






Spinopelvic Dissociation with Sacral H-Type Fracture in a Young Adult.
Score and Comment on this Case
Clinical Details
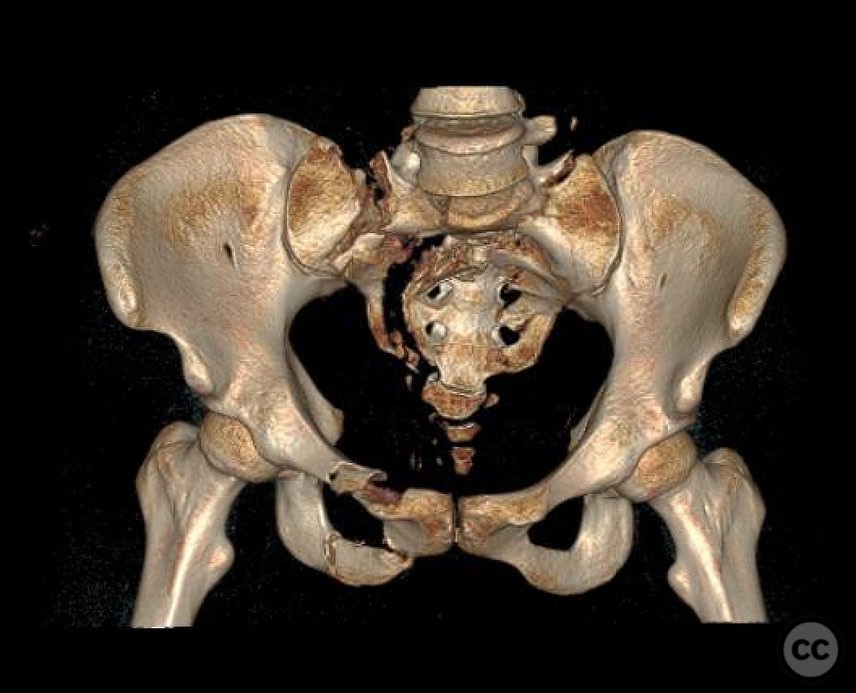
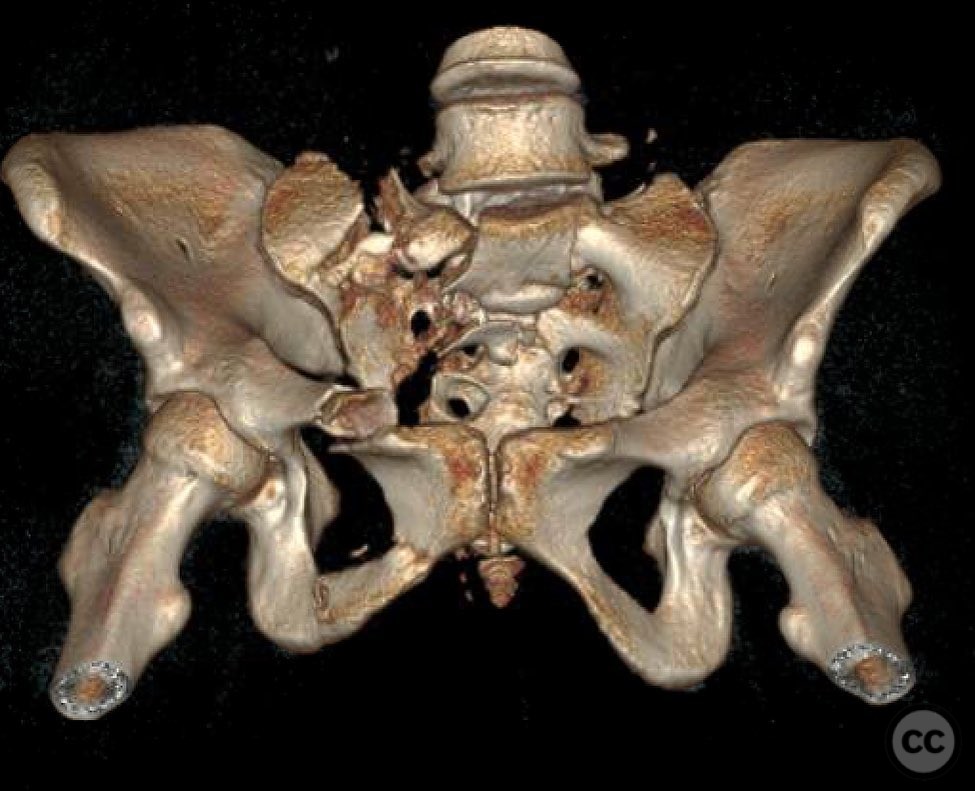
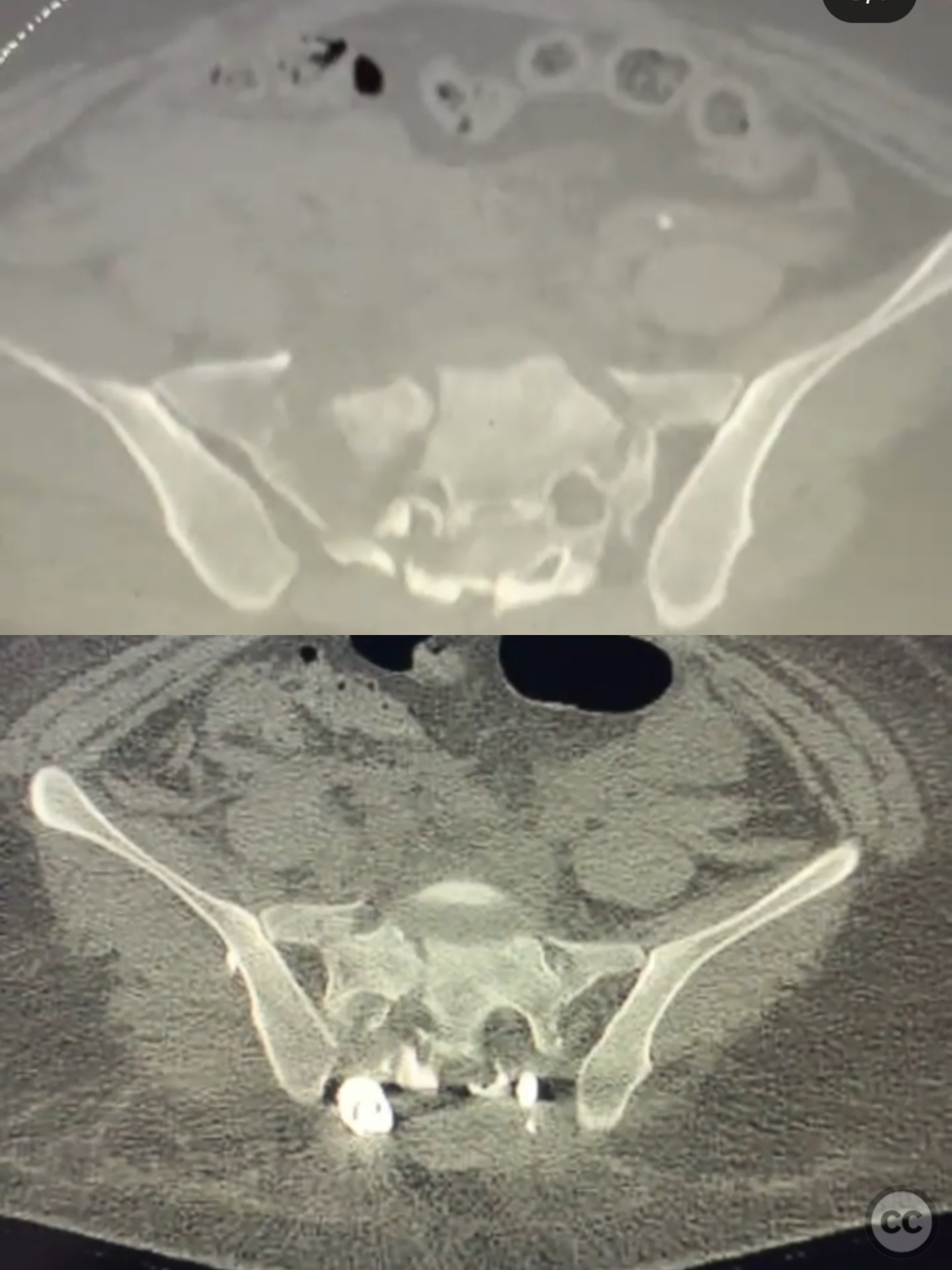
Clinical and radiological findings: A 22-year-old female sustained a fall from a height of 30 feet, resulting in bilateral open calcaneal fractures, an open segmental tibial fracture, and a spinopelvic dissociation with a sacral H-type fracture. The patient had no head, chest, or abdominal injuries. Initial management included debridement, irrigation, and external fixation of the calcaneal fractures, and debridement, irrigation, and intramedullary nailing of the tibial fracture. The patient was adequately resuscitated prior to addressing the pelvic injury. Neurological examination focused on L5 and below, with particular attention to bowel and bladder function due to potential kyphotic deformity and retropulsion.
Preoperative Plan
Planning remarks: The preoperative plan involved a two-stage approach: first, reduction and anterior plating of the pelvis to achieve partial indirect reduction of the sacral fracture; second, prone positioning for sacral lateral fluoroscopic imaging to assess kyphosis reduction. If necessary, open reduction and decompression would be performed, followed by transiliac transsacral screw placement and lumbopelvic fixation.
Surgical Discussion
Patient positioning: The patient was positioned prone for the posterior surgical approach, allowing assessment of sacral kyphosis reduction with lateral fluoroscopy.
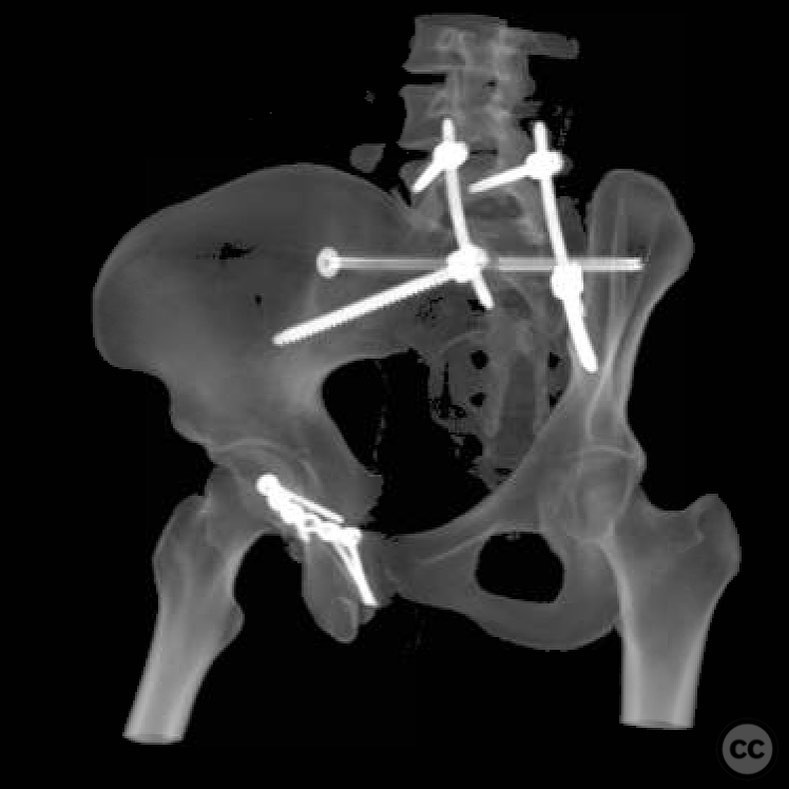
Anatomical surgical approach: A midline posterior approach was utilized for sacral exposure. Following prone positioning, the sacral kyphosis reduced adequately, allowing safe placement of an S1 guidewire. An O-arm was used for intraoperative navigation. A partially threaded screw was inserted to indirectly reduce sacral width without excessive compression. The spine team then performed decompression and percutaneous lumbopelvic fixation.
Operative remarks:The surgeon noted that prone positioning facilitated satisfactory reduction of the sacral kyphosis, preserving a safe S1 corridor for screw placement. The use of percutaneous techniques minimized infection risk associated with posterior sacral approaches. The spine team successfully avoided placing an iliac bolt in the sacroiliac joint.
Postoperative protocol: Postoperative rehabilitation included early mobilization with weight-bearing as tolerated, focusing on maintaining spinal alignment and preventing complications associated with prolonged immobility.
Follow up: Not specified.
Orthopaedic implants used: Partially threaded sacral screw, transiliac transsacral screw, percutaneous lumbopelvic fixation system.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 346 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Spinopelvic Dissociation with Sacral H-Type Fracture in a Young Adult.. Journal of Orthopaedic Surgery and Traumatology. Case Report 34732963 Published Online Jul 21 2025.