














Bicondylar Tibial Plateau Fracture with Meta-Diaphyseal Extension in a Multiply Injured Patient
Score and Comment on this Case
Clinical Details
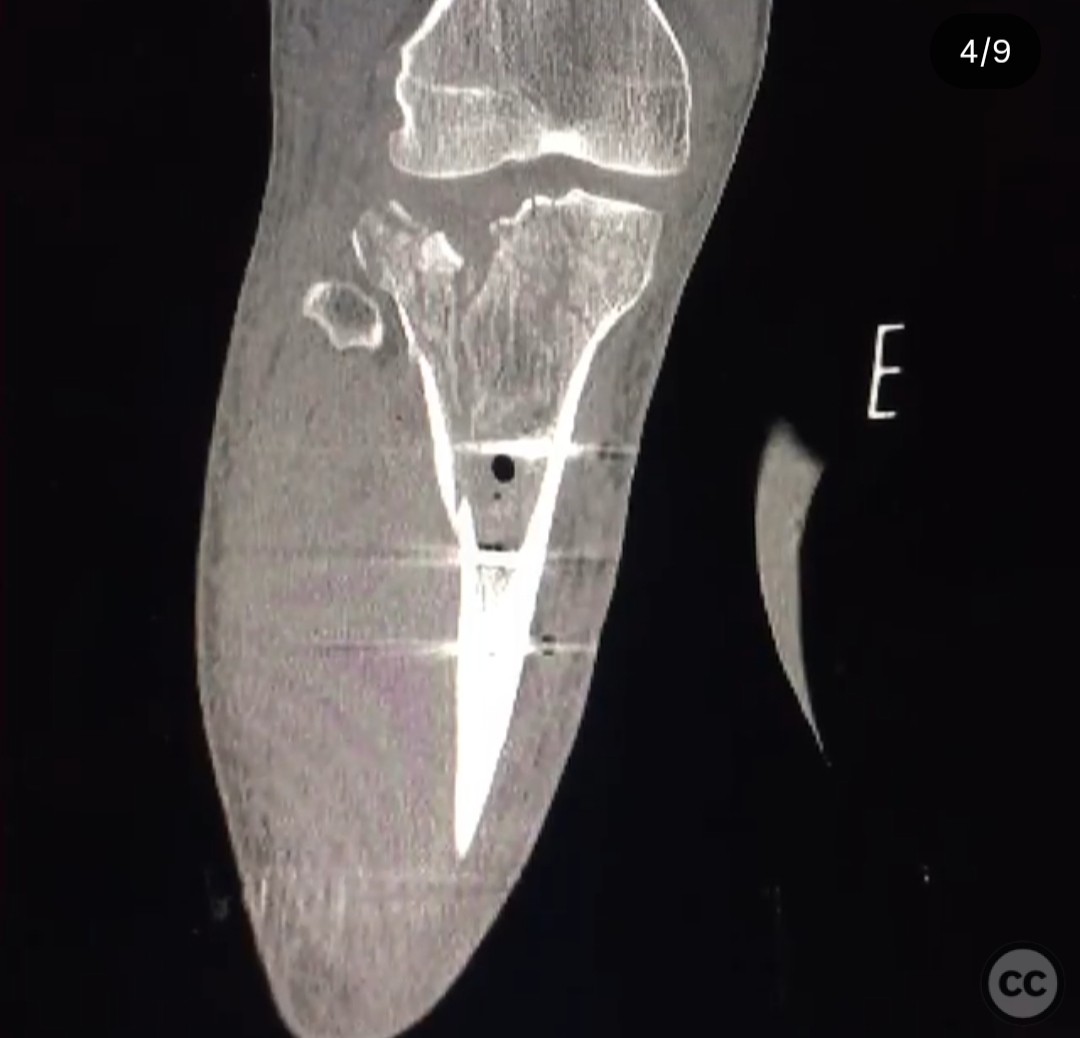
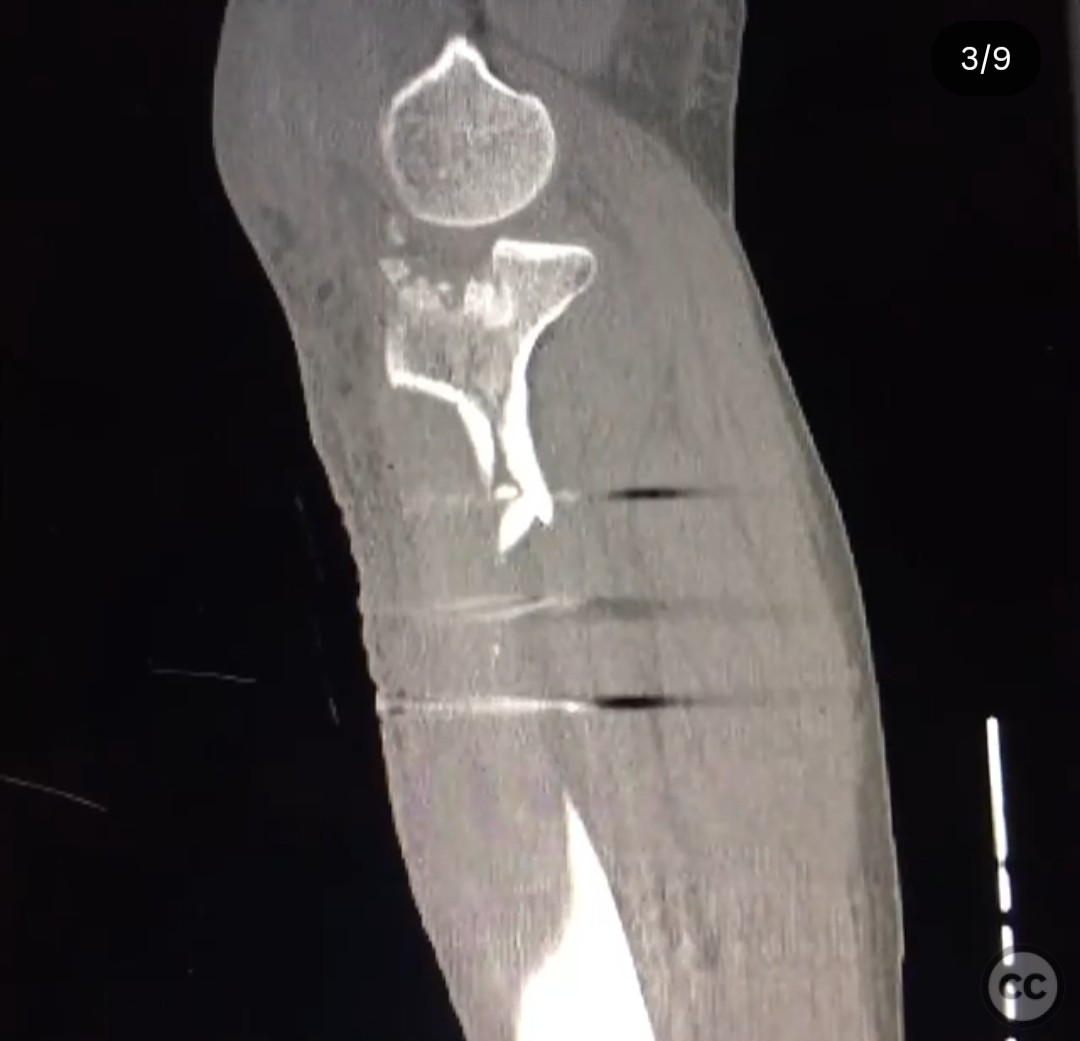
Clinical and radiological findings: A 27-year-old male sustained multiple injuries in a high-speed motorcycle collision, including a bicondylar tibial plateau fracture with long simple meta-diaphyseal extension, contralateral Schatzker IV fracture, scapula/glenoid neck fracture, olecranon fracture, grade 2 splenic laceration, and rib fractures with hemopneumothorax. The patient was stable on day one for surgical intervention. Initial radiographs and CT imaging confirmed the bicondylar tibial plateau fracture with diaphyseal extension. The AO/OTA classification for this fracture is 41-C2.
Preoperative Plan
Planning remarks: The preoperative plan involved early percutaneous reduction and fixation of the diaphyseal extension using percutaneous clamping and 3.5mm lag screws, followed by application of a knee-spanning external fixator. This approach aimed to stabilize the fracture and facilitate soft tissue recovery, with definitive open reduction and internal fixation planned once swelling subsided.
Surgical Discussion
Patient positioning: Supine position with the affected limb prepared for percutaneous intervention and external fixation.
Anatomical surgical approach: Percutaneous approach was utilized for the reduction of the diaphyseal component, employing small stab incisions in line with planned definitive surgical approaches. Percutaneous clamping was used to achieve reduction, followed by insertion of 3.5mm lag screws to stabilize the diaphyseal extension.
Operative remarks:The surgeon emphasized the importance of achieving accurate reduction of the diaphyseal component to prevent magnified mal-reduction at the joint level. The early stabilization with lag screws and external fixation was performed to accelerate soft tissue recovery and simplify the definitive operation. The definitive fixation involved open reduction of articular components and fragment-specific fixation once swelling allowed, approximately one week post-initial intervention.
Postoperative protocol: Postoperative rehabilitation included initial immobilization with the external fixator, followed by progressive weight-bearing as tolerated after definitive fixation. Early range of motion exercises were encouraged once stability was confirmed.
Follow up: Not specified.
Orthopaedic implants used: 3.5mm lag screws, knee-spanning external fixator.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 297 times
25 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Bicondylar Tibial Plateau Fracture with Meta-Diaphyseal Extension in a Multiply Injured Patient. Journal of Orthopaedic Surgery and Traumatology. Case Report 34086877 Published Online Jul 25 2025.