






Posterior Wall Acetabular Fracture with Incarcerated Chondral Fragment and Hip Joint Asymmetry
Score and Comment on this Case
Clinical Details
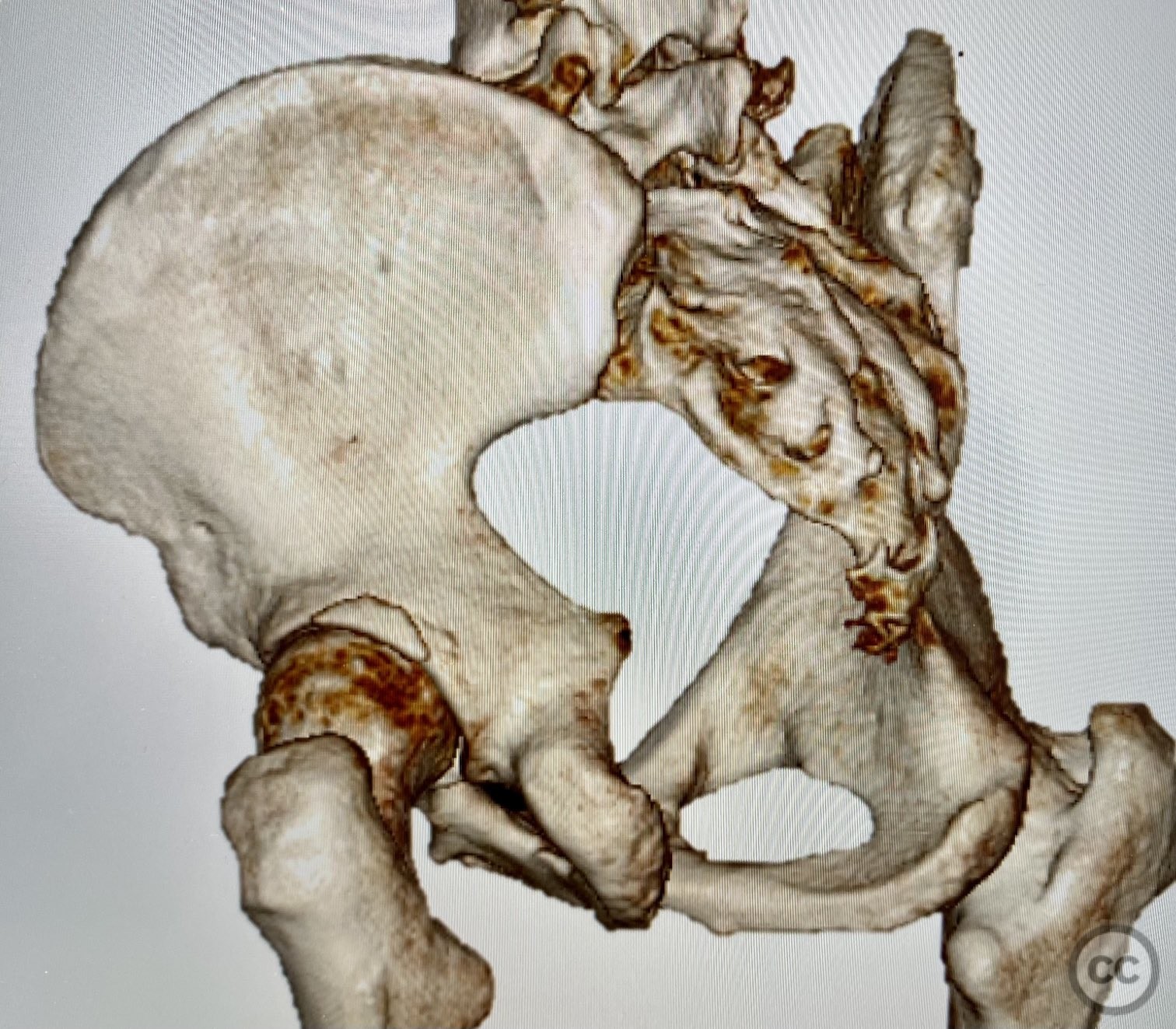
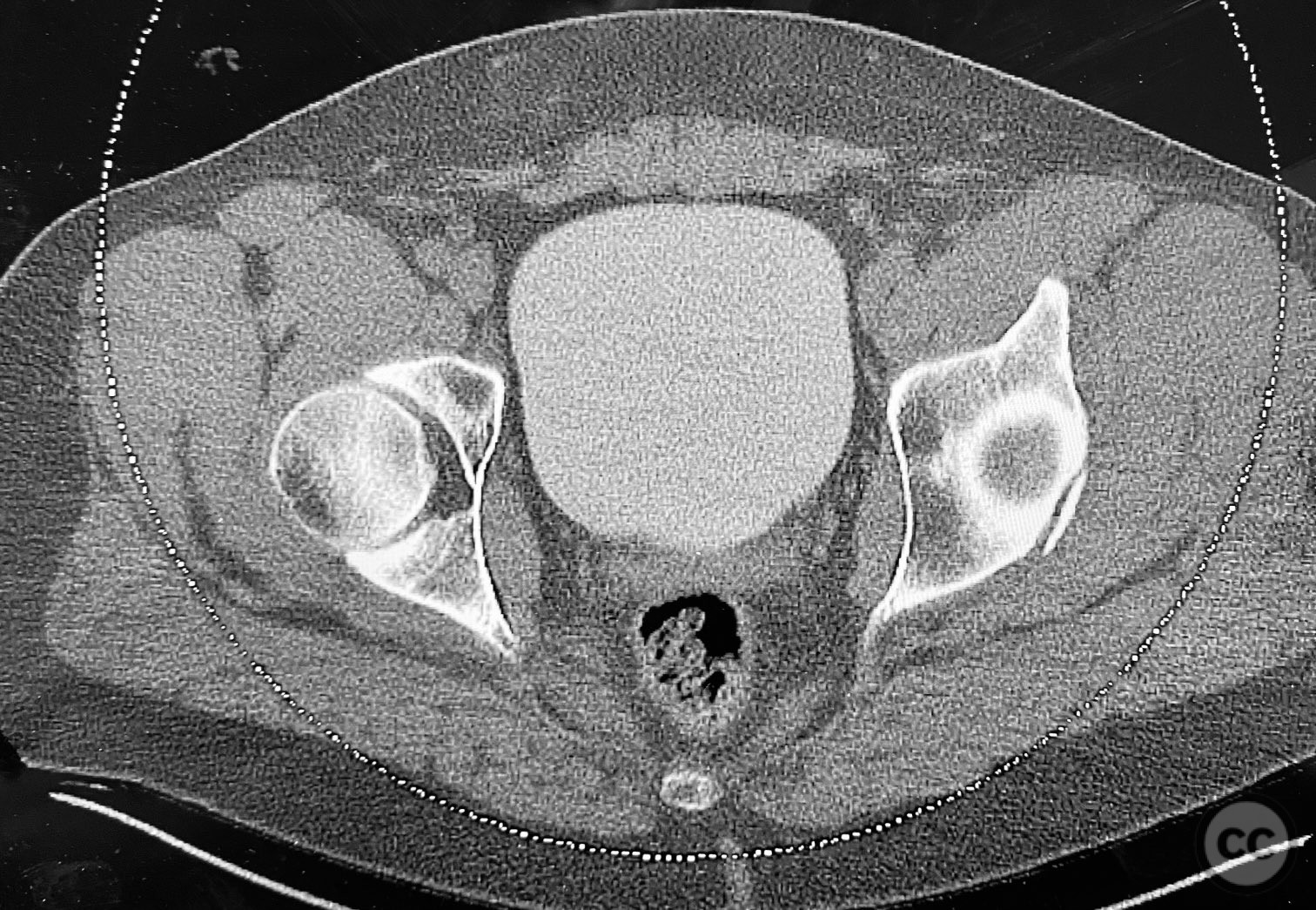
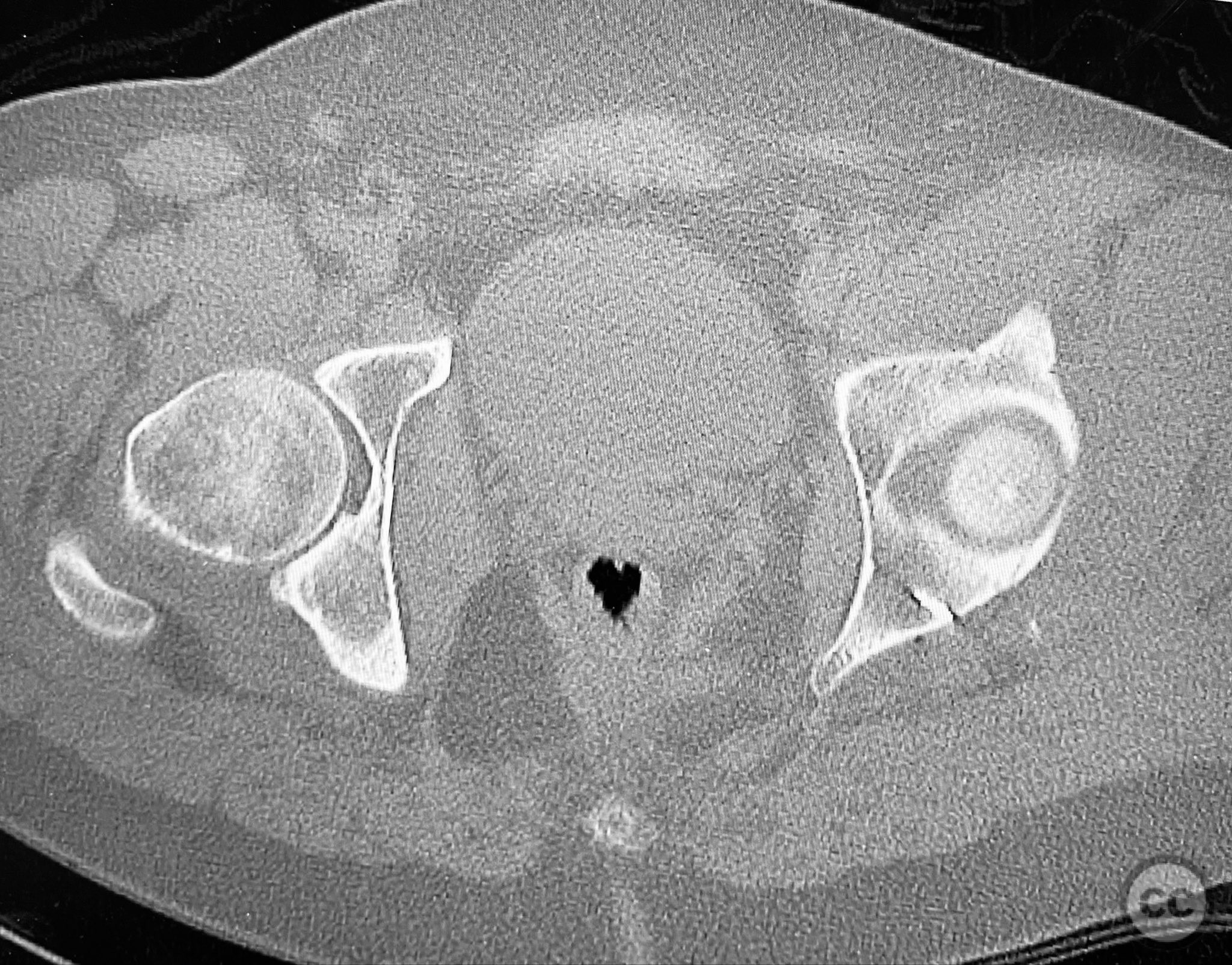
Clinical and radiological findings: A patient involved in a motor vehicle collision presented with left hip pain exacerbated by any attempted movement. Initial axial and surface-rendered computed tomography (CT) imaging demonstrated an essentially nondisplaced posterior wall (PW) acetabular fracture (AO/OTA 62-A1.1). However, the anteroposterior (AP) scan image and coronal reconstructions revealed significant hip joint asymmetry. Examination under anesthesia with fluoroscopic guidance confirmed persistent joint incongruity, with the femoral head subluxating posteriorly at 50–60 degrees of flexion. A pure chondral fragment was identified as being interposed between the femoral head and the intact region of the posterior wall, accounting for the clinical and radiological asymmetry.
Preoperative Plan
Planning remarks: The preoperative plan was to perform an open reduction and internal fixation of the posterior wall acetabular fracture via a Kocher-Langenbeck approach, with intraoperative assessment and removal of any intra-articular loose bodies or chondral fragments, followed by stabilization of the posterior wall fragment using suture anchor fixation.
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position to facilitate posterior access to the acetabulum.
Anatomical surgical approach: A Kocher-Langenbeck approach was utilized, involving a longitudinal incision centered over the greater trochanter, with dissection through the fascia lata and splitting of the gluteus maximus muscle. The short external rotators were identified and retracted, and the hip capsule was exposed and incised to allow direct visualization of the posterior wall of the acetabulum. The incarcerated chondral fragment was identified and removed from the joint space. The posterior wall fracture fragment, which remained attached to the capsule, was anatomically reduced and stabilized using suture anchors placed into the acetabular rim.
Operative remarks:Intraoperatively, persistent hip joint asymmetry was noted on fluoroscopic imaging, correlating with preoperative findings. The femoral head exhibited posterior subluxation at moderate flexion angles due to mechanical obstruction by a pure chondral fragment wedged between the femoral head and posterior wall. Removal of this fragment restored joint congruity and symmetry. The posterior wall fracture, though minimally displaced, was deemed unstable based on intraoperative assessment and fluoroscopic stress testing. The fragment’s capsular attachment facilitated stabilization using suture anchor repair. The use of a Kocher-Langenbeck approach was considered essential for adequate exposure, reduction, and stabilization; arthroscopic techniques were not employed.
Postoperative protocol: Postoperatively, the patient was maintained toe-touch weight bearing on the affected limb for six weeks. Passive range of motion exercises were initiated immediately, avoiding flexion beyond 60 degrees for four weeks. Active-assisted range of motion was introduced at week four, with progression to partial weight bearing at week six and full weight bearing by week ten, contingent on radiographic evidence of healing.
Follow up: Not specified
Orthopaedic implants used: Suture anchors (acetabular rim fixation)
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 271 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Posterior Wall Acetabular Fracture with Incarcerated Chondral Fragment and Hip Joint Asymmetry. Journal of Orthopaedic Surgery and Traumatology. Case Report 29288697 Published Online Sep 12 2025.