










Trans-symphyseal Screw Fixation for Unstable Superior Pubic Ramus Fracture
Score and Comment on this Case
Clinical Details
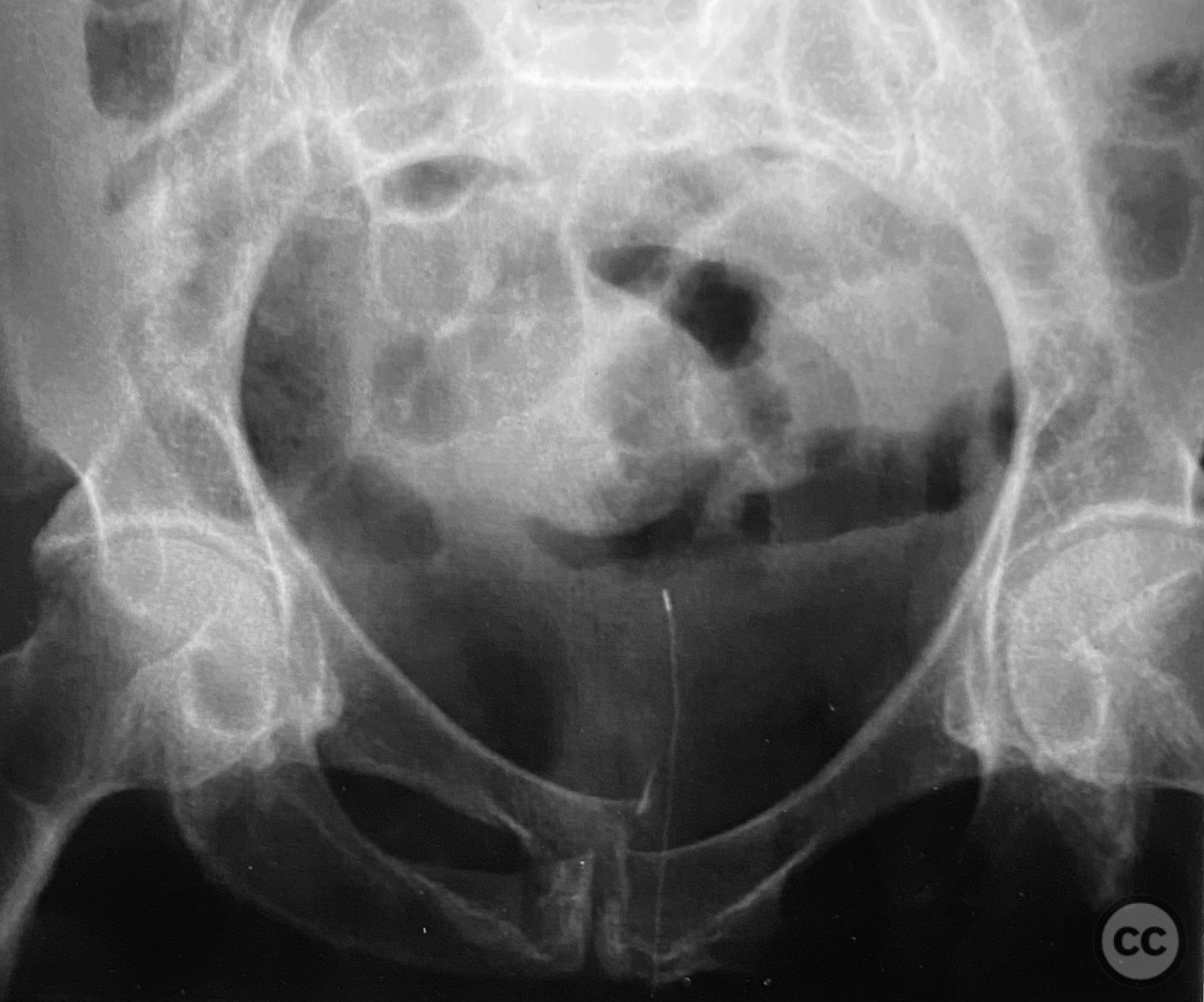
Clinical and radiological findings: Adult patient presenting with severe pelvic pain, unable to sit or transfer to a chair. Clinical examination under anesthesia demonstrated pelvic instability with “rebound reduction” upon minimal iliac crest compression. Imaging revealed an unstable superior pubic ramus fracture with challenging anterior pelvic bone anatomy and dense cortical bone at the anterior acetabular wall.
Preoperative Plan
Planning remarks: Planned trans-symphyseal fixation of the superior pubic ramus fracture using a 4.5mm cortical screw, with preoperative intent to maximize implant purchase in stable bone regions. Surgical approach selected to facilitate direct access to the superior pubic ramus and symphysis pubis.
Surgical Discussion
Patient positioning: Supine position on a radiolucent table, allowing intraoperative fluoroscopic imaging of the pelvis.
Anatomical surgical approach: Pfannenstiel (transverse suprapubic) incision made approximately 2cm above the symphysis pubis. Dissection carried through subcutaneous tissue and rectus sheath, with blunt separation of rectus abdominis muscles to expose the symphysis pubis and superior pubic ramus. Periosteal elevator used for subperiosteal exposure of the superior pubic ramus, maintaining careful retraction of neurovascular structures.
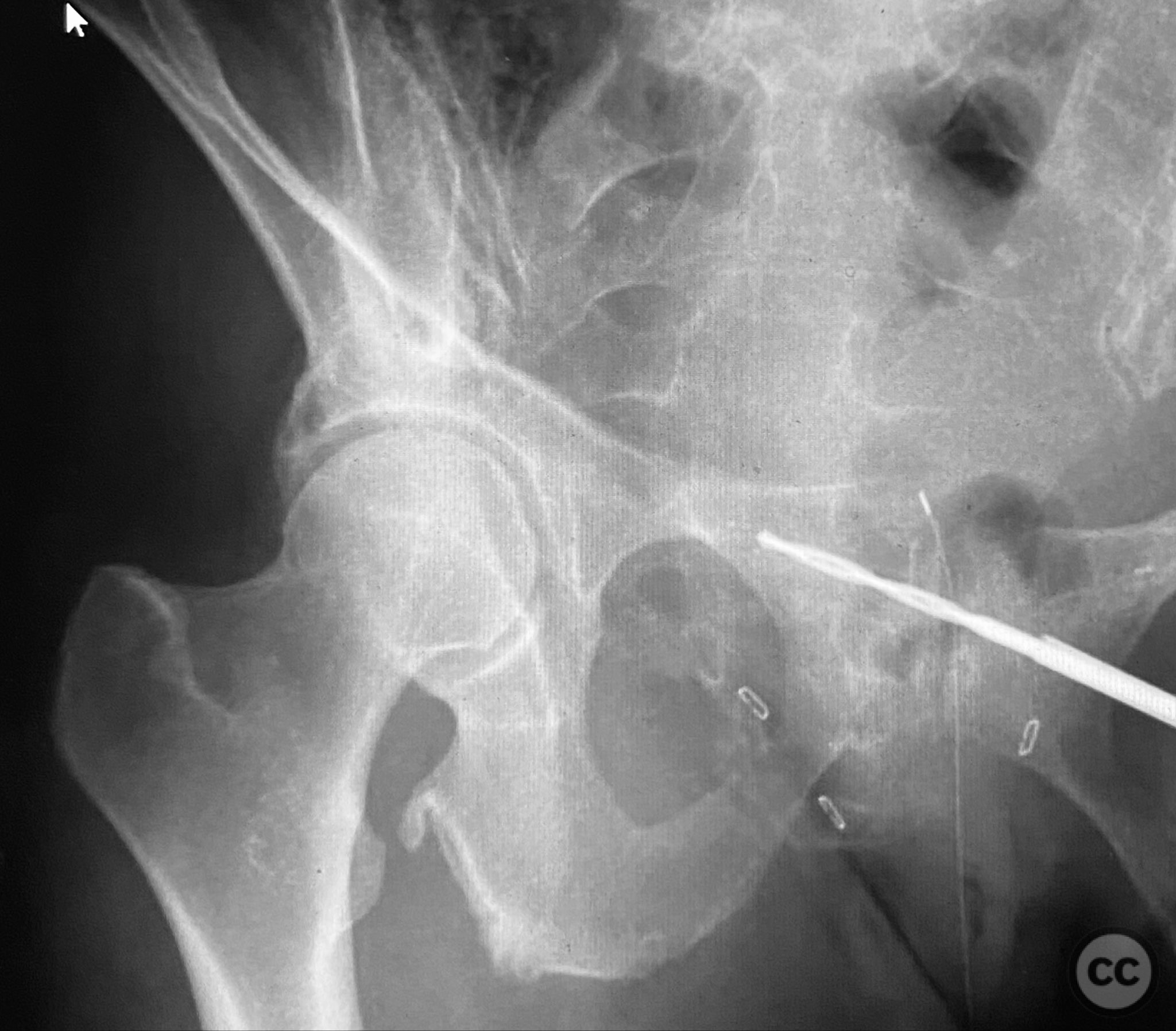
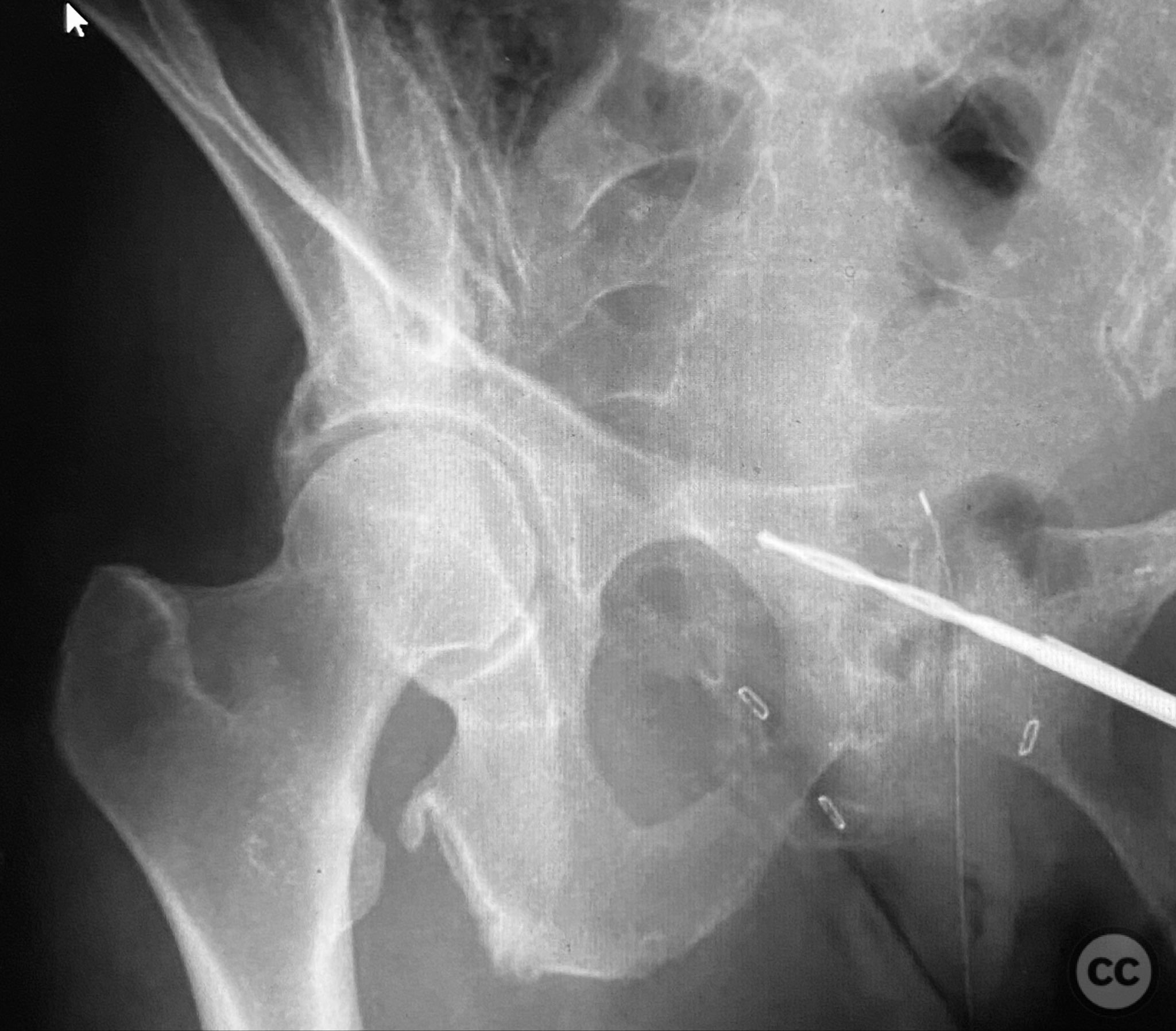
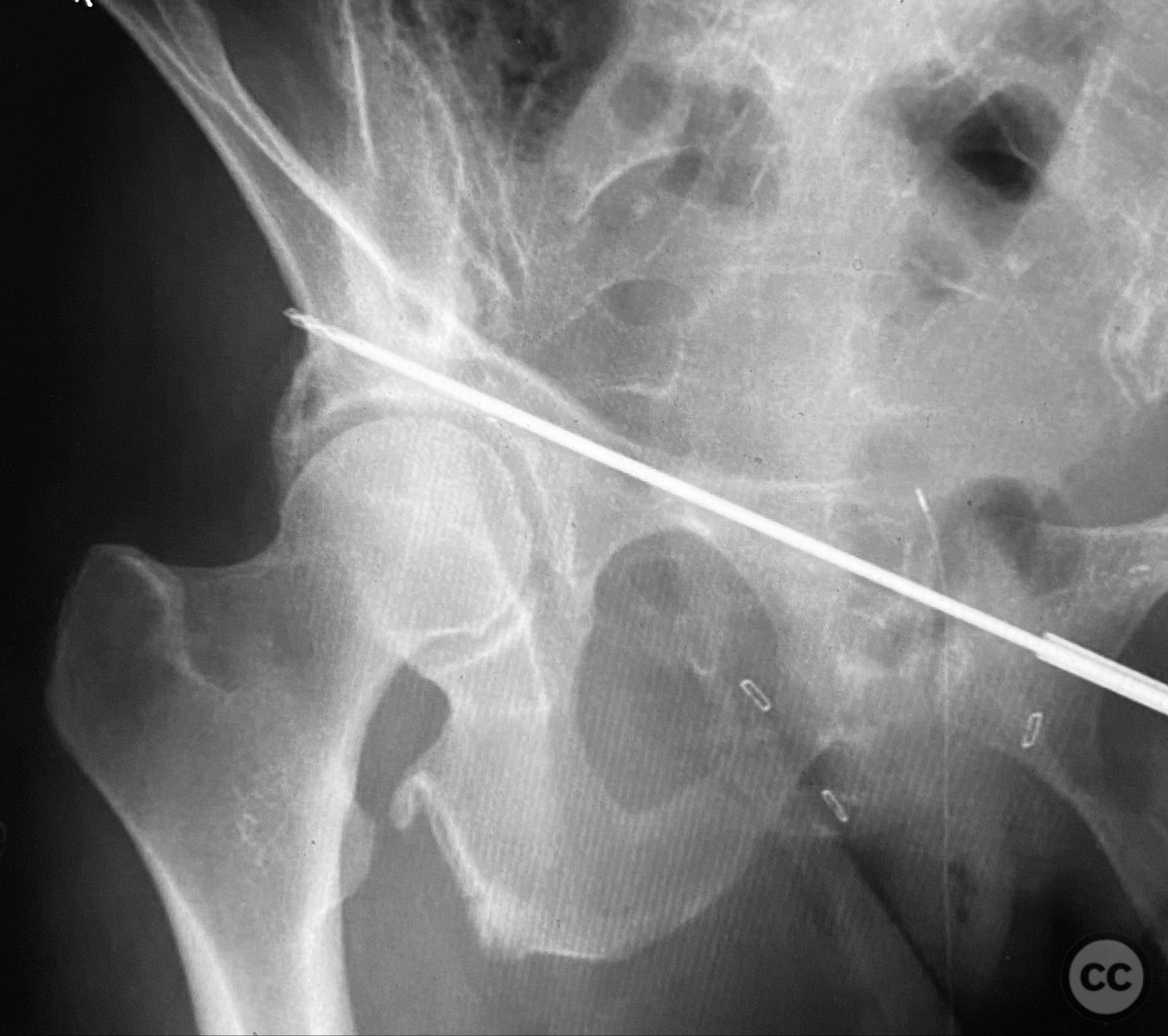
Operative remarks:Intraoperatively, a 3.5mm drill was used through a protective sleeve to initiate the screw pathway across the superior pubic ramus. Due to poor bone quality, a 2.5mm drill was subsequently employed; however, resistance was encountered as the drill tip engaged the dense cortical apex of the anterior acetabular wall. The drill became lodged in this region. To avoid drill breakage, manual extraction using pliers was considered; however, the surgeon elected to carefully deflect and advance the drill manually, successfully completing the pathway. Screw length was measured directly from the embedded drill tip. A 4.5mm cortical screw was then inserted trans-symphyseally along the prepared medullary canal, achieving stabilization of the unstable ramus fracture. Postoperative CT confirmed appropriate screw trajectory and demonstrated the dense cortical bone at the anterior acetabular wall where the drill tip had engaged.
Postoperative protocol: Early mobilization as tolerated with protected weight bearing, avoidance of forced hip abduction or external rotation for 6 weeks, and progressive increase in activity as pain allows.
Follow up: Not specified
Orthopaedic implants used: 4.5mm cortical screw
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 455 times
11 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Trans-symphyseal Screw Fixation for Unstable Superior Pubic Ramus Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 30654218 Published Online Sep 11 2025.