


Management of Proximal Tibial Bone and Skin Defect with Medial Gastrocnemius Flap and Ilizarov Technique
Score and Comment on this Case
Clinical Details
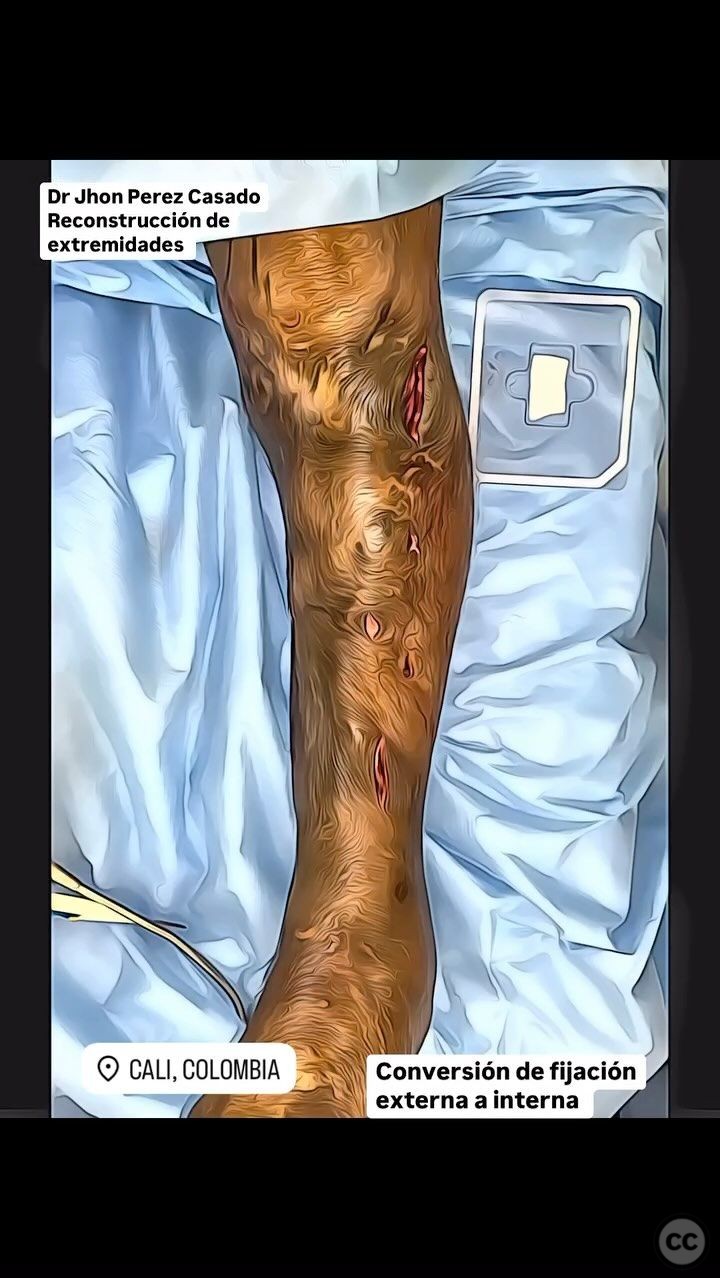
Clinical and radiological findings: The patient presented with an abandoned external fixator, a proximal tibial bone defect, and an associated skin defect. The initial clinical examination revealed a significant soft tissue defect overlying the proximal tibia. Radiological assessment confirmed the presence of a proximal tibial bone defect. The neurovascular examination was unremarkable.
Preoperative Plan
Planning remarks: The preoperative plan included the removal of the external fixator, thorough debridement of the affected area, and planning for a medial gastrocnemius flap with a skin island to address the soft tissue defect. A provisional cement spacer was to be placed to maintain space and provide temporary stability. Subsequent bone transport and lengthening using the Ilizarov technique were planned to address the bone defect.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the affected limb prepared and draped in a sterile fashion to allow access to both the anterior and posterior aspects of the leg.
Anatomical surgical approach: A longitudinal incision was made over the medial aspect of the proximal tibia. The medial gastrocnemius muscle was identified and elevated with care to preserve its neurovascular supply. A skin island was included in the flap design to cover the soft tissue defect. The flap was transposed to cover the defect, and a provisional cement spacer was placed within the bone defect.
Operative remarks:The surgeon noted that the medial gastrocnemius flap provided excellent coverage of the soft tissue defect. The provisional cement spacer was placed without difficulty, maintaining alignment and space for future bone transport. The subsequent stage involved the application of an Ilizarov external fixator for bone transport and lengthening.
Postoperative protocol: Postoperatively, the patient was instructed to maintain non-weight bearing on the affected limb. Range of motion exercises for adjacent joints were initiated early to prevent stiffness. Gradual weight-bearing was introduced as tolerated following consolidation of the transported bone segment.
Follow up: Not specified.
Orthopaedic implants used: Ilizarov external fixator, provisional cement spacer, morphogenetic protein (for conversion from external to internal fixation).
Search for Related Literature

Jhon Perez Casado
- Colombia , Cali - Valle del Cauca
- Area of Specialty - Lower Limb
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 376 times
23 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Perez Casado, J.J.. (2025). Management of Proximal Tibial Bone and Skin Defect with Medial Gastrocnemius Flap and Ilizarov Technique. Journal of Orthopaedic Surgery and Traumatology. Case Report 33496980 Published Online Jul 23 2025.