










Ballistic Distal Humerus Fracture with Segmental Lateral Column Bone Loss.
Score and Comment on this Case
Clinical Details
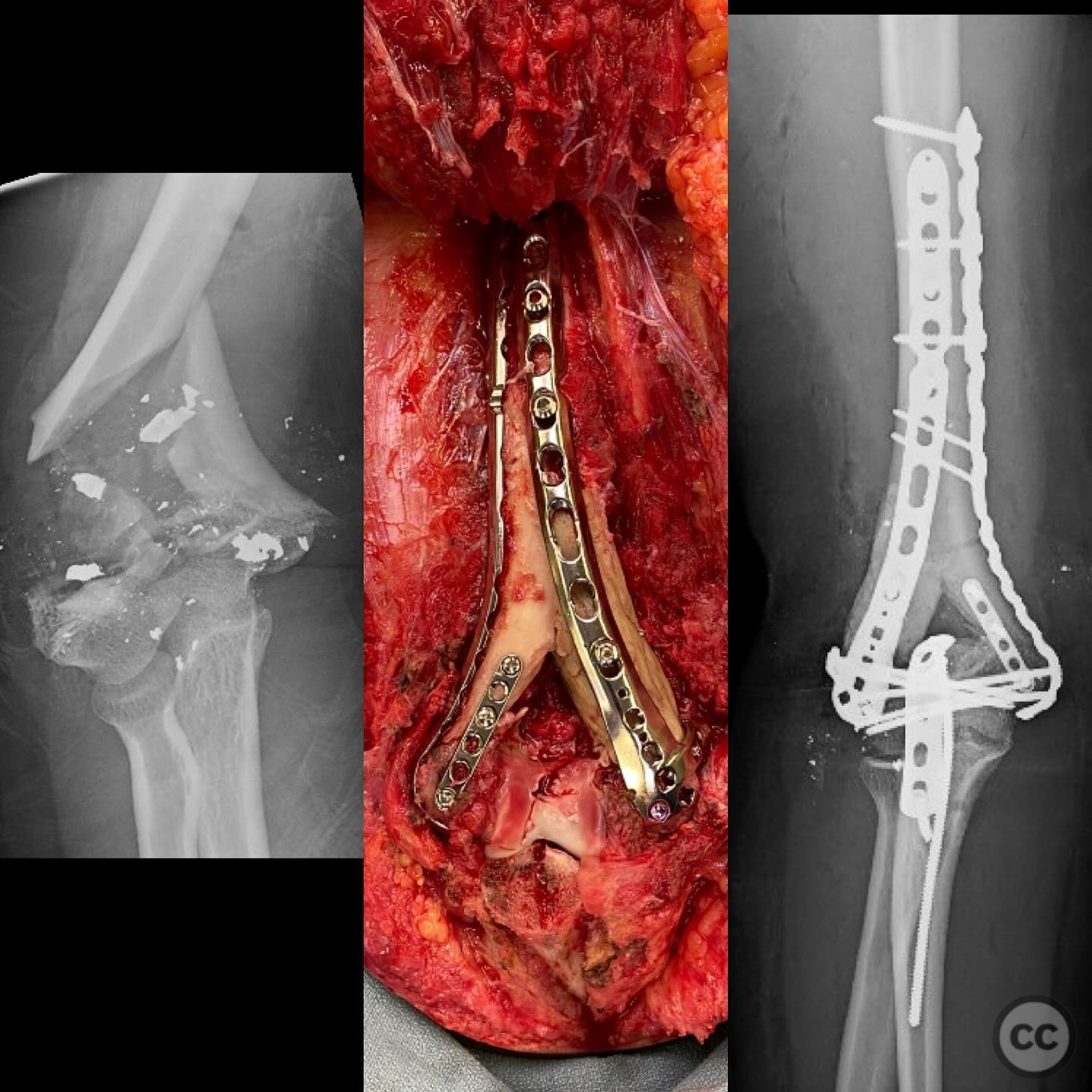
Clinical and radiological findings: The patient presented with an isolated distal humerus fracture resulting from a low velocity projectile. There was no vascular injury noted. Neurological examination revealed variable abnormalities in the radial and ulnar nerves, while the median nerve examination was normal. The fracture was characterized by segmental bone loss in the lateral column.
Preoperative Plan
Planning remarks: The preoperative plan involved a thorough debridement followed by primary open reduction and internal fixation. An anterolateral approach to the distal humerus was anticipated to address the fracture and associated bone loss.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected arm placed on a radiolucent arm board to allow for optimal access and imaging during the procedure.
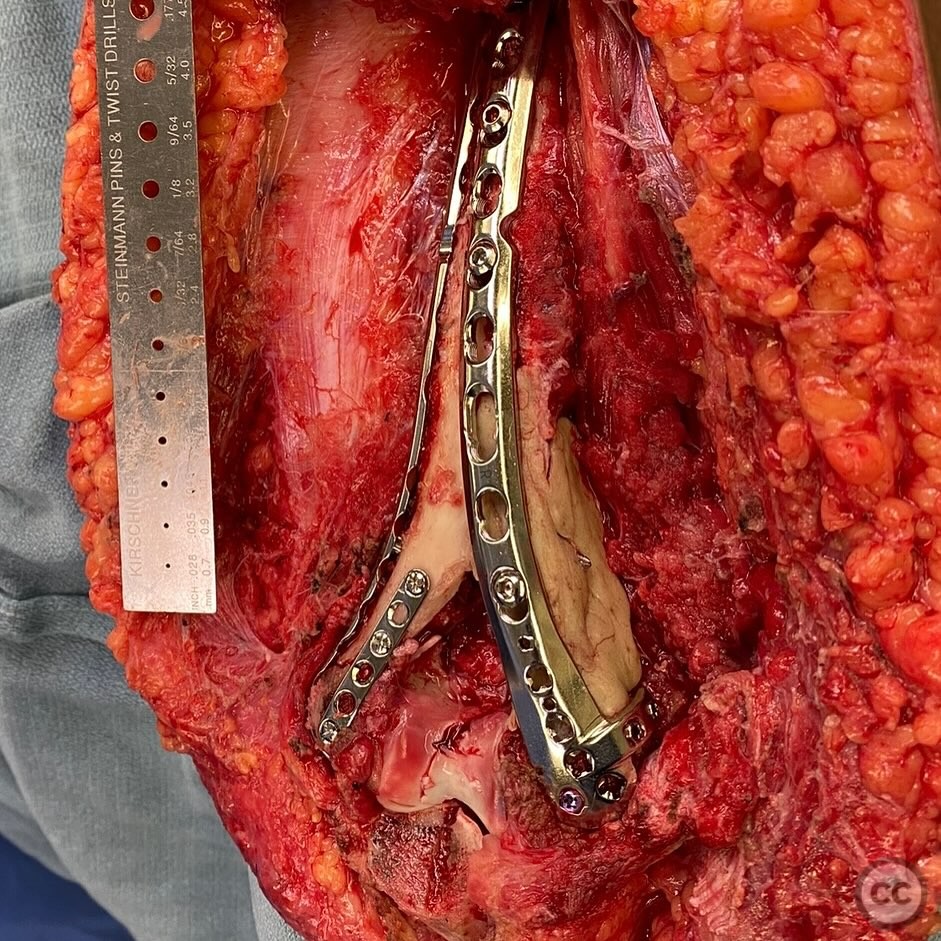
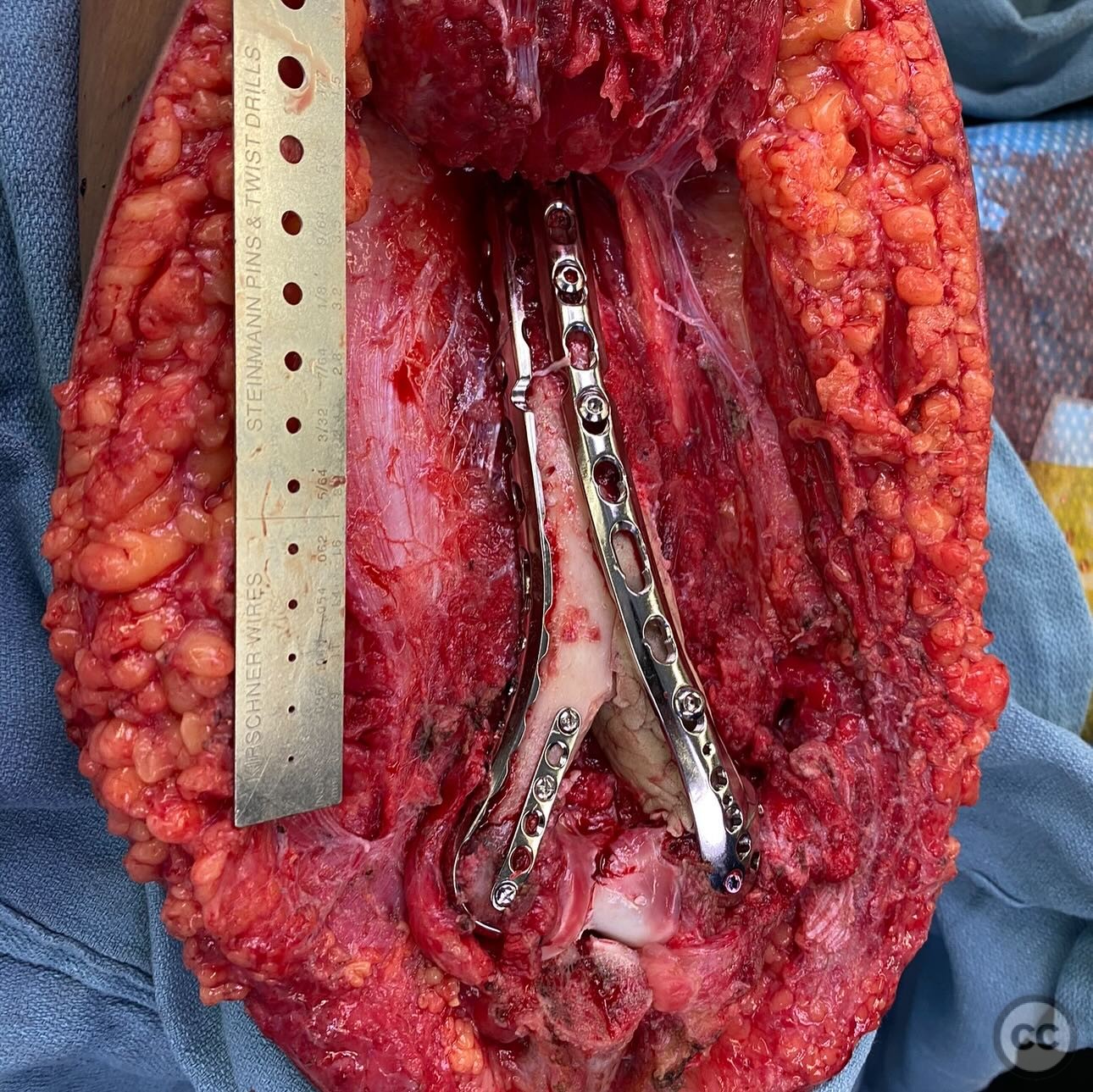
Anatomical surgical approach: A longitudinal posterior approach to the distal humerus was utilized. The incision extended from the lateral epicondyle proximally along the humeral shaft. Careful dissection was performed to expose the fracture site while preserving neurovascular structures. Gel foam was used in the olecranon fossa to maintain its integrity during reconstruction.
Operative remarks:The segmental bone loss in the lateral column posed a significant challenge in restoring the normal carrying angle and rotation of the elbow. An intraoperative consultation with a plastic surgeon was obtained for management of the segmental ulnar nerve loss, resulting in a plan for delayed cable grafting and distal nerve transfer. The induced membrane technique (IMT) was chosen to manage the bone defect, with plans for a second stage IMT and nerve reconstruction approximately three months post-initial ORIF. An AP radiograph of the contralateral elbow was used intraoperatively to guide restoration of column length and carrying angle.
Postoperative protocol: Early mobilization was emphasized postoperatively to prevent stiffness and maintain joint function. A rehabilitation protocol involving active range of motion exercises was initiated soon after surgery.
Follow up: At 18 months post-surgery, the patient achieved a motion arc of 5-130 degrees and demonstrated restored ulnar motor and sensory function with mild weakness.
Orthopaedic implants used: Orthopaedic implants used included antibiotic-loaded PMMA cement spacer and internal fixation hardware for ORIF.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (2)
Guest User
Well done
Dr Ed Oates
Impressive surgery, especially considering it was done in the index procedure