







Maisonneuve Fracture with Syndesmotic Injury.
Score and Comment on this Case
Clinical Details
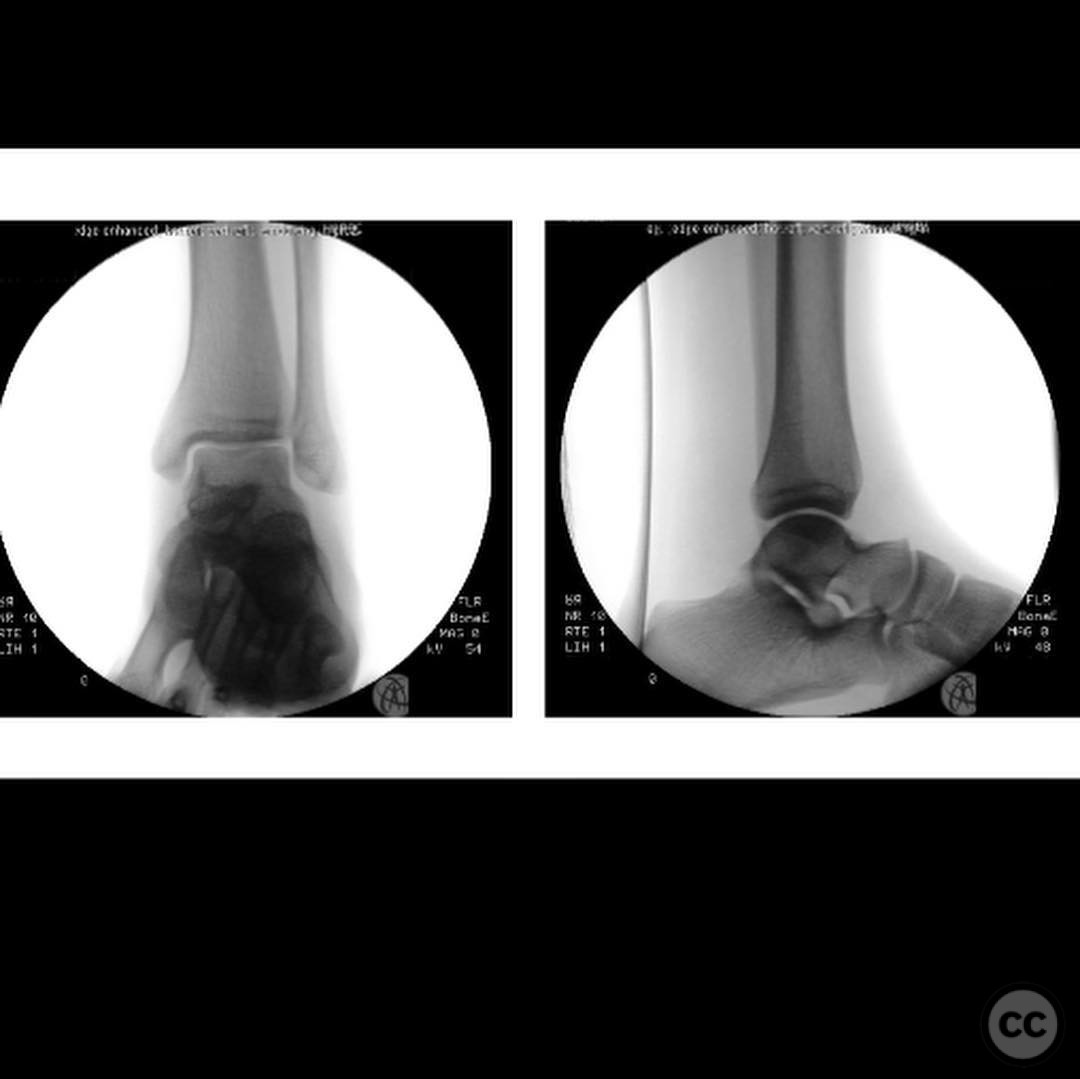
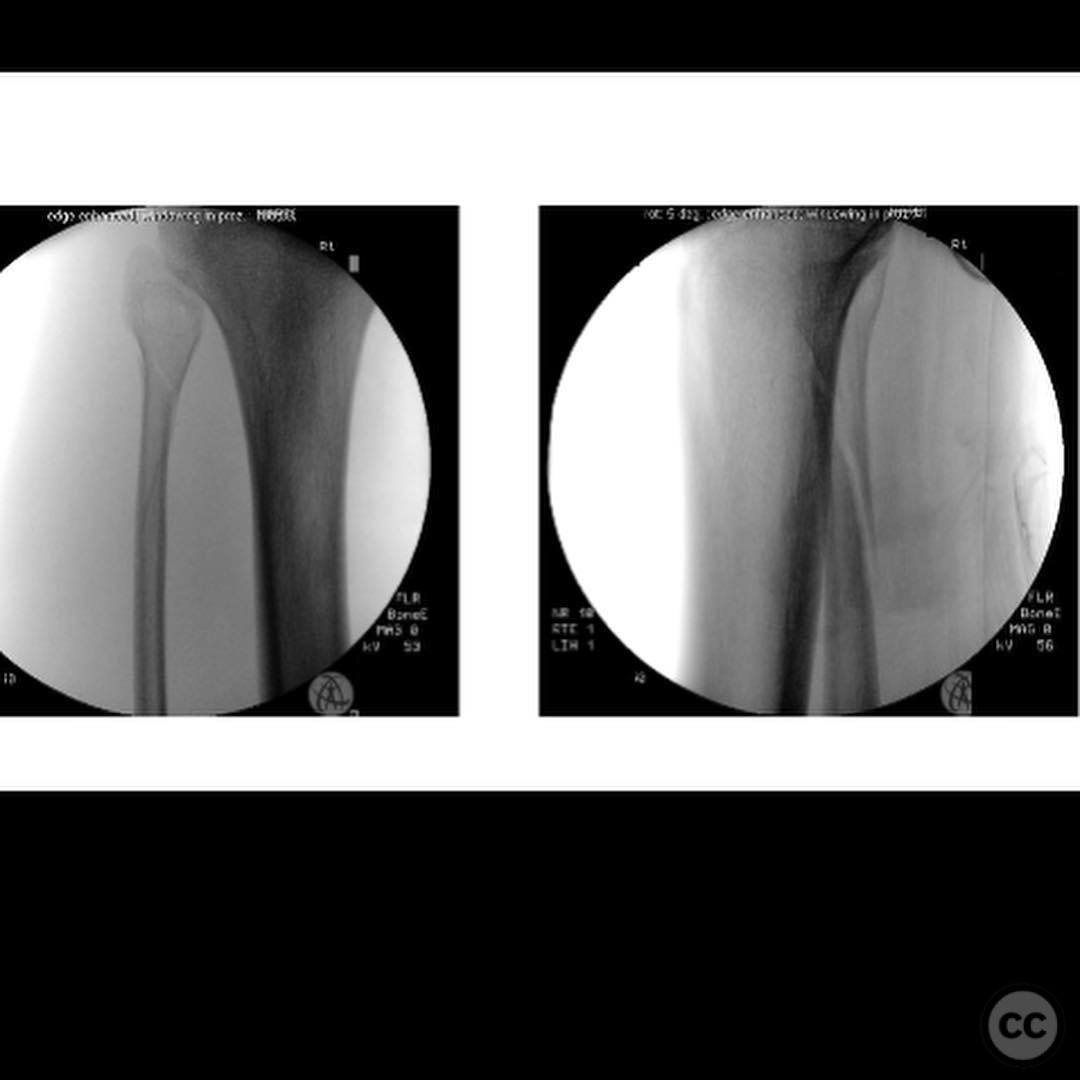
Clinical and radiological findings: A 19-year-old male sustained a fall while skateboarding, resulting in a Maisonneuve fracture with associated syndesmotic injury. Initial clinical examination revealed significant pain and swelling around the ankle joint, with no neurovascular compromise. Radiographic evaluation, including standard anteroposterior, lateral, and mortise views of the ankle, confirmed the presence of a high fibular fracture and widening of the syndesmosis. The contralateral uninjured side was imaged to serve as a reference for anatomical reduction.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction of the syndesmosis using a direct approach to visualize the confluence of tibial, fibular, and talar cartilage. The plan included fixation of the fibula to restore length and rotation, followed by syndesmotic stabilization using quad cortical screws.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the injured leg draped freely to allow manipulation and access to both the ankle and proximal fibula.
Anatomical surgical approach: A longitudinal incision was made over the lateral aspect of the ankle to expose the distal fibula and syndesmosis. Subperiosteal dissection was performed to access the fibula and syndesmotic region. An open reduction was achieved by direct visualization of the tibial, fibular, and talar cartilage confluence. A separate incision was made proximally to address the fibular fracture.
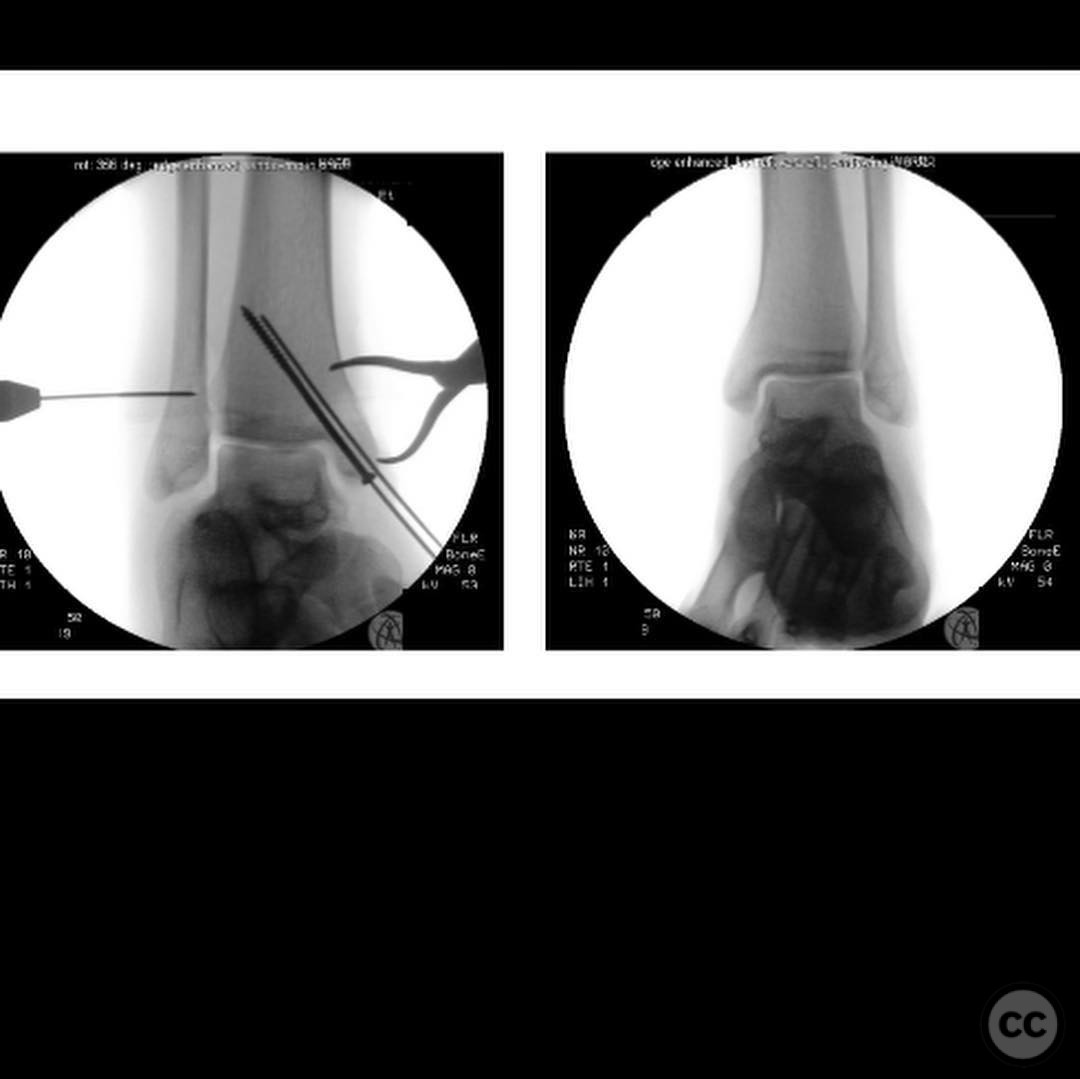
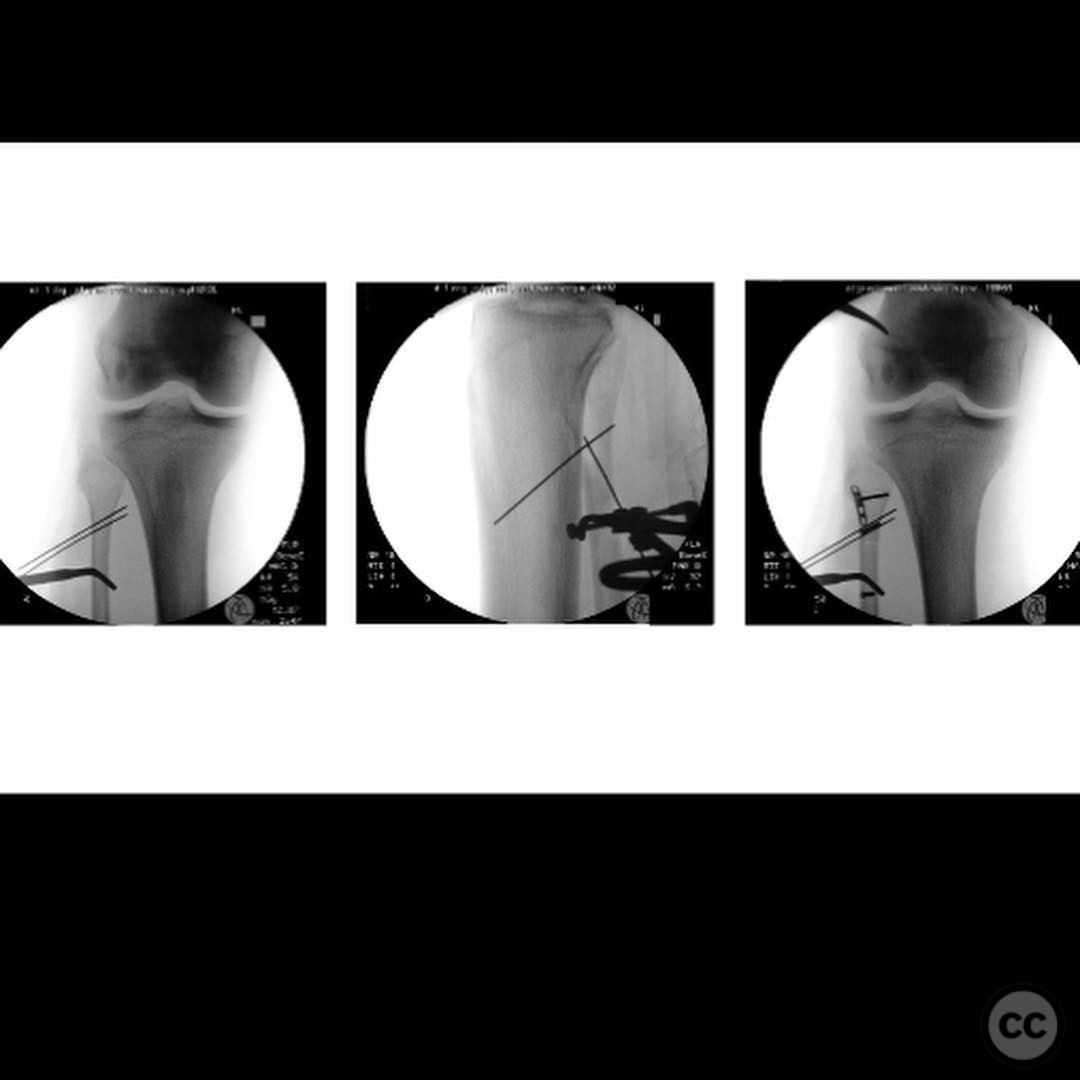
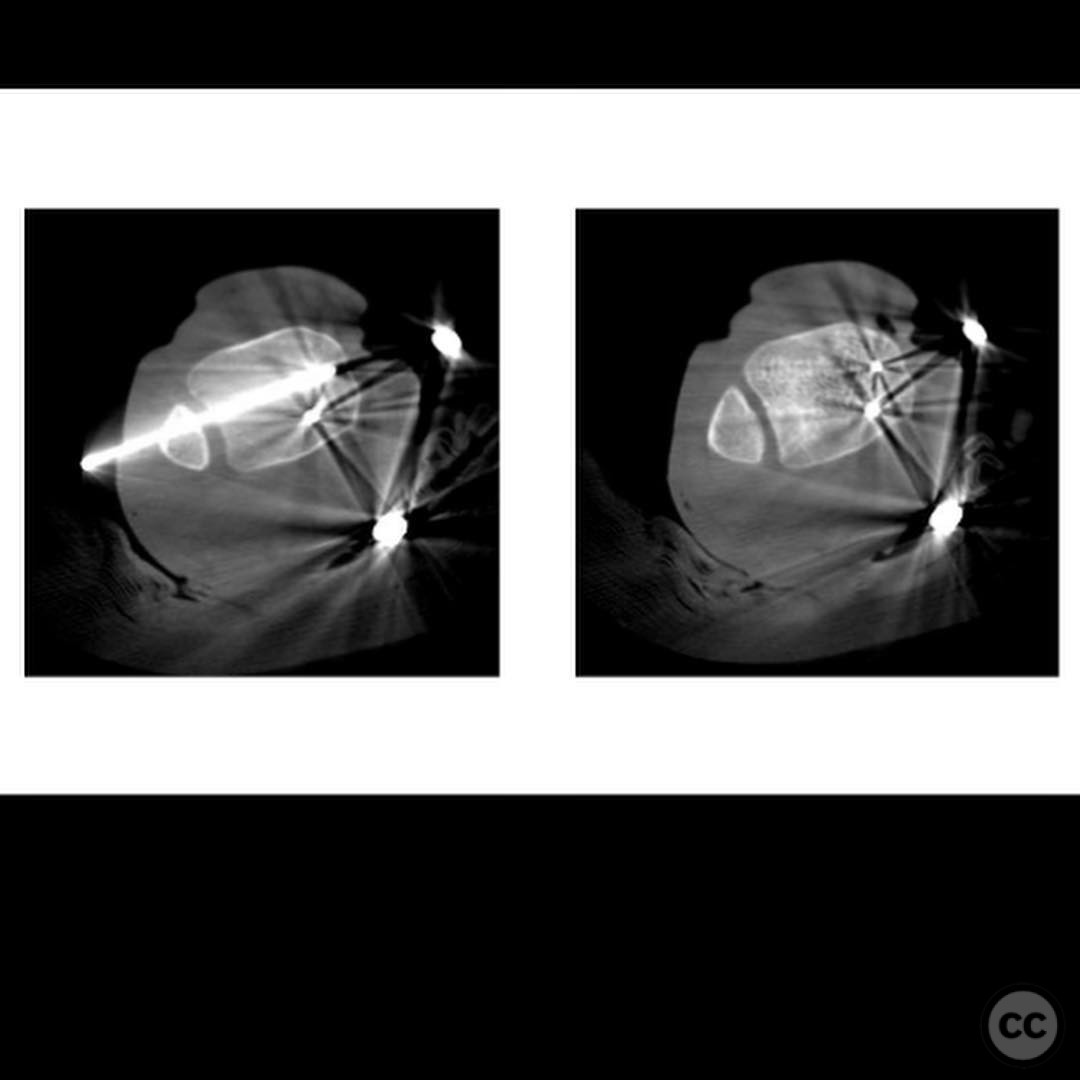
Operative remarks:The surgeon emphasized the importance of achieving an anatomical reduction of the syndesmosis, using a thumb reduction technique rather than clamping to minimize malreduction risk. The fibula was fixed first to ensure proper length and rotation, followed by syndesmotic stabilization with two quad cortical screws. Intraoperative imaging, including fluoroscopy and O-arm, confirmed satisfactory reduction and fixation.
Postoperative protocol: The postoperative rehabilitation protocol included 10 weeks of non-weight bearing, with initiation of ankle and subtalar joint motion exercises at 2 weeks post-surgery. The decision to retain or remove the screws was based on patient preference regarding discomfort.
Follow up: Not specified.
Orthopaedic implants used: Quad cortical screws for syndesmotic stabilization.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1062 times
23 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Maisonneuve Fracture with Syndesmotic Injury.. Journal of Orthopaedic Surgery and Traumatology. Case Report 33375327 Published Online Jul 23 2025.