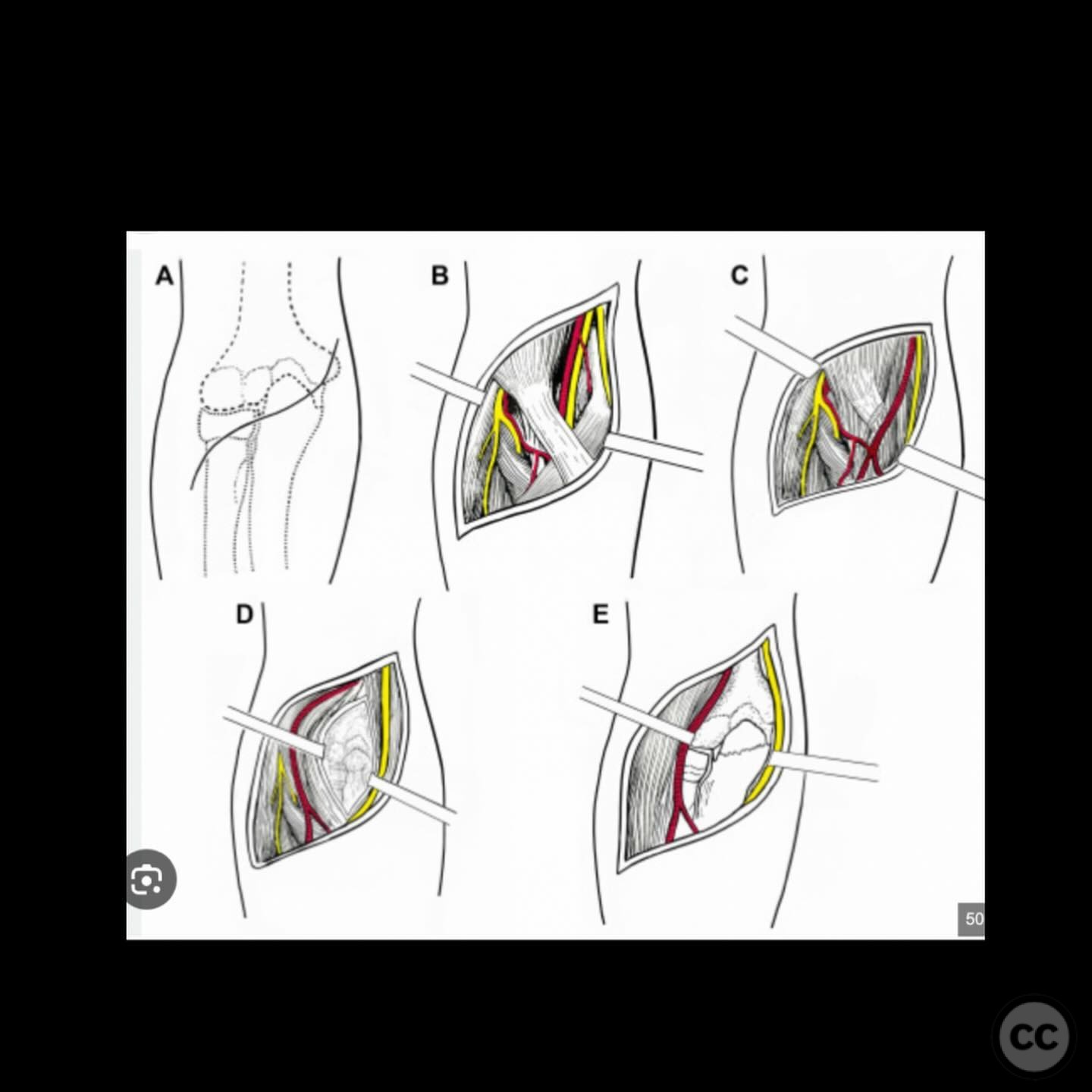
Anatomical surgical approach: The initial surgical approach was a posterior incision to expose the proximal ulna, including subperiosteal dissection around the olecranon and anteromedial facet. The second stage involved a direct anterior approach, providing access to the entire anterior distal humeral articular surface and coronoid process.
Operative remarks:The surgeon noted that the free anterior distal humeral articular fragments and residual void presented a significant challenge for access and fixation. Initially, there was consideration for cement reconstruction with potential delayed structural osteochondral grafting; however, large fixable fragments were identified intraoperatively. The distal humerus was repaired first due to improved visualization provided by the displaced coronoid. The coronoid was subsequently reduced and fixed with a buttressing plate. The surgeon emphasized the importance of careful preoperative planning and staging of the procedure to ensure accurate reduction and fixation.
Postoperative protocol: Postoperative rehabilitation included early mobilization with a focus on achieving a functional motion arc. At 6 months postoperatively, the patient demonstrated a stable, pain-free elbow with a motion arc of 10-125 degrees.
Follow up: Not specified.
Orthopaedic implants used: Buttressing plate for coronoid fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 301 times
10 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Low Velocity Ballistic Proximal Ulnar and Distal Humeral Fractures. Journal of Orthopaedic Surgery and Traumatology. Case Report 36158512 Published Online Jul 10 2025.