_ Displacement(s)_ Can you c_5.jpg)
_ Displacement(s)_ Can you c_2.jpg)
_ Displacement(s)_ Can you c_1.jpg)
_ Displacement(s)_ Can you cl(.jpg)
_ Displacement(s)_ Can you c_3.jpg)
_ Displacement(s)_ Can you c_4.jpg)

High Energy Pelvic Ring Disruption with Sacral Fracture and Symphysis Disruption
Score and Comment on this Case
Clinical Details
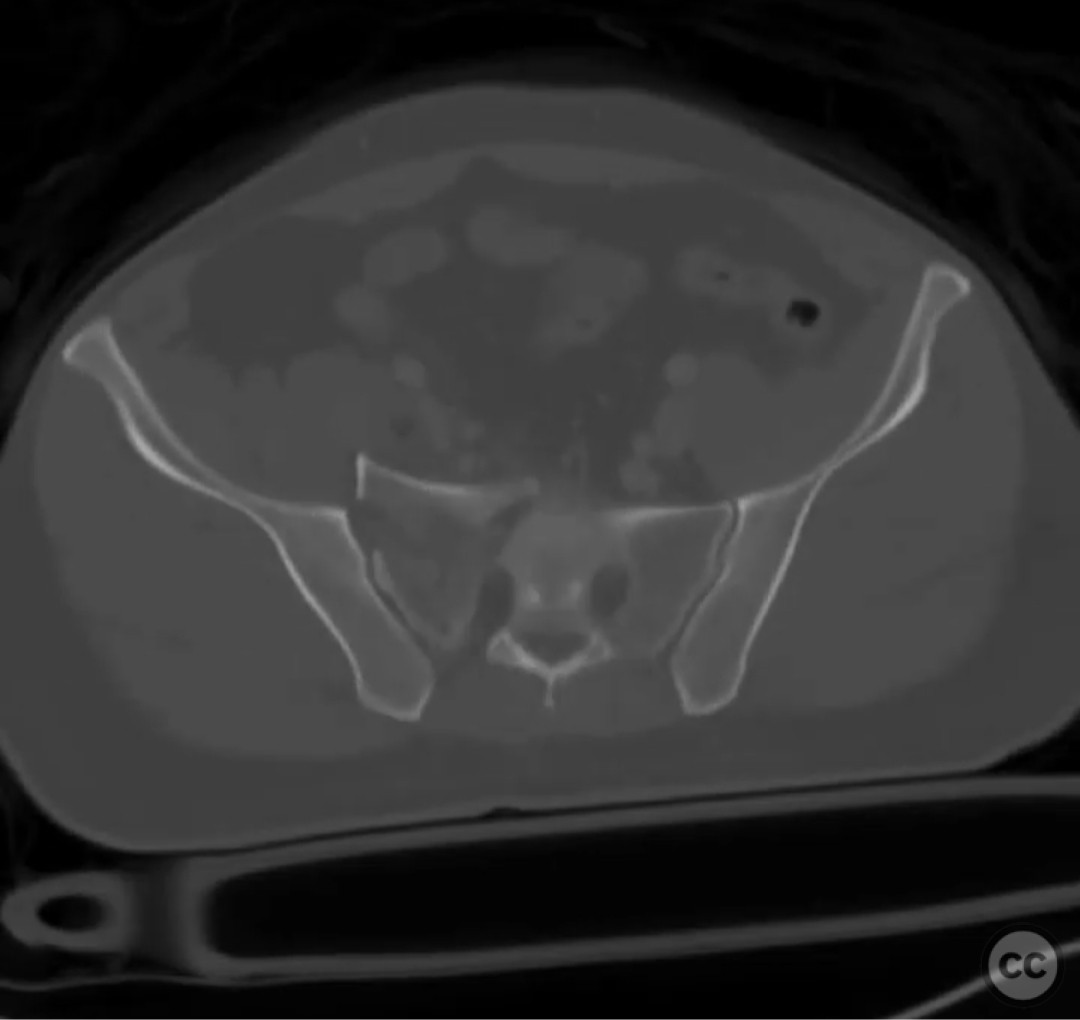
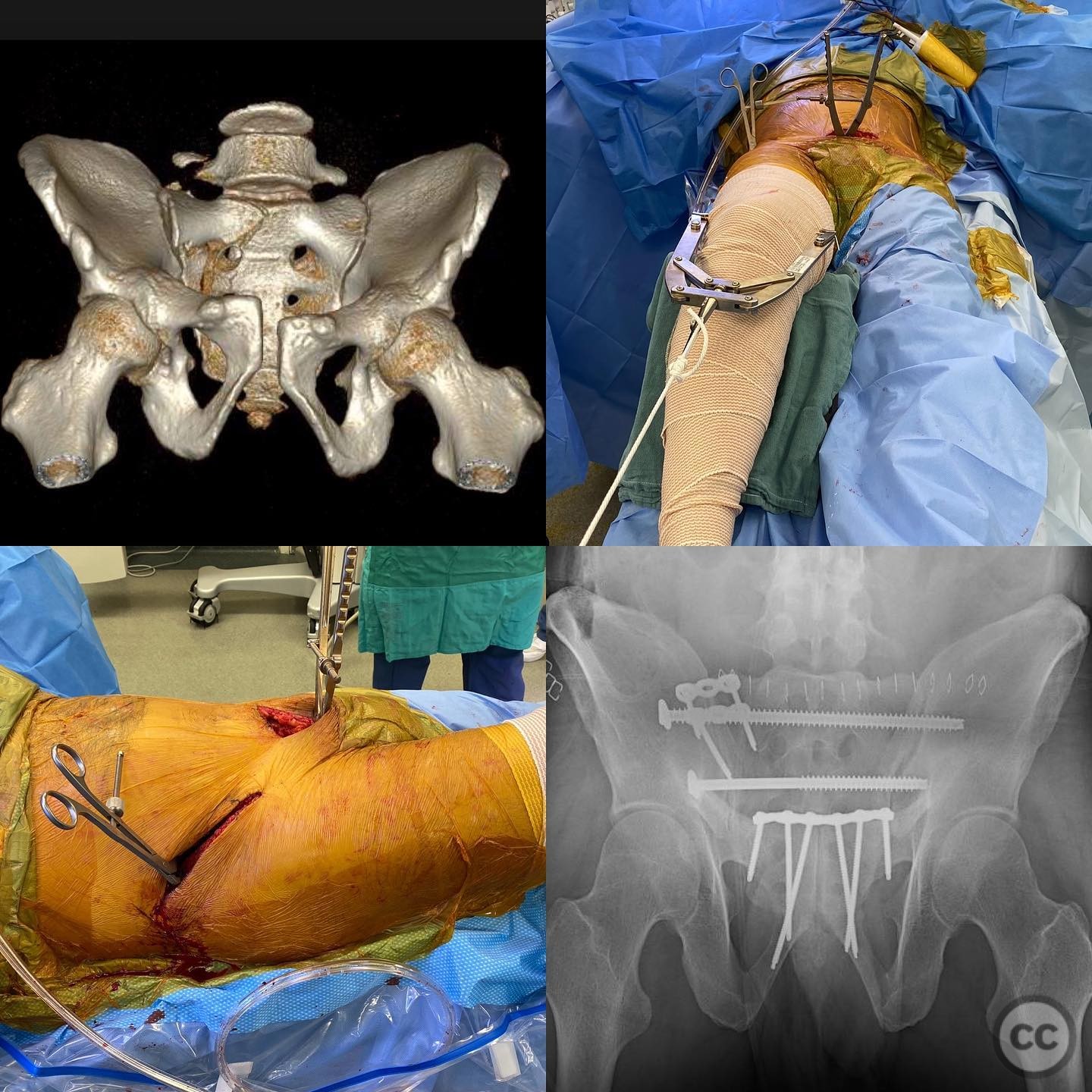
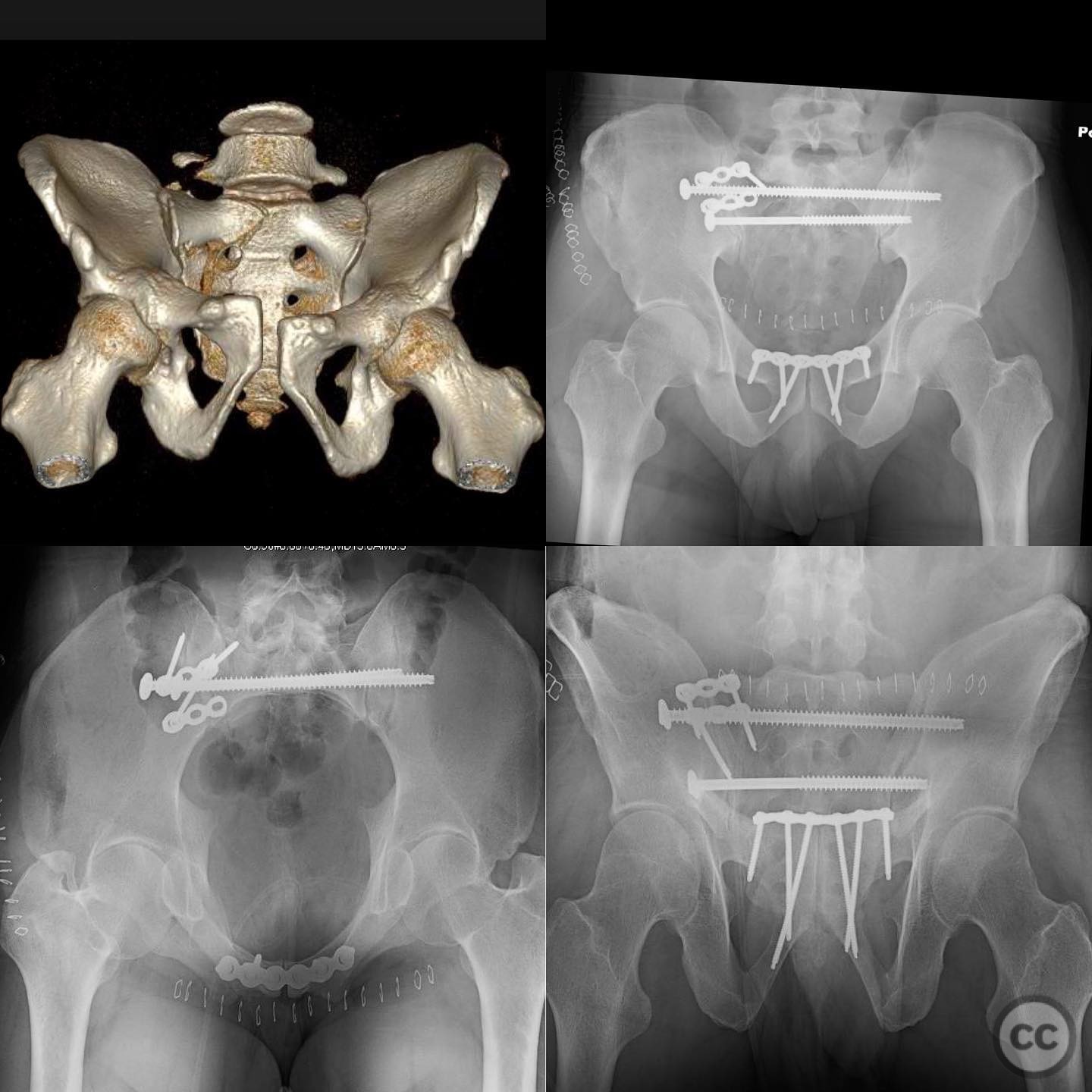
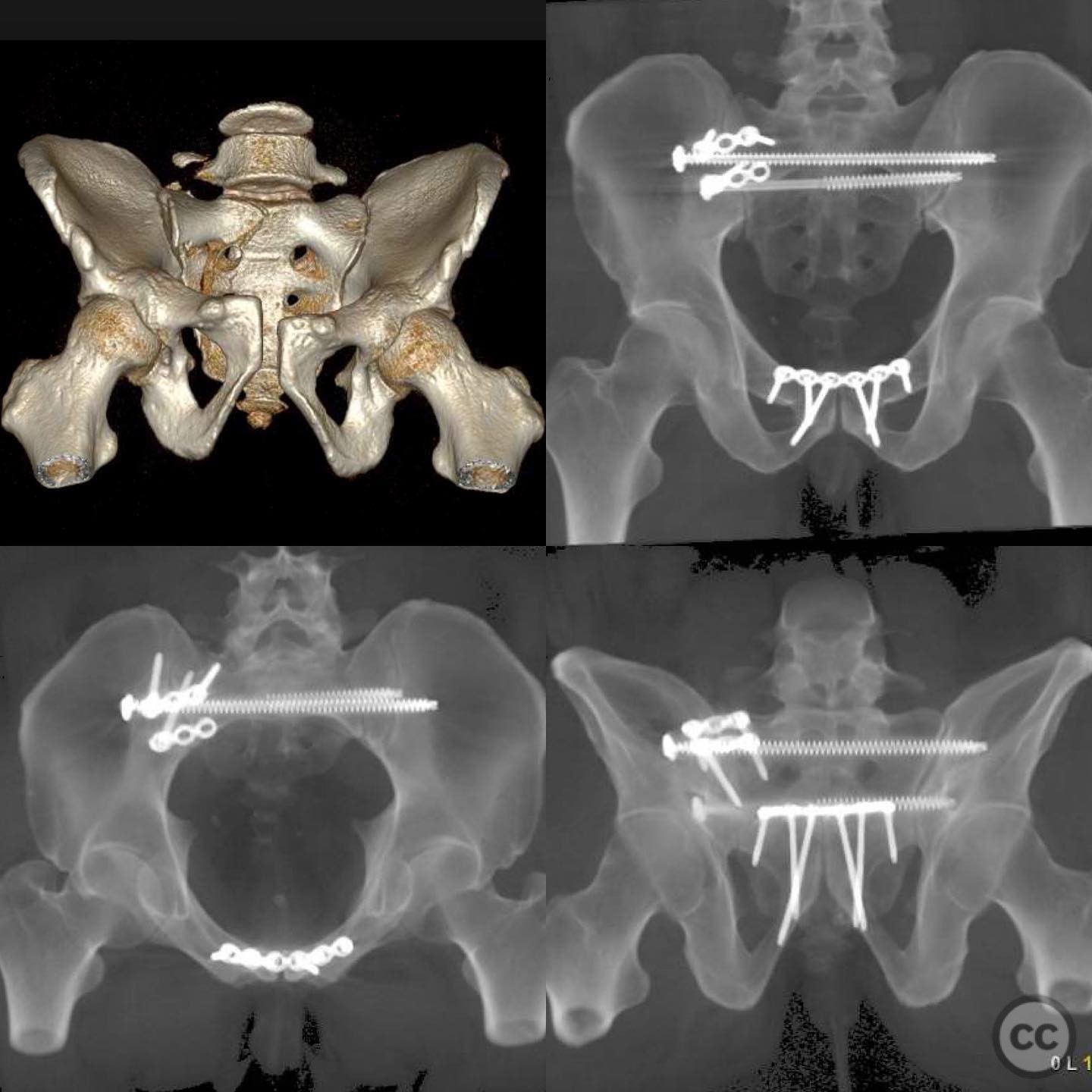
Clinical and radiological findings: A 38-year-old male sustained an isolated injury from a fall from the second story, resulting in a highly unstable pelvic ring. Radiological assessment revealed a complete sacral fracture with a large anteriorly dislocated fragment and posterior tension failure, along with symphysis pubis disruption. The hemipelvis was significantly flexed, indicating primary instability in the sagittal plane rotation. The injury pattern corresponds to a Tile C classification.
Preoperative Plan
Planning remarks: The preoperative plan involved open surgical approaches to both the sacral fracture and the symphysis pubis. Skeletal traction was applied preoperatively. The reduction of the sacral fragment and stabilization of the pelvic ring were prioritized, with simultaneous work through both approaches deemed necessary.
Surgical Discussion
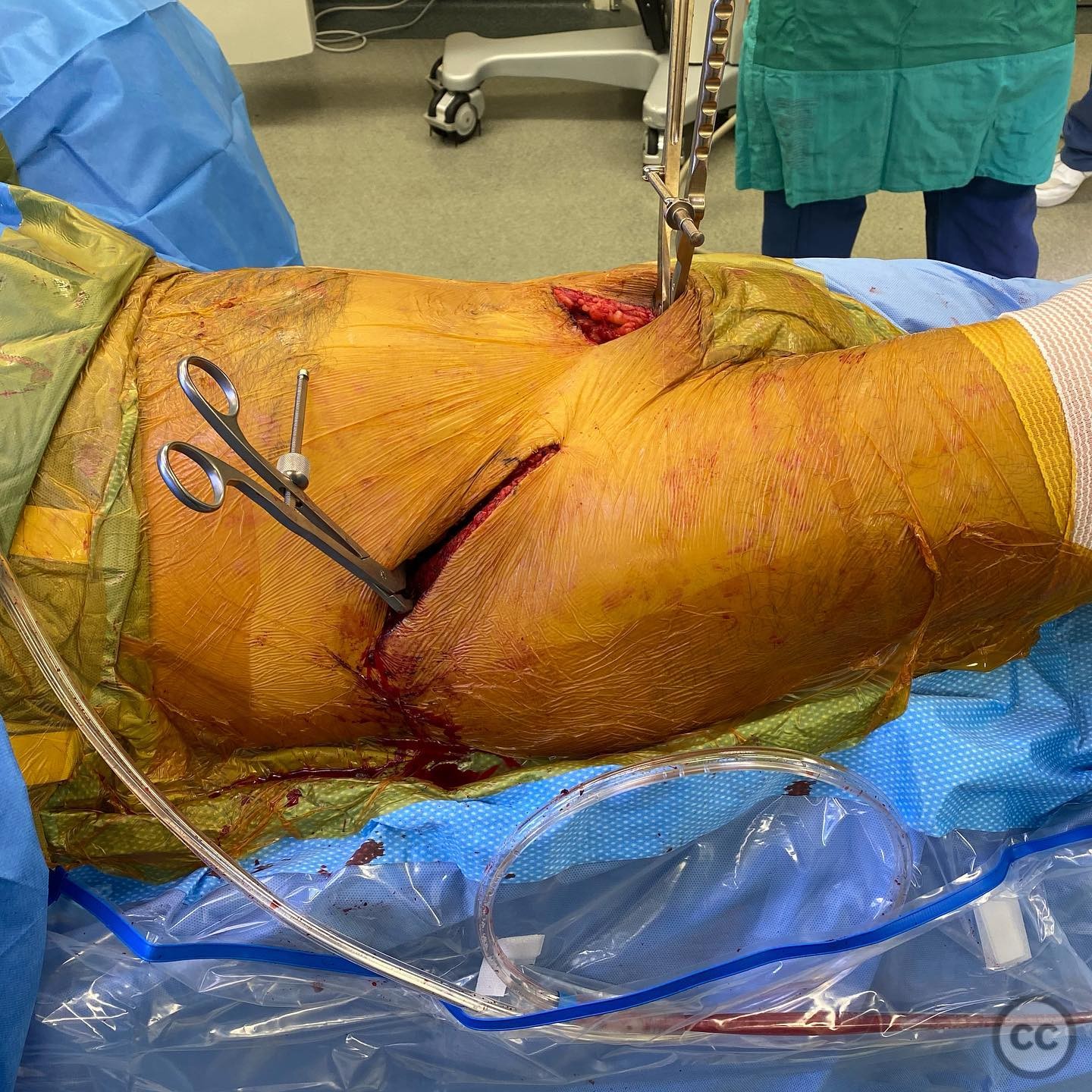
Patient positioning: The patient was positioned supine on the operating table to facilitate access to both the anterior and posterior pelvic structures.
Anatomical surgical approach: An anterior approach to the symphysis pubis was performed, allowing for direct visualization and reduction using a Jungbluth clamp for controlling multiplanar instability. A posterior approach to the sacrum was executed, with careful exposure of the dislocated sacral fragment and visualization of the L5 nerve root.
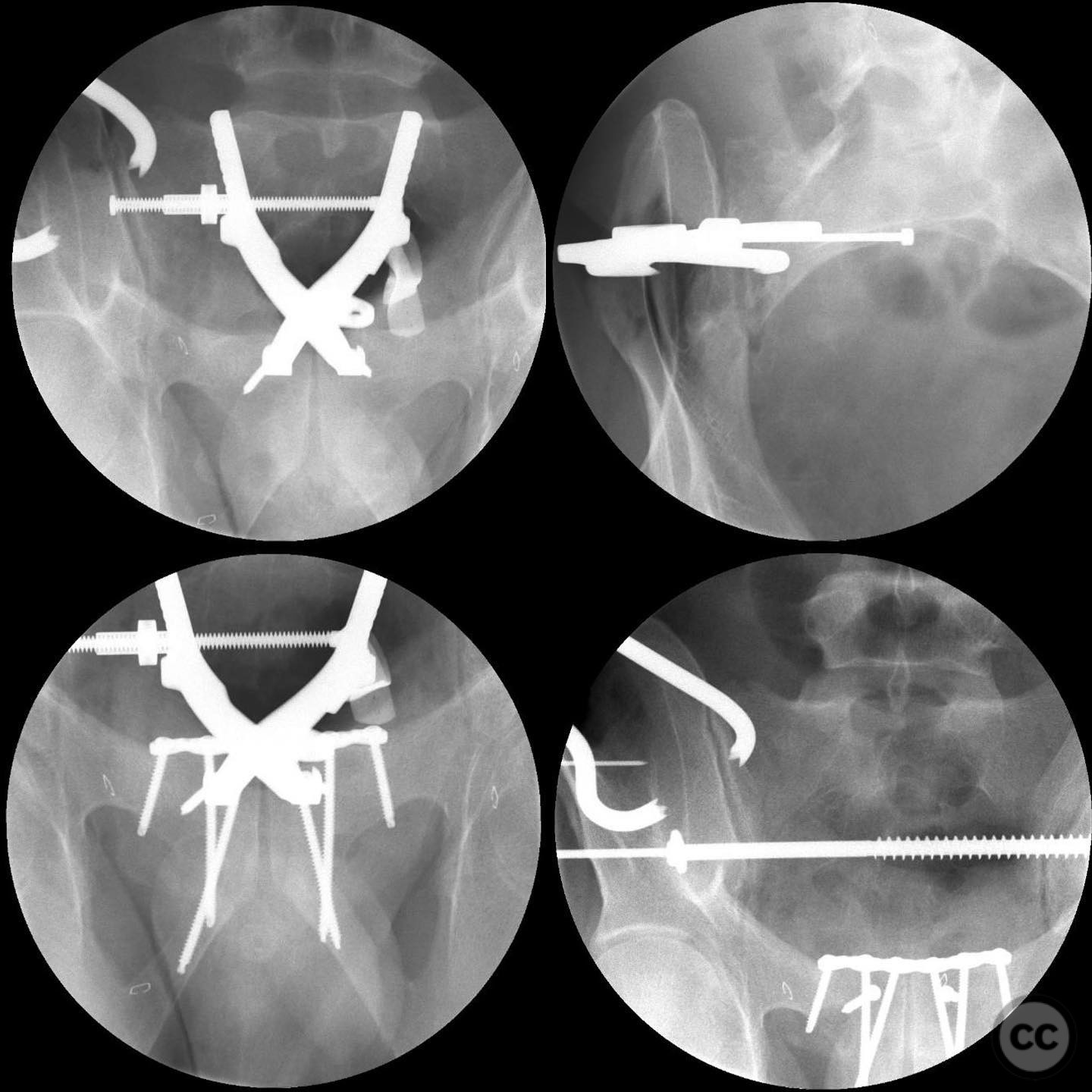
Operative remarks:The surgeon noted that the dislocated sacral fragment required careful exposure, with respect given to the L5 nerve root. Reduction of the sacral fragment and sacroiliac joint was achieved using a goose clamp. Sacral fixation was performed with an S2 screw for compression and an S1 screw for additional stability, followed by the application of two reconstruction plates to maintain reduction of the anterior sacral fragment. Sacral screws were placed prior to plating to avoid interference with screw corridors.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing on the affected side initially, progressing to partial weight bearing as tolerated, with close monitoring of fracture healing and stability.
Follow up: Not specified.
Orthopaedic implants used: S2 screw, S1 screw, two reconstruction plates.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Guest User
Great work sir.