















Distal Tibia Fracture with Underlying Vascular Disease and Chronic Ankle Deformity: Salvage with Circular Frame after IM Nail Failure
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 42-year-old male presented following a skateboarding accident with a distal third tibial fracture and a concomitant fibular fracture at the same level. The patient had a history of previous ankle trauma resulting in deformity and arthrosis. Notably, the patient exhibited significant skin changes indicative of undiagnosed peripheral vascular disease, resembling venous stasis. Initial radiographs confirmed the fracture pattern, and clinical examination highlighted the compromised soft tissue envelope.
Preoperative Plan
Planning remarks: The preoperative plan involved closed or percutaneous clamping for reduction, followed by intramedullary nailing of the tibia while leaving the fibula unfixed due to soft tissue concerns. The intention was to stabilize the tibial fracture, optimize the patient's vascular condition, and address the chronic ankle problem electively at a later stage.
Surgical Discussion
Patient positioning: Supine positioning was utilized for the procedure, allowing access for closed reduction and intramedullary nailing.
Anatomical surgical approach: A minimally invasive approach was employed for intramedullary nailing of the tibia. This involved small incisions for guidewire insertion and nail placement, avoiding extensive dissection to preserve the compromised soft tissue envelope.
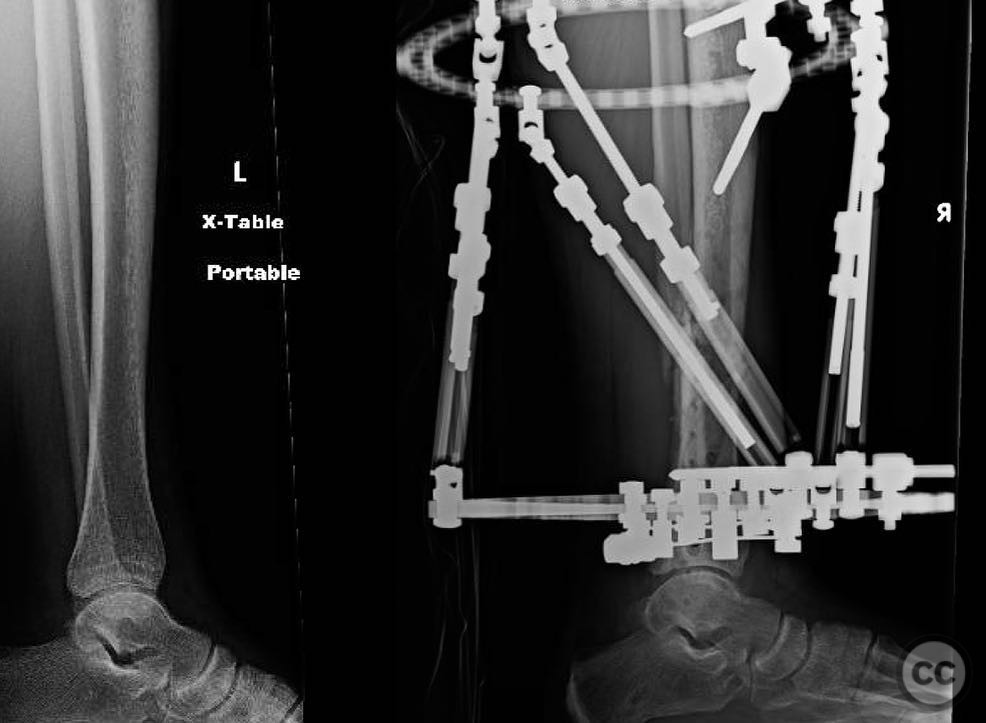
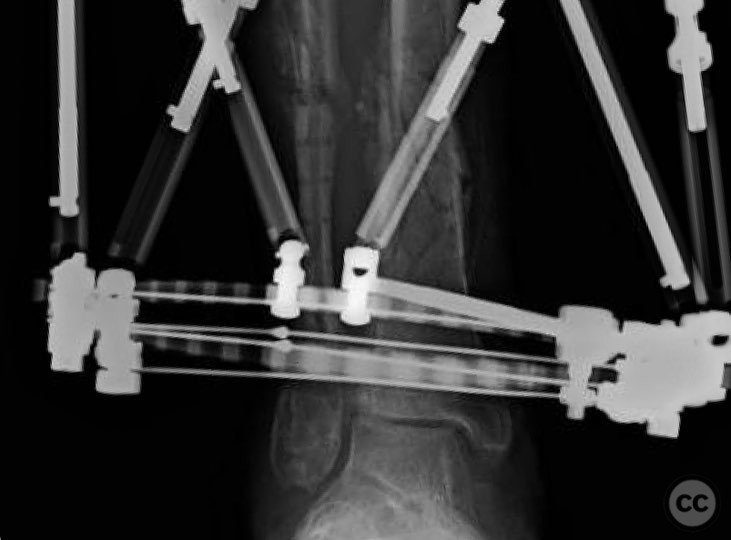
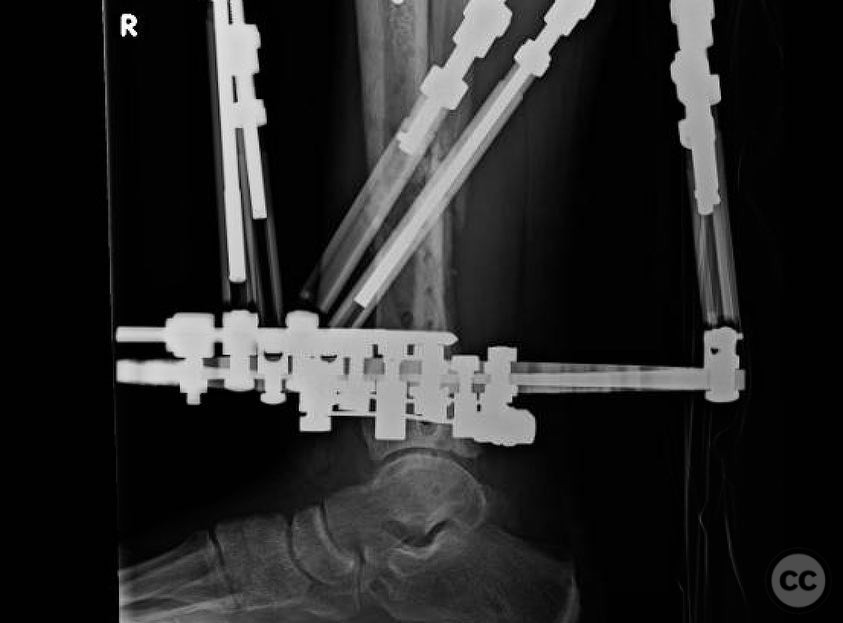
Operative remarks:Initial management failed at six weeks postoperatively, with valgus collapse and medial wound development, suggesting infection in the context of peripheral vascular disease. The decision was made to remove all implants, perform debridement, ream the canal, and initiate a two-week course of intravenous antibiotics. A tensioned fine wire frame was applied to manage the septic nonunion and deformity. The frame included fibular osteotomy and lengthening, syndesmosis takedown for planned arthrodesis, and medial gutter debridement. Olive wires were used to correct deformity acutely in the operating room, and the frame was locked statically.
Postoperative protocol: The patient remained non-weight bearing until surgical and medial wounds healed at six weeks. Weight-bearing was then allowed, with dynamization of the frame at five months and removal at six and a half months.
Follow up: Not specified.
Orthopaedic implants used: Intramedullary nail, tensioned fine wire frame with olive wires.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 314 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Distal Tibia Fracture with Underlying Vascular Disease and Chronic Ankle Deformity: Salvage with Circular Frame after IM Nail Failure. Journal of Orthopaedic Surgery and Traumatology. Case Report 31482184 Published Online Jul 21 2025.