






Complex Both Column Acetabular Fracture with Dome and Parasymphyseal Involvement
Score and Comment on this Case
Clinical Details
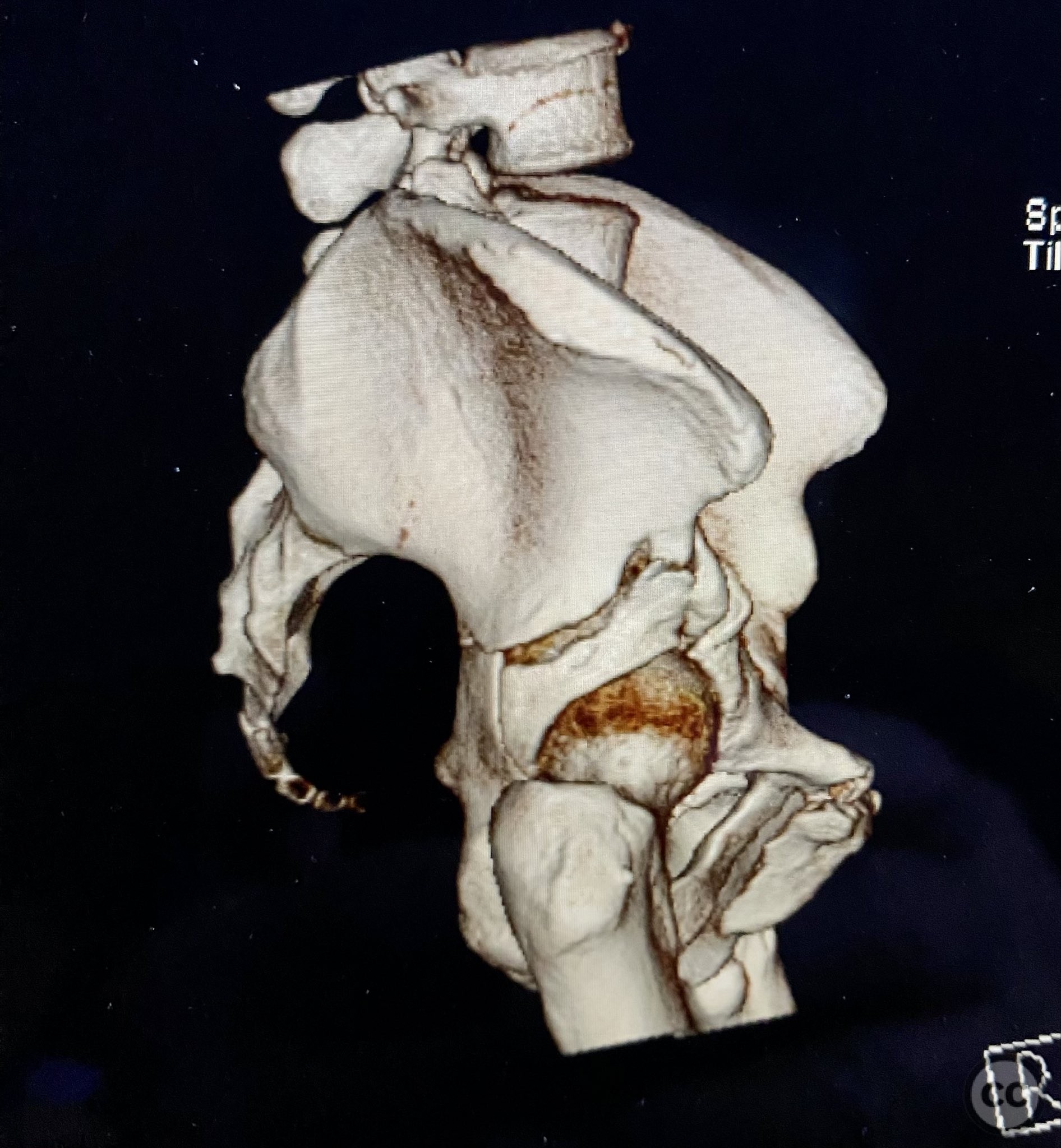
Clinical and radiological findings: The patient sustained a complex both column acetabular fracture, AO/OTA 62C1, characterized by several large columnar fragments, an independent anterior inferior iliac spine (AIIS) fragment, a notable dome fragment predominantly attached to the posterior wall (PW) fragment, and a distinct parasymphyseal injury zone. Initial application of a pelvic binder resulted in increased displacement of the fracture fragments. Preoperative imaging, including surface renderings and multiplanar CT, demonstrated the independent AIIS fragment, detailed cortical surfaces, and the orientation of fracture planes. The majority of the acetabular dome was associated with the PW fragment, a critical detail for surgical planning and reduction.
Preoperative Plan
Planning remarks: The preoperative plan involved an ilioinguinal approach to facilitate direct visualization, cleaning, and reduction of the cortical and fracture surfaces. The reduction sequence was planned as follows: first, anatomical reduction and provisional fixation of the anterior column (AC) fragment using a 6-hole plate and lag screw; second, application of a 12-hole intrapelvic plate for additional stabilization; third, definitive stabilization of the posterior column (PC) and PW fragments with lag screws. No additional exposures were planned.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table to allow optimal access for the ilioinguinal approach and intraoperative fluoroscopic imaging.
Anatomical surgical approach: A standard ilioinguinal approach was utilized. The incision was made parallel to the inguinal ligament, extending from just lateral to the anterior superior iliac spine (ASIS) to the pubic tubercle. Dissection proceeded through the subcutaneous tissue and external oblique aponeurosis. The abdominal musculature was retracted to expose the iliopsoas muscle and neurovascular bundle. Three operative windows were developed: lateral (between the iliac vessels and iliopsoas), middle (between the external iliac vessels and spermatic cord/round ligament), and medial (between the external iliac vessels and bladder). Fracture surfaces were meticulously debrided, and reduction clamps were applied as needed for provisional stabilization.
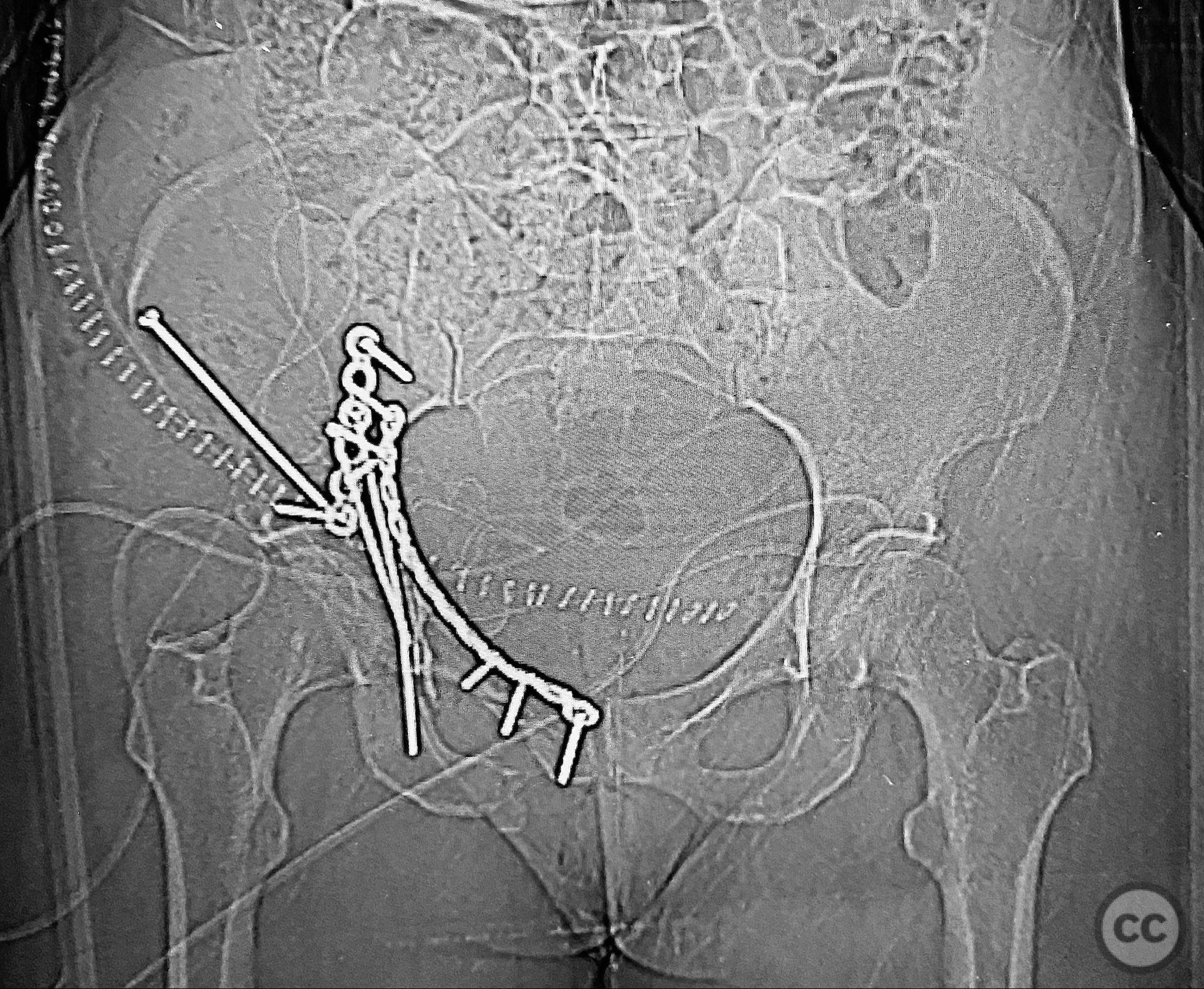
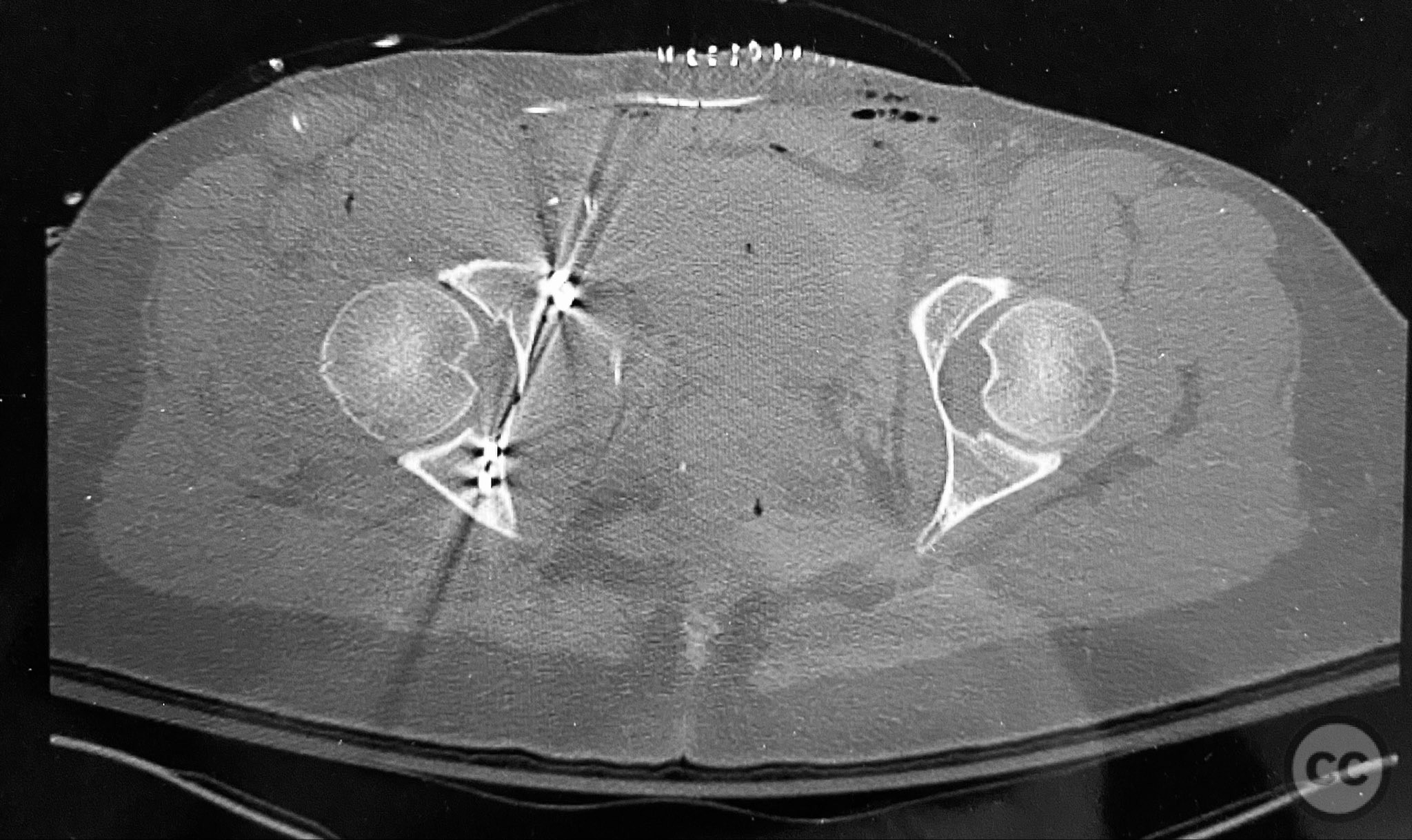
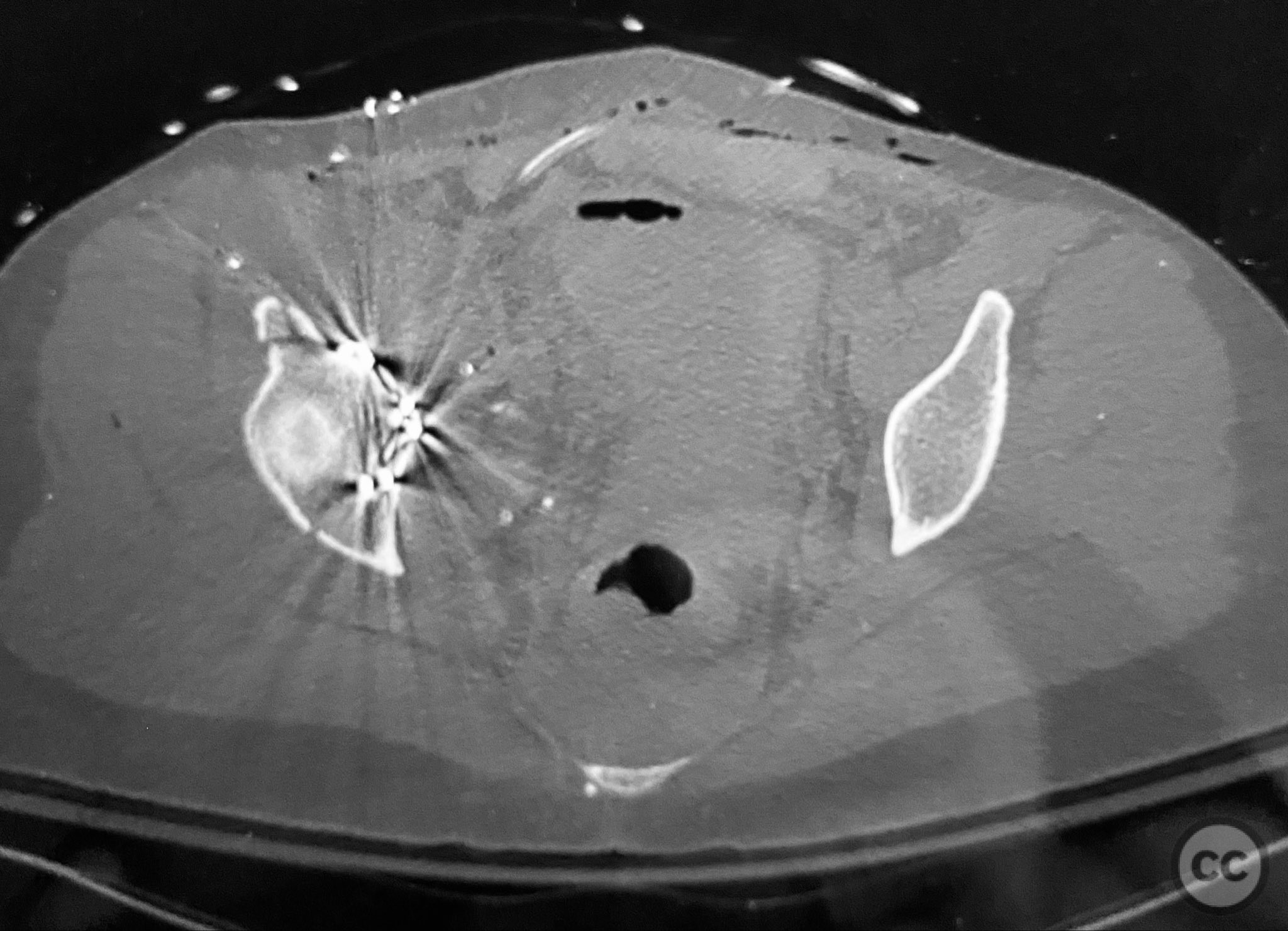
Operative remarks:The anterior column fragment was reduced first under direct visualization and held with a 6-hole plate and lag screw. The 12-hole intrapelvic plate was then contoured and applied along the pelvic brim to reinforce the reduction. The posterior column and posterior wall fragments, including the dome component, were stabilized with lag screws placed through safe osseous corridors under fluoroscopic guidance. The independent AIIS fragment was addressed during the exposure and incorporated into the reduction construct. The parasymphyseal injury zone was inspected for stability following fixation. Postoperative CT confirmed anatomical reduction and stable fixation of all fragments.
Postoperative protocol: For the initial six weeks postoperatively, the patient was instructed to maintain limited weight bearing with crutches to protect the repair. From postoperative weeks 7 to 12, a licensed physical therapist supervised progressive rehabilitation focused on range of motion, strengthening, and gradual return to full weight bearing.
Follow up: Not specified
Orthopaedic implants used: 6-hole reconstruction plate, 12-hole intrapelvic plate, multiple lag screws
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 1055 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Complex Both Column Acetabular Fracture with Dome and Parasymphyseal Involvement. Journal of Orthopaedic Surgery and Traumatology. Case Report 34912207 Published Online Sep 12 2025.